

Is a Hot Pack or Cold Treatment Better for Your Low Back Pain?

An ice bag or very cold pack may numb the pain in your back, but does this also promote healing?
Heat won’t numb the pain, but won’t it increase blood flow to your hurting muscles?
So the big question is: Heat or cold for back pain treatment?
Keep in mind that in most cases, back pain will resolve all by itself, says Kaixuan Liu, MD, PhD, nationally distinguished leader in endoscopic spine surgery; and chief surgeon at Atlantic Spinal Care in Edison, N.J.
This good fortune may occur only two weeks after the initial onset of pain. Both cold and heat can be applied — but not in a random way.
To determine whether you should use heat or cold to treat low back pain, Dr. Liu says it’s important to learn what’s causing the situation.
Sudden-onset of pain in the lower back can be caused by improperly lifting something heavy or by some kind of forceful trauma.
“With a mechanical injury, you might feel anything from dull aching to a shooting or stabbing pain,” says Dr. Liu.
“You might also experience stiffness or loss of flexibility that prevents you from standing or sitting normally.” Discomfort that’s acute is short-lived, but it may recur as well.
If the issue goes on for over 90 days, this is then “chronic” low back pain. It can be caused by improper lifting but also degenerative ailments.
Heat vs. Cold to Treat Low Back Pain
“It’s all about inflammation,” says Dr. Liu. An acute injury causes inflammation–which results in more blood going to the site of the injury, plus immune cells coming to the rescue.
“In the case of acute muscle or joint injury, or surgery,” says Dr. Liu, “it creates swelling that is the beginning of a healing process.” This beneficial response, though, can cause a lot of pain.
For acute inflammation, use ice, recommends Dr. Liu. “The cold shrinks small blood vessels in the area, which keeps blood and other fluids from flooding to the injury site, decreasing swelling.”
It also slows down nerve impulses at the site. This will intercept transmission of pain signals, numbing the area “like a local anesthetic.” Cold also helps reduce damage to tissue that the acute inflammation can trigger.
A heat application promotes blood circulation, and this will lessen pain. However, heat pads are not a smart choice for acute inflammation because the heat can worsen the swelling and even cause more pain.
If there is no inflammation of a chronic nature, you should use heat for your lower back pain to open up blood vessels.
This will promote healing via the increased nutrients and oxygen to the site and will stimulate the nerves — which means interrupted pain signals.
Throwing Out Your Back with the Wrong Movement
You’re moving furniture or some similar activity when suddenly, your back “goes out.” Dr. Liu says you should apply ice, as this is an acute injury. Apply for 15 to 20 minutes three to four times a day for one to two weeks.
After a few weeks switch to heat–for 15 to 20 minutes three to four times daily. It’s important to let at least two hours pass between either form of therapy sessions.
And by the way, the heat source should not be so hot that it’s uncomfortable or cause any kind of burning to the skin.
In fact, for either heat or ice, the source should not be directly against your bare skin, but rather, separated by some kind of fabric.
“There’s a popular myth out there that heat and cold are interchangeable in treating back pain,” says Dr. Liu.
“It’s true that they both relieve pain, but mechanisms that produce the pain relief are completely different. That means each has its time and place.”
 Dr. Liu specializes in disc herniations, spinal stenosis, spondylolisthesis, and mitigating failed neck and back surgery, among many other conditions that affect the neck, mid and lower back.
Dr. Liu specializes in disc herniations, spinal stenosis, spondylolisthesis, and mitigating failed neck and back surgery, among many other conditions that affect the neck, mid and lower back.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik/shayne_ch13

