

Causes of the Butt Wink in Back Squatting
It’s a myth that the squat butt wink is caused ONLY by tight hamstrings or tight hips!
Want to know what really is behind the cause of the butt wink motion that so many people do when performing the back squat?
The answer is really quite simple: The trainee fails to maintain a straight back.
But then, that begs the next question: Why do people fail to keep a straight back when performing this version of the squat?
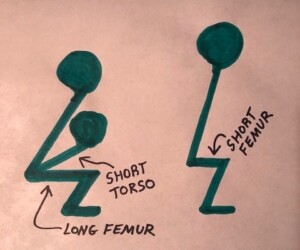
I have a second explanation for the butt wink, though this second explanation may, at least in part, explain why a person fails to keep their back straight as they begin closing in on depth. And that’s “bad levers.”
Though not all people who commit the butt wink have relatively long femurs (or femur bones longer than their torso), it’s a fact that long femurs (relative to torso length, regardless of one’s total body height) predispose a person to the butt wink problem.
But as just mentioned, this may all point back to why a person fails to keep their back straight.
When I say straight, I don’t mean vertical, but rather, not rounded or hunched — but having an arch in the lower back, as shown below.

Freepik
The butt wink is the opposite of the arch; the lower back rounds out or loses its extension; it becomes flexed.
Tight hamstrings are often blamed as the cause of the butt wink.
I do not have tight hamstrings, yet if I get low enough with the back squat, I’ll butt wink.
I can’t say with 100 percent certainty that this is caused by the fact that my femurs are relatively long compared to my torso, but I can definitely rule out BOTH tight hamstrings and tight hips. I have good hip flexibility!
However, I can hit just below parallel before the butt wink starts in.
But still, if I’m nearly ATG, a slight butt wink is present, and has absolutely nothing to do with my hamstrings, hips or ankle mobility.
A butt wink will occur in anyone if they go low enough in a wall squat, in combination with their feet being close enough together, toes pointed straight ahead.
In other words, a person with short femurs, long torso, rubber-band-like hamstrings and hips, will produce a butt wink if they’re right up against the wall, feet less than shoulder width apart (or even at shoulder width), and sink ATG.
Often, the butt wink is caused simply by lack of concentration. Once a person is aware of it, it can sometimes be instantly or near-instantly corrected.
Other individuals will need to practice, and sufficient practice may eliminate the problem.
Poor squat form with the legs can also cause it. Have a qualified partner or personal trainer watch you; trying to watch yourself as you squat is not a practical way to practice this exercise.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/HD92

Can Short People Have Relatively Long Femurs ?

Short people CAN have a relatively long femur, meaning, their thigh bone is longer than their torso — even if their overall height is way shorter than average.
As a former personal trainer, I am fascinated by the anthropometrics of long femurs as this relates to the squat and deadlift exercises, but am puzzled that so many people believe that only tall people can have long femurs that sabotage squatting.

John Kagwe, long-distance runner, 5’6″
Of course, a 6-4 person has a long thigh bone in the absolute sense, but not necessarily in the relative sense.
When it comes to the squat (or deadlift), relative length is the factor, as in length of femur relative to shin bone.
What about short people?
A short person can have a noticeably long femur relative to his or her shin bone length.
If you take notice of enough people in shorts or leggings, you’ll sooner or later come upon a short person whose femurs are disproportionately long for either their torso or their shins.
Now check out the thigh bones of very tall people, RELATIVE to their shins!
Some of them have noticeably short femurs (and thus, lengthy shins).
Being tall does not necessarily screw up your ability to squat or deadlift.
This is clearly evident in strongman competitions, in which athletes of towering height deadlift enormous amounts of weight.
You’ll also see tall people at powerlifting events as well, performing amazing deadlifts and squats.
- With the tall person’s longer thigh bone (in the absolute sense!), also comes a longer shin and longer torso to go with it.
- And the longer shin and longer torso balance things out.
A short athlete can have a femur that’s longer than his or her torso, making the parallel squat more challenging.
If you still believe that short men or women can’t have relatively long femurs, then take some notice of thigh length — relative to overall height — of short adults whenever you’re out and about, especially at crowded venues (amusement parks, shopping centers, festivals, etc.).
You may even spot a “long-femured short person” at your own gym, while also catching sight of men well over six feet who clearly have thighs that are much shorter than their torsos.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com
Sources:
hbing.com/images/search?q=john+kagwe&view=detail&id=CF6FCC3F646FF5DD15FD95A46BB17B0949615210 ninamatsumoto.files.wordpress.com/2010/12/athletes05.jpg
forum.bodybuilding.com/showthread.php?t=138030823&page=1

