
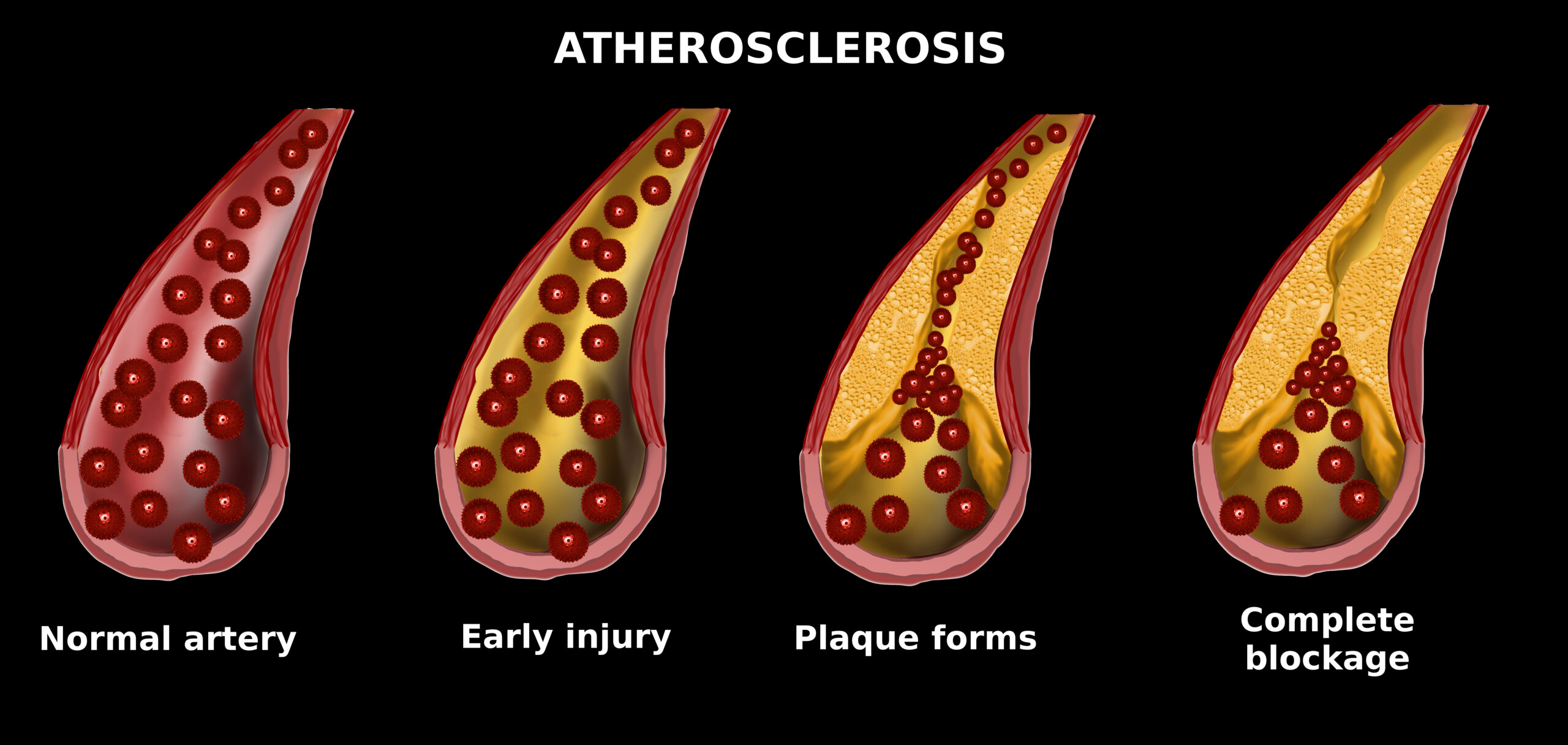
Can You Have a Low Calcium Score with Blocked Arteries?
Is it possible to have blocked arteries but at the same time a low coronary calcium score?
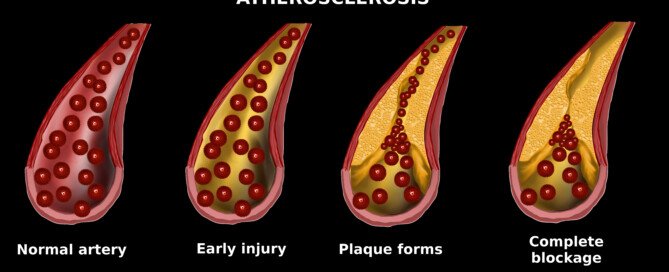
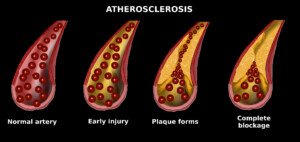
The calcium score is a numerical value that’s associated with the likelihood of having soft plaque heart disease.