Does Shoulder Pain Wake You at Night? Solutions

Shoulder pain at night can prevent even a few good hours of sleep, so here are some things you can do to fight and maybe prevent shoulder pain that strikes at night while you’re asleep.
“There are a few very important steps to take if rotator cuff tendinitis is waking you at night,” says Dr. Joseph J. Ruane, a sports medicine specialist with OhioHealth Physician Group.
The first is to make sure you’ve been diagnosed and that it is indeed a rotator cuff problem.
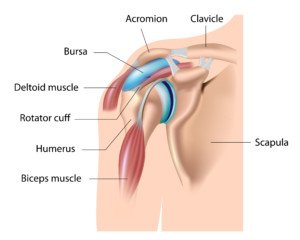
“Rotator cuff tendinitis is especially tricky in that the most common presenting symptom is a deep ache in the middle of your upper arm; often in the bicep region or at the end of the deltoid muscle.
This is called referred pain. While the pain is actually in the middle of your arm, the problem is coming from deep in your shoulder.”
The rotator cuff consists of four muscles and their tendons. These tendons can easily end up irritated from improper lifting technique or insufficient warm-up preceding heavy lifting.
Dr. Ruane continues: “The second step to successful sleep is getting the right treatment once the problem has been identified.
Rotator cuff tendinitis responds well to many common treatment modalities.
Physical therapy, tried and true, remains the best intervention for rotator cuff tendinitis.
There are 26 muscles that are responsible for proper shoulder function.
If just one or two of those are not working properly, shoulder motion becomes unsynchronized and rotator cuff tendinitis can develop.
It is like a car engine – when just one cylinder is not firing on time, the entire engine runs poorly.
Physical therapists are the mechanics of the body and can get your ‘shoulder engine’ running properly again, and eliminate that gnawing pain in your arm.”
An hour before bedtime, says Dr. Ruane, take an anti-inflammatory such as ibuprofen (Advil) or Aleve.
Often, a person suffering shoulder pain at night will point out that the bad shoulder is the side he or she sleeps on.
To help resolve night-time shoulder pain, you must change your sleeping position habits. Yes, this can be done.
“If you like falling asleep on your right side, and the right shoulder is the one with tendinitis, force yourself to fall asleep on your back or on your left side for one week,” says Dr. Ruane.
“You’ll be surprised how easy it is to change the habit, especially once the pain does not disrupt you just an hour or two after falling asleep.
“And another thing – you know your favorite position of falling asleep on your stomach with your arm tucked up under your pillow? It has got to go – pronto!
“That sleeping position alone can be the cause of rotator cuff tendinitis, and is a nasty position for a shoulder that already has it.”
Try these changes and see if they don’t help diminish shoulder pain at night.
 Dr. Ruane’s practice is dedicated to comprehensive, nonsurgical musculoskeletal care. He is active in clinical research and is a nationally recognized speaker and educator.
Dr. Ruane’s practice is dedicated to comprehensive, nonsurgical musculoskeletal care. He is active in clinical research and is a nationally recognized speaker and educator.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/tab62

Simple and Quick Ganglion Cyst Pain Exercises

These ganglion cyst pain exercises are very simple.
Do you have wrist pain? You may have a ganglion cyst, and I have exercises to relieve ganglion cyst pain.
These ganglion cyst exercises should be done two to three times every day.
I’m a former fitness trainer with a ganglion cyst in my wrist, so I know firsthand that these exercises I’ve designed just for ganglion cysts may help you out.
These exercises won’t cure a ganglion cyst.
The exercises are meant to help relieve pain and better enable you to do things that the ganglion cyst pain is interfering with.
I also once had a client with a wrist ganglion cyst, and she described the pain as “feeling like your wrist is always sprained.”
The ganglion cyst often develops in the top part of the wrist, in the middle or near the middle.
The result is that bending (extending, that is) the wrist produces discomfort.
It may also feel like something’s in there blocking the full range of extension.
And there is: the ganglion cyst. Sometimes you can see the cyst as a little lump if you flex (bend down) the wrist. Pressing on the ganglion cyst may cause pain.
Usually, the pain comes only during certain motions. I can type all day and never know I have a ganglion cyst.
But handstands are out of the question. Standard pushups are out, too.
For pushups I grasp dumbbells or pushup handles rather than use flat hands on the floor, though the discomfort isn’t that bad with flat hands, but who wants any kind of discomfort during a pushup?
For other people with ganglion cysts, they can be really nasty. I recently had a “flare-up” for no good reason and felt pain just doing dumbbell presses. It even hurt doing dumbbell curls.
I said to myself, There MUST be some exercises I can do to get rid of this pain.
So here are some very simple exercises that should definitely alleviate some of the pain from a ganglion cyst.
Upon awakening, before getting out of bed, commit to doing the exercises as you lie comfortably in bed.
Simply flex and extend (bend back and forth) your wrist. But at the bottom and top of each bend, hold for 1-2 seconds and “push” a little, but not to the point of discomfort. Do 20 times each direction.