Can Long Femurs Be a Disadvantage in Daily Life?

You know that long femurs are a curse for squatting exercises, but does this problem carry over to day-to-day activities?
As a former personal trainer and always-fitness enthusiast, this topic intrigues me.
If you clicked on this article you probably have long femurs (and a short torso) and struggle with the squat exercise.
But have you wondered just how much this anthropometry affects daily activities?
The long femurs and short torso body type, indeed, moves differently in real life.
But because real life movements aren’t the same as the back squat, people whose femurs are longer than their torso will not necessarily make a connection between why they must move a certain way, and their body proportions.
When trying to barbell squat, the person whose femurs are longer than their torso will know there’s a big problem.
That’s because it’s impossible not to notice that if you don’t lean your torso far forward in a barbell back squat, you’ll fall backwards.
In real life, the issue of falling backwards gets unnoticed because when a person with long femurs and short torso bends their legs to pick a heavy item off the floor — their hands on the object, or arms wrapped around it — prevents them from feeling the sensation that they’ll fall backwards.

Shutterstock/studioloco
They simply bend over, grab the item and lift it. In a barbell squat, you are not grabbing onto anything for support, so the tendency to fall backwards is glaringly obvious.
The exerciser is thus forced to think about limb proportions and biomechanics.
So if a person with long femurs and a short torso can, indeed, pick a heavy object off the ground, how is he or she affected by their anti-gym squat anthropometry?
It’s a matter of degree of range of motion.
Let’s take two people of equal height and weight, Mark and Rip.
Mark’s femurs are a lot shorter than his long torso. Rip’s femurs are a lot longer than his short torso.
However, both guys train hard and are strong. There are 10 heavy crates on the ground. About midway down on either side of each crate is a handle.
The proper way to pick them up is to squat (feet FLAT on ground), keeping the back upright, grab the handles and “lift with the legs.”
To make this easier to understand, imagine that Mark’s femurs are six inches long and his torso is two feet long.
He only needs to squat half-way (thighs parallel to ground) to reach the crate handles while still in an upright position.
His lift, then, consists of coming out of a HALF squat.
Imagine that Rip’s femurs are two feet long and his torso is one foot long.
Rip will fall backwards long before his squat gets half-way unless he bends his torso to practically parallel with outstretched arms.
He can also grab the top of the crate. However, this puts him in a position that makes it impossible to pick up the crate.
In order to lift it, his groin must be close to the crate. (Did you not picture this with Mark?)
If Rip simply leans over and grabs the handles, what happens to his body? He’s nowhere near a half-squat.
His torso is bent so far over that it’s well-below parallel and his back is totally rounded, butt poking high into the air.
He can pick the crate up this way, but it puts tremendous stress on his lower back!
If he tries to squat parallel while holding the handles, his long femurs get in the way; he can’t do it.
In order to keep his hands on the crate WHILE being in a parallel squat, he must distance his body from the crate, making it impossible to lift it.
The person with long femurs and a short torso has two choices.
He can either lift the crate from the position of being stooped way over (torso well-below parallel, back rounded, legs nowhere near a half-squat, butt sticking up into the air), OR —
He can get into a full “ATG” squat. This will enable him to be close enough to the box to get his hands on the handles, while keeping his back much more upright.
The illustration below will help you understand the general concept.
Who’s in a better position to lift that crate with their hands (assuming both have equal length arms)? The body on the left or right?
Close your eyes and visualize a man with super long femurs in a full squat, back upright, arms out in front holding onto the crate handles for balance.
Unless Rip has arthritic knees, this position is easily doable. Of course, the second he lets go of the handles, he’ll fall flat on his back.
To lift the crate, Rip rises from a full squat, straight up, back upright. The lift consists of a FULL squat.
- Mark picks up 10 crates; that’s 10 half-squats.
- Rip picks up 10 crates; that’s 10 FULL squats.
Rip must do more work! The same scenario occurs when they must set the crates down; Mark gets to do 10 half-squats, but Rip must do 10 FULL squats!
Though Rip may have stronger muscles than Mark, his inability to get into an efficient body position causes him to fatigue faster than Mark; the job is harder.
In summary, those with femurs longer than their torsos must perform full or three-quarter squats (depending on height of object to be picked up), to lift something off the ground with an upright back.
However, those with the opposite proportions get to do only half-squats.
And if the long femur person wants to do a half-squat, he has to forfeit the upright back!
There’s a third option for those with long femurs and a short torso: a wide stance with feet pointed out; this will enable a more upright back.
There’s a caveat: This shifts some work to the weaker adductor muscles (inner thigh).
Nevertheless, those with long femurs and a short torso can train hard and develop a very strong wide or “sumo” stance.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com