Wait one minute. Then repeat the routine. However, next, you will do “alphabets” with your wrist.
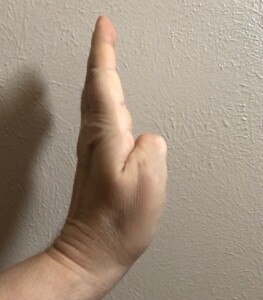
The wrist joint is the pivot. Hold all five fingers rigid, together and straight.
Pretend that the tip of the middle finger is the tip of a pen, and you will be printing every letter of the alphabet in the air — the air being the paper.
Go from A to Z. Do not rush. Make big perfect letters. Move only the wrist joint. Keep elbow and shoulder still.
Afterwards, do the same thing except with numbers up to 20. And that’s the exercise routine.
Repeat the exercises one or two more times throughout the day. You may feel much less pain or discomfort within a few days.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/girl-think-position

Everyday Movement Patterns that Can Hurt the Rotator Cuff, and How to Relieve Pain

Everyday motions can strain the rotator cuff and even prevent healing. You likely don’t even realize when a particular movement is bad for your rotator cuff.
The rotator cuff is a group of four muscles and their delicate tendons.
These muscles enable the shoulder to move in different ways.
Stand with your arms hanging straight at your sides.
Now, slowly lift them up at your sides, keeping them straight, palms facing the floor. Keep shoulders relaxed.
Do you feel pain or anything irksome in one or both shoulders? If so, chances are, this is a rotator cuff problem, mainly with the supraspinatus rotator cuff muscle.
There are other ways to test for a rotator cuff problem, but I won’t go into them here since they are tricky to describe.
However, another classic sign is that when you reach up for something, like grabbing something off the top of the refrigerator or a high shelf, you feel an uncomfortable tweak, ache or pain in your shoulder.
If you lift weights, a rotator cuff problem will be obvious when you do the following exercises: bench press, pushup, behind-the-head shoulder barbell press, and sometimes, wide-grip pull-downs and dumbbell presses (depending on amount of weight).

Freepik.com, ArthurHidden
Everyday movements that can cause, or aggravate, rotator cuff problems.
One: When you feed your arm into a coat arm or jacket arm, your palm faces the floor.
The joint motions here are shoulder internal rotation, and shoulder abduction.

Shutterstock/Milles Studio
These two joint motions in combination “crowd out” the air space at the rotator cuff, and can actually result in the humerus bone of the upper arm making contact with a rotator cuff tendon.
Over time, the bone frays the edge of the tendon. To prevent this, when you feed your arm into an arm hole, do it with 1) your palm up, and 2) your arm as bent as you can.
This creates an opening in the joint, which gives the humerus more room, and thus, it does not contact the tendon.
Two: When you reach for high objects, your palm is facing down. When you hold the object and lower your arm, your palm is facing down or sideways.