Best Way to Tell if Femurs Are Too Long for Back Squat

There’s a fool proof way to tell if your femurs are too long for decent parallel back squats.
If you can’t parallel squat, does this automatically mean your femurs are too long relative to the rest of your body, or is there a way to accurately determine this since other variables can prevent a parallel squat?
I’m a former certified personal trainer and have plenty of experience with relatively long femurs.
Some frustrated clients have asked, “How can I tell if my femurs are too long?” It’s easy to tell these trainees to just look at their legs.
If the thighs look out of proportion in terms of being too long, then you probably have long femurs.
However, what one person might think is too long, another person (who has long femurs) might think is normal.

Almost every anatomical illustration I’ve ever seen depicts the femurs as too long for the rest of the legs (in my opinion, anyways). The shins in anatomical illustrations are usually puny.
Another way people try to evaluate femur length is with a tape measure. The problem here is two-pronged:
1) Exactly where are the measuring points? And
2) For people of generous girth, it will be difficult to locate the hip bone.
Fool proof way to determine if long femurs are hampering your back squat.
And as you may already know, if a person’s torso is longer than their femurs, this can help offset problems with the back squat, even if their femurs are disproportionately long for their legs.
The best way to tell if long femurs are your problem (as well as a short torso) is to find a chair, bench or stool that — when you sit on it, your thighs are perfectly parallel to the floor.
If they are not parallel (meaning, the hips are higher OR lower than the knees), this test won’t be fool proof.
Next, make sure you’re sitting before a mirror, profile facing it. It’s mandatory that you be able to readily view your profile.
If you’re on a chair, sit off of it somewhat to give your calves room to move.
If you’re wearing the shoes that you normally squat in, that’s fine, but for optimal accuracy, do this test barefoot.
At all times during this test, keep feet flat on floor.
Place feet about shoulder width apart, toes pointed ahead.
Place feet so that knees are ahead of them as in a back squat, but keep heels on floor.
Viewing your profile, start leaning forward and maintain an arch in your lower back, as you would during a squat. Do not round your back.
The objective is to form a vertical line between your ankle and the back of your shoulder.
The back of your shoulder is where a barbell would be for the squat.
How far must you lean forward to create a vertical line between your ankle and the back of your shoulder?
In other words, the back of your shoulder (picture a barbell there) perfectly aligns, or is directly overhead, your ankle.
Are you REALLY far over, to the point where you’ve lost that lower back arch?
Is your torso virtually parallel to the floor?
Do you feel your back rounding?
If these points describe you, you have “long femurs.”
But don’t give up yet; see if you can move your knees further ahead of your feet: Shift forward on the seat WITHOUT your feet moving a millimeter.
Is there room to get those knees out a little bit more?
If so, this will allow you to retract a little bit on the forward torso lean.
Below is a wide stance squat. Note how it allows the athlete’s back to be remarkably upright.