Shutterstock/Milles Studio
Again, this palms-down motion crowds out the joint, bringing the humerus bone too close to the tendon.
When you reach up for that jar of pickles or whatever, face the palm to the ceiling.
After grabbing the jar or item, hold it with the palm facing the ceiling as you lower your arm. In other words, always have a palms-up approach.
Three: “Some movements that can put your shoulder muscles at inefficiency can be reaching to put your bag in the back seat [or retrieving something from there] when you’re sitting in the front of the car,” says Dr. Megan McLain, PT, DPT, cofounder of Intuitive Choice Physical Therapy & Wellness in Atlanta, GA.
Similar to this is draping a jacket or sweater over the passenger seat of the car when you’re driving.
In both cases, the rotator cuff will be aggravated most when your palm is down.
This is bad news. It crowds out that glenohumeral space.
Perform these actions with the PALM UP. And keep the arm bent as much as possible.
Additional Movement Patterns that Are Bad for the Rotator Cuff
“Another is lifting an object that is too heavy for one arm like a barrel or heavy groceries that can overload the joint and muscle’s capabilities, straining the rotator cuff,” says Dr. McLain.
“Repetitive overhead work is also a risk factor for rotator cuff tears.
“Also, quick movements like trying to catch a heavy object from falling or yourself from falling also can overload the rotator cuff tendon’s ability to stabilize the joint.”
What’s going on inside the rotator cuff?
The rotator cuff. Shutterstock/Alila Medical Media
“The reason that the glenohumeral space can become crowded is partly because of the way the shoulder is constructed,” says Dr. McLain.
“The head of the humerus is larger than the glenoid fossa, so the rotator cuff and the labrum both help to provide extra stability to the joint.
“Think of it similarly to how chocks can stabilize a whole airplane. Poor posture or overworking a certain group of muscles with repetitive motions can lead to faulty mechanics at the shoulder, which most often leads to the head of the humerus to translate up and forward relative to the glenoid.
“This can lead to something called subacromial impingement, which is the tendons rubbing against the bone and becoming frayed.
“This happens because the bicep and one of the rotator cuff tendons run under the acromion, which is the hook on the side of the shoulder.
“This space gets relatively smaller with poor mechanics and overhead lifting, in particular.”
Strength Training Will Help
“Strength training that can be done to counteract this is for the muscles at the back of the shoulder, meaning the scapular muscles,” says Dr. McLain.
“This can include exercises like bent-over rows and pulling tasks.

Bent-over dumbbell row. George Stepanek
“Also working the biceps and triceps, especially if you do a lot of carrying or lifting, is also important to protect the smaller, stabilizing rotator cuff muscles.
“You should be mindful of your body position and avoid trying to lift objects that are too far away from your body.
“Move closer before lifting and use two hands to evenly distribute forces.”

Another pulling motion, the seated row. Start out with very light weights and gentle motion. Freepik.com yanalya
 Dr. Megan McLain, PT, DPT, puts her clients first while providing one-on-one in-home care. With physical therapy and health coaching services, Dr. McLain addresses all aspects such as physical barriers, mindset, accountability and knowledge that may be impacting the client’s experience.
Dr. Megan McLain, PT, DPT, puts her clients first while providing one-on-one in-home care. With physical therapy and health coaching services, Dr. McLain addresses all aspects such as physical barriers, mindset, accountability and knowledge that may be impacting the client’s experience.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Rustle

Cardio Exercise for Plantar Fasciitis: 3 Aerobic Routines

I’ve had plantar fasciitis and have discovered that you don’t need to limit your cardio exercise routines to the stationary bike with this painful heel condition.
I used to have a very nasty case of plantar fasciitis in both feet, and my first instinct was to just use the stationary bike until the condition resolved.
But why stop at the stationary bike just because you have plantar fasciitis? If you have this condition, then you know that it comes and goes, often without warning.
If you’ve read up about it, or have seen a doctor, then you also know that stretching the bottom of the foot is one of the treatment modalities for this stubborn condition.
Cardio like jogging, step aerobics, dancing, tennis, jump rope and inline skating are not recommended for people with plantar fasciitis, if for no other reason that these activities can bring on searing heel pain.
However, when I had plantar fasciitis, I discovered that walking uphill made it feel better, and of course, uphill walking is a form of cardio exercise.