Shutterstock/Veles Studio
Nevertheless, these aforementioned issues spell long femurs.
Again, widening the stance will allow you to retract on the forward torso lean.
Two Points to Consider
1) Being very leaned forward puts strain on the lower back and forces the lower back to absorb some of the forces from the squatting movement, and
2) A pronounced dorsiflexion of the feet (caused by moving the knees forward as much as possible) diverts some work away from the hamstrings and glutes, and concentrates more of it on the middle quad muscle as well as the knee joint.
Anyone who knows the basics about the back squat knows that these biomechanics stink.
Yet there are those who insist that the long femur is a lame excuse for lazy people.
The ideal back squat biomechanics have the spinal column in an almost upright position, eliminating low spinal strain, and dorsiflexion is minimal, allowing maximal workload to be absorbed by the body’s three most powerful muscle groups:
GLUTES, HAMSTRINGS, QUADS
This is the recipe for maximal lifts in the back squat with minimal risk of knee joint and low spinal strain.
This test also clearly demonstrates why a short torso is a potential curse in the back squat.
I say potential because if you have really short femurs, they can somewhat offset the short torso.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Vladimir Sukhachev

Best Leg Muscle Building Exercises for Long Femurs

If you’ve given up on the squat due to long femurs, here are the best exercises to build muscle in your legs.
Time and time again, the muscle building literature says that people with long femurs “make poor squatters.”
This is no myth in that trainees with long femurs must have a pronounced forward lean to keep their balance as they approach parallel in the squat, let alone deeper. I’m a certified personal trainer.
“Long femurs” refers to a relative measurement, not an absolute length, in particular, femur to torso ratio.
Thus, if a short person’s femurs are longer than their torso, they will have more difficulty squatting than will a very tall person whose femurs are a lot shorter than their torso.
Best exercises for those with long femurs (no particular order):
Split Squat with Elevated Foot with dumbbells.

Shutterstock/Artsplav
Try to keep torso erect. The drawback is there’s a limit with how much weight you can hold in each hand. (A free barbell can also be used.)
Split Squat with Back Foot on Floor with dumbbells (a.k.a. stationary weighted lunge). Same as above.
Split Squat with Smith Machine. If you’ve reached a point where you need heavier dumbbells with split squats than your gym provides, try the Smith machine.

Freepik.com/pressfoto
Weighted Walking Lunge. Keep torso erect. Whenever I see men doing this with huge dumbbells, they always have well-developed quads.

Shutterstock/VGstockstudio
Though I also gather that some of that development is from other leg exercises, very possibly the back squat, but I’m sure they wouldn’t be doing weighted walking lunges with heavy dumbbells if it didn’t help build leg muscle.
Weighted Single-Leg Step Up.

Shutterstock/WoodysPhotos
Do not confuse this with the aerobic version where the trainee is going up and down for many reps while holding dumbbells.
The dumbbells should be heavy enough to prevent more than 8-12 reps with good form. Keep torso erect and don’t rush.
The higher the step, the more hamstring and glute activation, so use a higher step to really build leg muscle.
Dumbbell Squat. Hold dumbbells on either side and see if you can go parallel. Widen stance until you can and do this before a mirror. The caveat is the limitation on dumbbell weight.
Women with long femurs won’t be presented as much with this limitation, as it’s far less likely that a woman will get too strong to be challenged by holding a 100 pound dumbbell in each hand.
Thus, dumbbell exercises are even better for women with long femurs wanting to build muscle. This isn’t to say that a woman can never “outgrow” 100 pound dumbbells.
Sumo or Wide Squat. This is great at building leg muscle. A person’s femurs would have to be outrageously long for this exercise to be difficult to do.
However, the wider the stance, the more hip and hamstring flexibility required.
A great sumo stance is possible only with adequate hip/hamstring flexibility.
Want to build leg muscle and have long femurs? Then get going on achieving flexibility. (One way to do that is to just keep doing the sumo squat.)
Front Squat. Many with long femurs swear by this for building leg muscle.