Shutterstock/G-Stock Studio
I recommend gentle, slow hiking, and do it nearby your car, in case the plantar fasciitis flares up mid-hike. You don’t want this happening when you’re a mile from your car.
If the pain is bad before you start hiking, postpone it. If it’s mild, proceed slowly, but if it gets worse, turn back and postpone the activity.
Hiking or walking uphill, however, should produce largely benefits for plantar fasciitis, as it stretches the plantar fascia.
Remember, stretching this tissue is what doctors recommend anyways, so why not give it some stretching while at the same time getting in some aerobics uphill?
Try walking slowly using a treadmill incline as well. However, walking uphill on a hiking trail may prove to be more beneficial, since the uneven terrain will cause more stretching and motion of the plantar fascia of the foot.
If you use a treadmill, let your arms swing naturally. Holding on will interfere with a normal gait pattern.
If it hurts to use a treadmill, then postpone this activity.
If any cardio activity aggravates your plantar fasciitis, even the stationary bike, then STOP the activity.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Pamela Au
Why an Imminent Heart Attack Causes Shoulder Pain

Ever wonder how a heart attack about to happen can cause shoulder pain?
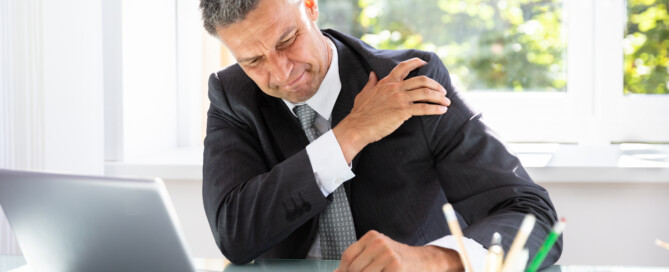
There are people who’ve experienced recurring shoulder pain thinking it was only a rotator cuff problem or arthritis.
But some of these cases are not caused by a problem in the shoulder joint; they are caused by a problem with the heart: a warning that a heart attack is right around the corner.
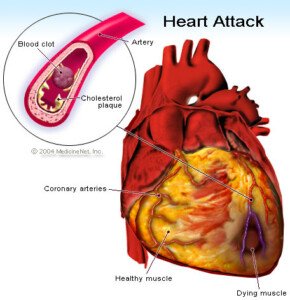
“Most commonly, pain of a heart attack occurs in the center of the chest, but may radiate down the left arm into the shoulders, into the throat or jaw, and at times only occur across the shoulders or the upper back,” explains Dr. Ronald Scheib, MD, past Medical Director at Pritikin Longevity Center & Spa in Miami.
“Referred pain is the description of pains caused by internal organs, which are felt at some area distal on the surface.
“That area can be, in the case of heart attacks, jaw, shoulders, chest, upper abdomen, and occasionally in very unusual places, possibly related to an individual’s prior illnesses.”
Does this mean that if you suddenly start developing shoulder pain, that you should rush to the ER to get your heart evaluated?
Pain in this joint is extremely common. As a certified personal trainer, I know this for a fact.
A person must review the entire picture, however, when it comes to shoulder pain.
Do you recall straining the joint recently? Is the pain just like the pain you had when you first strained the shoulder lifting something above your head?
What are your risk factors for heart attack?
A lean person who exercises, doesn’t smoke, sleeps well, limits processed food, has low blood pressure and a normal lipid profile, need not fear an impending heart attack as much as, say, a woman over the age of 50 with excess abdominal fat, who never exercises and has very high triglycerides. This described my mother.
I was alarmed at her triglyceride levels and actually said to her, “You could be dead from a heart attack in six months!”
She went to bed that night worried sick over my comment, but made no changes in her diet after that point, and still refused to exercise.
Recurring episodes of shoulder pain were a common complaint from her, and I never made the connection between these “pain attacks” in her shoulder and the condition of her heart, especially since she had had a total of three surgeries on her rotator cuff.
As a fitness expert, it’s never surprising to me that a senior-aged person, who has never exercised her shoulders, eventually develops problems in this versatile but vulnerable joint.
About four months after I made my comment, I took my mother to the ER for chest pains. The day after that she underwent quintuple bypass surgery.
The surgeon had told me that a “massive” heart attack was imminent, possibly within a week, without the surgery.
Once my mother was recovered from the surgery, she reported that the bouts of shoulder pain had disappeared.
This sounds like more than a coincidence. It has always been the same kind of pain, same general location of the joint.
Dr. Scheib explains, “On occasion, the location may vary based on the specific coronary artery, but in general it tends to be repetitive in the same location.”
 Dr. Scheib passed away in 2018. To Pritikin he brought a career in cardiology spanning four decades, including Miami Heart Institute Chief of the Section of Cardiovascular Medicine, and President of the Medical Staff.
Dr. Scheib passed away in 2018. To Pritikin he brought a career in cardiology spanning four decades, including Miami Heart Institute Chief of the Section of Cardiovascular Medicine, and President of the Medical Staff.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Andrey_Popov

Why a Looming Heart Attack Can Cause Nausea, Vomiting

©Lorra Garrick
Vomiting and nausea can be a sign that a heart attack is imminent.
This is not about an actual heart attack in progress, but vomiting and nausea as a warning sign that a heart attack is in the very near future.
“Nausea and vomiting are very complex interactions between the brain and the stomach,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“The scientific thinking behind myocardial ischemia or infarction associated with nausea relates to the vagus nerve,” continues Dr. Fiocco.
Myocardial ischemia simply means depletion of oxygen to heart muscle. Infarction means tissue death.
The vagus nerve “arises from the brain and travels through the neck, along the esophagus, and gives off nerve fibers to the heart before continuing into the abdomen where it supplies nerves to the stomach,” explains Dr. Fiocco.
“So there is the stomach-heart-brain connection. Why people get nausea prior to a heart attack may be similar to why people get arm, neck or jaw pain rather than chest pain.
“A lot of overlapping circuits may cause the brain to misread the signals, leading to nausea or left arm pain rather than chest pain.”
Of course, being overcome with nausea, as a result of conditions ripe for a heart attack, can then lead to vomiting.
Vomiting was a tip-off to me that my mother might be having a heart attack, or that a heart attack was looming around the corner for her.
She awakened one morning reporting difficulty breathing.
I brushed it off as a panic attack, since trouble breathing is one of a panic attack’s classic symptoms.
She had a history of panic attacks, along with “labored breathing.”
That particular morning seemed like just another panic episode, especially since I knew that about five or six weeks prior, she had quit taking Effexor altogether. Effexor helps suppress panic and anxiety attacks.
I was staying with my parents because my father, just days prior, had back surgery.
About a half hour later I heard my mother call out to my father, “Quick, bring it over here!”
Intuition told me she was referring to a waste can and that she was about to vomit.
I raced upstairs to their bedroom and saw my mother upchucking into a small waste can.
Much of it was dry-heaving, actually, but yellow gunk definitely was coming out.
The bells went off because my mother had never vomited during a panic attack or after one subsided.
Since when did she vomit? I knew that an imminent heart attack can cause vomiting.
She just had a bout of breathing difficulty bad enough to make her weep.
Something told me to get her to the emergency room for a cardiac evaluation.
Two evenings later she was undergoing quintuple bypass surgery – just in time, said the cardiothoracic surgeon; though my mother had not suffered a heart attack, he said that a massive heart attack could have occurred any moment due to severe coronary artery blockage.
In my mother’s case, the vomiting was a sign that something was wrong with her heart, I believe.
Nothing she ate the day prior could explain the upchucking.
She had not been in any pain, either (pain can cause nausea). So in hindsight, it’s logical to conclude that my mother’s pending heart attack caused the vomiting (and difficulty breathing).
Does this mean that next time you feel nauseous or vomit, you should fear imminent heart attack?
Of course not. But take notice of any other symptoms like shortness of breath, trouble breathing, chest pain or tightness, sweating, and pain in the jaw, arm, neck or back that can’t be explained by other benign factors …
… and take into consideration if you have risk factors for a heart attack like smoking, excess weight, lack of exercise, diabetes and a junk food diet. Puking is no laughing matter.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: ©Lorra Garrick