Shutterstock/Syda Productions
Sumo Deadlift. This, too, will build leg muscle and has similar dynamics to and requirements of the sumo squat.

Shutterstock/Nomad_Soul
Machine Hack Squat. Give this a try. Many trainees find it uncomfortable and hard on the knees, however. A variation is to face the machine.

Credit: GeorgeStepanek
Leg Press. Get at least a 90 degree knee bend; preferably go deep.

Shutterstock/Free around
Box Squat. Make sure the height of the box allows your femurs to be at least parallel or a little deeper.
Don’t abuse the presence of the box by resting too long on it at the bottom of the movement or losing the lower back arch.
Don’t let feet leave the floor when you make contact with the box. Pretend the box isn’t there, even.
Many fitness professionals swear that this exercise really builds leg muscle, and even those who don’t have long femurs will do these to help build leg muscle.
If you have long femurs and want to build leg muscle, there’s no reason why you can’t achieve this. It’s a myth that the back squat is for every body.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Dean Drobot

Can Low Back Flexibility Offset Long Femurs in the Squat?

Learn about what increasing low back flexibility can do for your squat if you’re stiffed with the curse of long femurs and a short torso!
If you’ve been working hard on getting your squat to parallel without an excessive forward lean, thanks to “bad levers” (femurs longer than torso), you may have read somewhere that the problem is primarily lack of flexibility in your low back.
I have investigated the issue of bad levers or poor anthropometrics as they apply to the back squat, a favorite exercise among those wanting to build up their legs and glutes.
The more flexible your low back is, the less difficult the squat will be if your femurs are longer than your torso. Your overall body height is not relevant.
However, a super flexible lumbar region doesn’t mean that your entire back will be as upright as someone’s whose femurs are shorter than their torso.
Instead, super flexibility will enable the upper portion of your back to be strikingly upright, even if you have a short torso and long femurs.
How do I know? I recently witnessed this. A man was doing back squats. His movements were very deliberate and careful, and it was obvious he’d been working very hard on perfecting his form.
He had a visibly shorter torso than femurs, one of those “high waisted” men. (The better term is “high waist,” not “short waist”).
His low back was so super flexible that the upper portion of his spinal column was fairly upright as he sunk to a tad past parallel.
It looked really odd. This was his way of overcoming the short torso long femur issue.
But it’s too simplistic, and not fair at all, to state: “Well gee, if your femurs are longer than your torso, just improve your low back flexibility and you’ll be able to do the squat.”
The degree of flexibility in this man’s lower spine was significant, something that most men will never be able to attain.
It’s possible this man used to train in a sport that’s conducive to substantial lumbar “bendability,” such as diving.
He was tall, so I’m doubting he was ever much into gymnastics.
His low back was so ultra-flexible that when he walked around the gym, it was molded in hyperextension: His chest puffed out and his butt stuck out.
To the untrained eye, he walked around with arrogance, but what this really was, was a locked-in position of his vertebral column.
To expect to develop this kind of flexibility, to overcome the difficulties that a short torso and long femurs cause in the back squat, is just unrealistic.
However, if you’re one of the few who can develop this kind of rare bendability in the vertebral column, it will definitely assist you with getting parallel and beyond in your back squat.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Can Construction Work Substitute for Gym Weight Workouts?