How Dangerous Is Low Blood Pressure? How to Raise It

Chronic low blood pressure may be harmless or extremely dangerous; low blood pressure can cause damage to your organs, not to mention cause you to take a serious fall from fainting.
Low blood pressure is called hypotension, and as mentioned, it can be a harmless condition as well, or cause only mild problems.
Low blood pressure has many causes including heart conditions, nutritional deficiencies and medications. The cut-off for normal BP readings and high readings is 140 over 90.
So when does blood pressure get too low?
“The first question to address is if the blood pressure is really too low,” says Teresa Caulin-Glaser, MD, a cardiologist and senior vice president with Service Lines, OhioHealth.
“In general, if patients are asymptomatic and the systolic (“top number”) blood pressure is approximately 90mmHg or better, you do not need to treat.
“However, if the person is developing symptoms such as dizziness, fatigue, and/or passing out, there needs to be a full history and medical evaluation.”
If you believe your blood pressure is too low, review any medications you’ve been taking.
Explains Dr. Caulin-Glaser: “If the evaluation determines there are no medical problems and/or medications such as diuretics, ace-inhibitors, beta blockers, calcium channel blockers causing low blood pressure and symptoms, then there are non-pharmacologic treatments that can be implemented.”
Other symptoms of low blood pressure: lack of concentration, blurred vision, fatigue, nausea, thirst, cold and clammy skin, and rapid shallow breathing.
A big danger of low blood pressure is organ damage due to insufficient blood supply to them.
As you can see, low blood pressure can present with an assortment of symptoms, while high BP (also known as hypertension), which is a major risk factor for stroke, offers up no symptoms, which is why hypertension is nicknamed “the silent killer.”
So how do you raise low blood pressure that’s creating symptoms?
Dr. Caulin-Glaser says, “Some simple options for treatment are drinking fluids to decrease the risk of dehydration, increasing the amount of sodium in the diet, and decreasing alcohol intake.
“There are medications such as fludrocortisone that can be considered in the treatment of symptomatic low blood pressure, but this would be under the direction of a physician after a full medical evaluation.”
Other causes of low blood pressure: vitamin B12 deficiency causing anemia (result of a vegan diet, since this vitamin is found in animal-derived foods); pregnancy; low blood sugar; severe infection.
The low blood pressure that’s caused by infections of the urinary tract, lungs or abdomen, can be fatal.
(High BP can be life-threatening, but there are natural ways to bring high BP down to normal levels.)
Typically whenever one sees a doctor for any reason, a BP reading is taken. It’s perfectly okay to request that your BP be taken at the conclusion of the doctor visit, because by then, much of your anxiety will be diminished.
Otherwise, your readings may be uncharacteristically high if taken at the beginning of the visit, due to anxiety; this is known as white-coat syndrome.
Low blood pressure has many causes, but if there are no accompanying symptoms, then you need not worry about having BP that is below normal.

Dr. Caulin-Glaser is an experienced physician, teacher and researcher in the specialty of cardiovascular disease, and formerly the system vice president for Heart & Vascular Services at OhioHealth.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/kurhan

Life Expectancy in Elderly After Coronary Bypass Surgery

The life expectancy (long-term survival) of elderly people after coronary bypass surgery is receiving increasing attention, since the population of advanced age people is ever-growing.
This means more and more elderly people, including octogenarians, are having coronary bypass surgery (a.k.a. CABG).
“Life expectancy after CABG is difficult to determine because so many factors are involved,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital, one of the nation’s top 50 heart hospitals.
And this applies to the elderly population.
“Mortality within 30 days of CABG is less than 2 percent, and that is including some very sick patients undergoing CABG,” says Dr. Fiocco.
When an elderly person has coronary bypass surgery, other factors still remain an important part of the life-expectancy equation:
In other words, the CABG and post-op may have gone without a hitch, but an elderly individual inherently is at risk for other serious conditions such as cancer, Alzheimer’s disease and dying in a car accident that otherwise would result in only moderate injuries for someone much younger.
Thus, the question of “What is the life expectancy for the very old patient after coronary bypass surgery” almost doesn’t seem to make a lot of sense.
Again, this is about life expectancy, rather than a more immediate survival rate.
Once the elderly patient is out of the woods in terms of possible post-op complications (e.g., internal bleeding, pneumonia, infection, stroke), the life expectancy is extremely variable.
But of course, it’s within the confines of how much longer any 80-year-old (CABG or not) is expected to live.

For elective coronary bypass surgery (meaning, it’s not performed on an emergency basis), the mortality rate falls below 1 percent 30 days post-op.
Dr. Fiocco explains, “Life expectancy beyond that is determined by so many factors it is hard to quantify.
“Was the patient 50 years old when the surgery was performed or 80?
“Did the patient stop smoking?
“Change their diet?
}Exercise regularly?
Control blood sugar levels after CABG or did they continue in the ways that led them to surgery in the first place?”
Though the patient’s new “plumbing” consists of cleaner veins harvested from either the leg or arm, to replace the clogged, plaque-caked coronary arteries, don’t assume that the elderly patient can get away with bad health habits — with the idea that it will take another 20 years for the grafted blood vessels to develop severe blockage —
— so why bother being health-conscious if the patient would have to live to 100 or older by the time another bypass surgery is needed?
Well, here’s the deal:
The grafted vessels are veins from the legs and arms; they were not designed by nature to endure the blood pressure forces that coronary arteries are!
They aren’t as durable, and if the patient takes excellent care of his body, the replacement vessels should last 10-15 years.
So imagine the potential disaster if the elderly CABG patient fails to quit smoking or lose weight, and/or won’t stick to an exercise program and eat healthfully!
The plaque-buildup rate in the grafted veins that came from the leg or arm is much faster than the plaque-buildup rate in coronary arteries.
Dr. Fiocco adds, “A large study did show average life expectancy after CABG was approximately 17 years, but this was from the 1980s and it is likely even higher now.
“Again, what determines anyone’s life expectancy after CABG is what got you there and what you change going forward.”

Shutterstock/Interpass
Some elderly coronary artery bypass patients will continue living on a food pyramid whose bottom tier is comprised of foods that damage the heart.
They will also continue to avoid exercise and maintain other habits hazardous to the heart.
And likewise, other elderly coronary bypass patients will completely overhaul their lifestyle habits:
Quit smoking, lose weight, avoid trans fats and limit saturated fats, take up aerobic and strength exercise, practice better stress management and be compliant with appropriate medications.
It’s intuitive who will have the much longer life expectancy.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Does Normal Blood Pressure Mean You Don’t Have Heart Disease?
The answer is NO!
In fact, you can have life-threatening heart disease — extensive coronary artery blockage — and still have consistently normal blood pressure readings.
“High blood pressure (Htn) causes the occlusions (blockages), but occluded arteries do not cause Htn,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Blood pressure can be normal even in patients with severe coronary artery disease because they still may have diabetes, elevated cholesterol, genetic abnormalities, and/or a smoking history, all of which can cause coronary artery disease.
“But sometimes the blood pressure is normal.”
In fact, you can have 97 percent blockage in your coronary arteries – an emergency situation – yet have perfectly normal blood pressure.
This was the case with my mother. She faithfully took her blood pressure almost daily with a home device, and the always-normal blood pressure readings gave her peace of mind when it came to her heart health.
However, little did she know that her coronary arteries were becoming dangerously blocked. In fact, the catheter angiogram report said “sub-optimal occlusion.”
The heart surgeon told me this meant about 97 percent blockage. He took one look at the angiogram and decided that my mother needed quintuple bypass surgery ASAP; about two hours later she was wheeled into the operating room.
Yet right up to that point, her blood pressure was in the normal range. So if you have good blood pressure readings, don’t be fooled and think you can’t possibly have heart disease.
Though high blood pressure (hypertension) is one of many risk factors for heart disease, the absence of hypertension does not in any way get you off the hook from America’s #1 killer of both men and women.
Other factors can cause heart disease even if you have normal blood pressure:
1) Lack of structured exercise
2) Poor diet such as high sodium
3) Smoking
4) Overweight/BMI greater than 25
5) Chronic emotional stress
6) Insomnia/sleep deprivation/sleep apnea
7) Sleep exceeding 9 hours/day including naps
8) Family histor
9) Diabetes/prediabetes
10) Poor cholesterol profile. Do you have any of these risk factors for heart disease?
So don’t be deceived by normal or low blood pressure readings.
The risks of heart disease are numerous, and the absence of one of these risk factors in no way means you can’t possibly have dangerous blockage in your coronary arteries.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}