Are you in construction and wondering if this will build muscle the way that training at a gym with weights will?
The big question for men in construction work who believe that this occupation can replace weight lifting for building muscle, is this: When is the last time you saw a construction worker who was “jacked”?
have physiques that look like the ones you see in magazines like Men’s Fitness, and certainly not the bodies you see in more hardcore bodybuilding magazines.
From time to time I’ll spot a construction worker whom you can tell works out with weights — weights at a gym, not equipment on the job.
Yes, some of the workers routinely hit the gym, and this is what gives them their symmetrical muscular bodies, not anything they’ve been doing at the work site.
This is why you’ll see plenty of skinny, and overweight, potbellied construction workers.
When they are portrayed in movies and TV, often the actors look fresh out of a gym.
This creates the stereotype of construction workers having these wonderfully sculpted, muscled, ripped bodies.
In real life, it’s rare to see such a physique among that row of construction workers sitting on a ledge eating their lunches while they watch the women walk by.
In short, this type of work does not substitute for gym workouts.
Take a look at the vast majority of construction workers for your proof.
Not only that, but more and more women are entering this field, and you certainly don’t see these women resembling Mr. World competitors, or even a fraction of that. They look like typical, 5’4, 144 pound ladies.
Men who wish to build muscle mass will typically work a specified group of muscles in a given training session – to failure. This is not what happens in construction.
On the job, the worker tends to use his entire body, many muscles, and certainly not to muscle failure.
It may also be the same muscle movements nearly every day on the job, and the result is quick adaptation by the muscles — and this will not promote muscle growth nearly as much as a focused, highly structured gym workout.
- Your gym workout is designed to build muscle mass.
- This is not the goal of the work being performed by a man building a house.
- The goal there is to build the house or complete the task at hand.
Look at it this way. If you want big mean biceps, what do you have to do? Curls, of course (along with compound exercises that involve biceps activation).
What task on a construction site mimics targeted biceps — and especially triceps — work?
Though construction workers use their biceps to carry heavy items, the mechanics behind this are quite far-removed from what occurs in the gym when targeting the biceps muscles.
What task on the construction site simulates the bench press?
Though there can easily be some construction movements that are similar to the deadlift, bent-over dumbbell row, overhead press, dumbbell squat and farmer’s walk — it’s important that you realize that:
• A construction worker’s movements lack the structure, deliberation and consistency of a weightlifting regimen.
• Methodical repetitions are not performed on the job site.
• Proper form is rarely given much attention.
• The worker’s dominant arm will be doing most of the work, creating imbalance in the shoulder and back.
Though this kind of work can be grueling and burn a whopping amount of calories, it is not conducive to building the big, strong and symmetrical muscles that you seek.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

What Makes Legs Shake During Leg Presses?
Does doing leg presses make your legs shake?
So your legs shake while doing leg presses; what is going on here? I’m a former personal trainer and was not uncommon for my clients’ legs to start shaking in the middle of performing pressing routines.
And when this happened for the first time, almost always, if not 100 percent of the time, the client would ask, “Why are my legs shaking?”
If this is happening to you, do not worry. I told my clients that leg shaking is a sign of very hard work, in combination with the lower body performing a routine that it’s not accustomed to.
This is a simplistic explanation, but I obtained a more thorough explanation from Fabio Comana, Senior Fitness Educator for the National Academy of Sports Medicine (NASM) as well as an ACSM-certified personal trainer
He explains that when your legs shake during presses, it’s “nothing really to be concerned about other than the fact you have exerted yourself a little hard and the muscles are not receiving adequate oxygen.
“The shake experienced during the exercise is simply muscle unaccustomed to this intensity of work — during recovery, most commonly attributed to muscle fatigue.
“I would doubt any neural or physiological concern unless damage with injury was inflicted upon the muscle.”
Some people report quivering legs after the exercise, but what about during?

Freepik.comgpointstudio
Well, limbs are under the most exertion during a strenuous routine.
When my clients’ lower limbs shook, this told me they were pushing their absolute hardest and had a high tolerance for lactic acid buildup, or that wicked “burn” that occurs in strenuously-working muscles.
I also told my clients that the quivering or trembling is a temporary reaction in their legs.

Shutterstock/Syda Productions
After several more workouts on the pressing apparatus, or whatever maneuver causes the quivering, their muscles will start adapting and will eventually no longer cause the trembling.
Additionally, I inform clients that once the routine is completed, the quivering should stop.
When muscles are short on oxygen, as a result of a very intense exercise routine, they may spasm, and this is what you perceive as the shaking.
These are benign spasms, which may also be on a much smaller scale in the form of muscle twitching.
The reason that the whole-limb-shaking is more likely to occur in legs, than in the arms, is because the lower body has the largest muscle groups in the entire body, and hence, these large, strong muscles are able to generate more force production than the muscles of the upper body can.
This means greater potential for lots of work to get done in a short amount of time, and as a result, muscles are apt to get depleted of oxygen in very hardworking people.
Due to the mechanics of the leg press machine, a person can exert quite a bit of effort with this equipment, and shaking is more likely to occur due to the person’s body position, versus when he or she is performing barbell squats.
 Fabio Comana is frequently featured on TV, radio, Internet and in print publications, and has authored chapters in various textbooks and publications.
Fabio Comana is frequently featured on TV, radio, Internet and in print publications, and has authored chapters in various textbooks and publications.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Free around

Prevent Finger Pain from Climbing: 6 Ways

Follow these guidelines to help prevent finger pain related to climbing.
Finger pain from climbing can be caused by more than one factor, says Joseph Ciccone, DPT, CSCS, a doctor of physical therapy and certified strength and conditioning coach with ColumbiaDoctors in New York, NY.
“If you are a novice and start climbing, then having light soreness can be expected as your body is performing a new activity and needs a chance to accommodate to the new stresses,” says Ciccone.
“It is especially important to gradually increase amount of time climbing and difficulty levels, as this will allow your body to become conditioned to the new imposed stresses, which will decrease soreness.”
That’s the first step to preventing climbing-related finger pain. I’ve done a lot of climbing myself, and can vouch that sometimes, finger pain or discomfort comes the day after climbing, so it’s easy to get ahead of yourself while you’re participating in this sport without realizing how your fingers will feel the next day or two after.
#2: Ciccone advises all levels of climbing athletes to perform strengthening exercises for the hands, elbows and shoulders, “as the strength will improve control and stability when climbing,” he says.
#3. Ciccone explains that after climbing you can apply a cold compress or ice to your hand and fingers to minimize pain and inflammation. You can dip your hand in a bowl of ice and water and soak for 10-15 minutes.
#4. Climbing is one of those sports where the athlete really pays for it when consistency is lost over even a short time. Ciccone urges consistency.
Two or three times a week is consistent enough to get the fingers used to the stress of climbing.
#5. Some climbers don’t believe cross-training is necessary, and shy away from gym workouts.
At a minimum, these athletes should use hanging boards and devices specifically for strengthening the hand and grip, says Ciccone.
#6. “In addition it should be noted that climbing is a full body activity, and having addressing shoulder, core and lower extremity strength/dexterity and endurance are all factors that can take stress away from fingers and utilize other parts of the body to distribute forces.”
This means that climbers will benefit from strength training. This doesn’t have to be with heavy weights.

Shutterstock/Oleksandr Zamuruiev
Strength training with light to medium resistance will strengthen joints and help the body, as Ciccone says, distribute forces more efficiently.
Implement these guidelines and they’ll go a long way at helping prevent climbing-related finger pain.
 Joseph Ciccone’s practice focuses on numerous musculoskeletal conditions, including management of chronic and acute injuries, and surgical rehabilitation. He has a strong interest in adolescents, weekend warriors and professional athletes.
Joseph Ciccone’s practice focuses on numerous musculoskeletal conditions, including management of chronic and acute injuries, and surgical rehabilitation. He has a strong interest in adolescents, weekend warriors and professional athletes.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Seasontime

Walk Backward on a Treadmill for Low Back Pain Relief

You can relieve your low back pain by walking backwards on a treadmill…
…but if you hold on, you’ll sabotage this benefit!
You need to stand upright and keep your hands off the rails.
Walking backward on a treadmill can relieve low back pain, says a study (Journal of Exercise Physiology online (Vol 14, No. 2, April 2011).
The JEP’s summary includes: “The results support backward walking to reduce pain and increase low back range of motion for athletes with LBP.”
Though the study was conducted on athletes, namely NCAA Division 1, this doesn’t mean that in order to reap the benefits of backward walking for your low back pain, that you must be a collegiate athlete.
“Walking backwards helps to strengthen the quads, calves and glutes,” says Dr. Tom Carpenter, whom I interviewed for this article.
Dr. Carpenter is a corrective exercise specialist, certified personal trainer and chiropractor, inventor of Stand Corrected™, a portable harness-like stretching tool that helps alleviate back, neck and shoulder pain.
“These muscles help to improve balance and posture in general, but specifically, the quads and glutes contribute to stabilizing the pelvis as well,” continues Dr. Carpenter.
“The pelvis is the foundation for the lumbar spine and lower back muscles.
“By improving the proper tone and balance to these muscle groups, the very important pelvic alignment is supported, contributing to a healthier lower back.”

Stand Corrected™
I’ve encouraged my personal training clients to walk backwards on a treadmill for several reasons including alleviation of back pain.
Athletes may have been chosen for the JEP study simply because they can quickly adapt to walking backwards, versus the general non-athletic population.
I’ve had my non-athlete clients walk backwards on a treadmill without any problem, including a middle-age, obese woman with osteoarthritis in her knees.
About 80 percent of people with low back pain do not show, via imaging results or diagnostic tests, any specific pathologies that can explain the low back pain.
Even a very fit athlete can experience low back pain upon bending over to reach into the back of a refrigerator (I actually knew a firefighter-in-training who experienced this).
For the JEP study, subjects were given a pretest which included getting used to walking backwards on a treadmill without holding on.
Not holding on is very important because this forces the body to move in a natural pattern.
On the other hand (no pun intended), placing your hands on the rails cancels out the benefits of a hands-free movement and produces an unnatural, inefficient posture.
The pretest had the subjects walking backwards without knowledge of the speed, which was gradually increased until they said they could no longer comfortably handle whatever speed they were at (without holding onto the rails, of course).
The control group was “healthy active individuals” who did not have low back pain.
After the pretesting period, the subjects then walked backward on a treadmill three times a week, for 15 minute sessions, and controlled the speed.
The report states: “…both groups increased velocity, stride parameters, and low back ROM following 3 weeks of backward walking exercise.
It appears that the presence of LBP did not interfere with the ability of participants to adapt to the actions of backward walking. Both groups achieved greater walking velocity…”
ROM refers to range of motion. The report also says: “…all LBP subjects reduced self-reported P and over half significantly increased low back range of motion.
This finding suggests, as has been previously reported (21), that backward walking improves low back flexibility..” And “P” refers to pain.
How does treadmill backward walking relieve low back pain?
The explanation is technical, but the translation is: The joint action when walking backward differs a bit from the joint action of walking forward.
This altered joint action affects the vertebral disc space…in a positive way.
But you don’t need to know how treadmill backward walking relieves low back pain in order to get on a treadmill and just do it.
I have my clients start out very slowly and I stand before them, my feet straddling the moving tread.
This gives them peace of mind, and it’s also a good practice on my part as a fitness professional.
But if you’re alone, start at a very slow speed, say, 1 mph.
Like the study subjects did initially, place hands on the treadmill rails and get positioned with good walking posture. But at some point you must remove your hands.
Otherwise you’ll cause a disservice to your body. Holding on “would negate the normal healthy bone rhythms and core muscle stability that are engaged by not holding on,” says Joseph Ciotola, MD, orthopedic surgeon at The Orthopedic Specialty Hospital at Mercy Medical Center.
Don’t fear falling off; you’re going only 1 mph. Spend as much time as needed getting used to this. It’s supposed to feel different, even awkward.
But you will get used to it. As you get more comfortable, let go of the rails, and just gradually increase speed.
Mimic the research: Walk backwards on the treadmill without holding the rails, three times a week, for 15 minute sessions.
See if this doesn’t help relieve your low back pain, especially if your doctors have not pinpointed the cause via diagnostics.

Photo credit: Aleesia Forni
Based upon 30+ years of experience, Dr. Carpenter’s practice approach reflects his belief that restoring optimum health and function will enable his patients to enjoy a much greater amount of vitality and wellness. Chiropractic care is true health care, not sick care!
 Dr. Ciotola is dedicated to providing his patients the best orthopedic care possible for their hip, knee or shoulder pain.
Dr. Ciotola is dedicated to providing his patients the best orthopedic care possible for their hip, knee or shoulder pain.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}