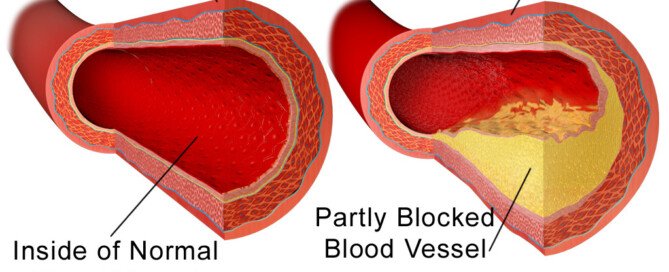
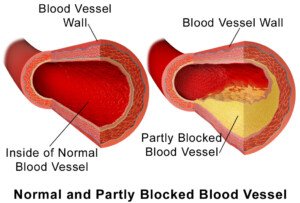
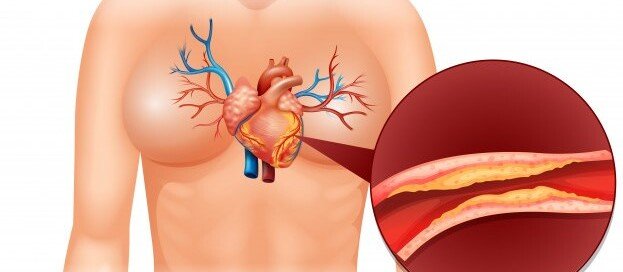
“A blocked artery means the narrowing in the artery is more than 70 percent narrowed, the point where blood flow is restricted,” says Dr. Larry Santora, MD, a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
Dr. Santora explains, “This is called ‘obstructive coronary artery disease.’ There is a direct relationship between total calcium score and ‘obstructive disease,’ so if the calcium score is greater than 100, the chance of an abnormal stress test is greater than 3 percent.
“If the score is greater than 400, the chance of an abnormal stress test is 15 percent, and so it goes”
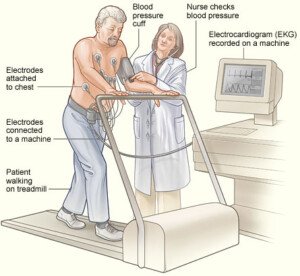
A stress test can be done either with physical exercise or a chemical stress test.
“So you can have obstruction, though it is very unlikely, even with a very low score.
“However, if you are having angina, even with a very low score, then the chance of an abnormal stress test becomes dramatically higher.
“So anyone with symptoms of chest pain should have a stress test first, because you are then trying to determine if the chest pain is due to obstruction of blood flow in the coronary arteries.”
Can a person have a very high coronary calcium score, yet less than a 70 percent blockage in the arteries?
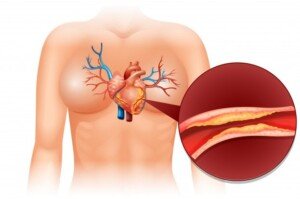
Dr. Santora explains, “The reason the score is high but the artery lumen (channel) is not severely narrowed is because the plaque is forming in the walls of the artery.”
Wouldn’t a CT angiogram (which measures the amount of unstable soft plaque) be preferable over a stress test?
After all, can not a stress exam miss severe coronary blockage? Wouldn’t the CT angiogram, which emits less radiation than a stress test, be more definitive?
“The CTA would be a helpful tool, but not preferable, since the CTA shows the shape of the artery (anatomy), but not the function or ‘flow’ in the artery,” says Dr. Santora.
Flow is also referred to as perfusion, which is why stress exams are usually called perfusion stress tests or myocardial perfusion tests.
Dr. Santora continues, “The stress test is a ‘functional test,’ whereas a CTA is an anatomic test. Sometimes, even with an invasive angiogram (which uses catheters), I find blockages that look borderline in narrowing, like 60 to 70 percent.
“Before putting in a stent, we place a wire through the narrowing and measure flow.
“It is called a functional flow reserve test (FFR). If the flow is not restricted, then I do not put in a stent.”

Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus
Calcium Score Too High for CT Angiogram to Show Arteries?
Suppose you’ve been wanting a CT angiogram, and your cardiologist has informed you that the CT angiogram would be pointless —
— because your very high calcium score indicates that all the calcification in your arteries would obscure the images on the CT angiogram.
What should you do at this point?
“A CT angiogram has limitations if there is severe calcification (a calcium score > 800),” says Dr. Larry Santora, MD, a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
He adds, “There is a good chance the CT scan cannot see through the calcium to see the lumen (channel) of the artery. High scores are a relative contraindication.”
So if your physician says that the CT angiogram is out, due to a very high calcium score, this is the real deal, unfortunately.
It’s likely that one day, technology will advance enough to create a way for a CT angiogram to read through the heavy calcification.
Until then, you are left with the next step, which is a “stress test,” which can be done via exercise to stress the heart, or chemical stress (usually given instead of exercise if the patient cannot carry out sufficient physical exertion, e.g., patient has osteoarthritis).
Dr. Santora says, “If the stress test (nuclear or stress echocardiogram) is normal, you do not need a CT angiogram.”
This will sound surprising to the patient who has a very high calcium score, since the higher the calcium score, the higher the likelihood that he or she will have a heart attack in the next several years. The correlation between the two is well-established.
“The stress test becomes abnormal when there is a narrowing of at least 70% in the coronary artery.
“Such a blockage may benefit from a mechanical fix, like an intracoronary stent or coronary bypass.
“The idea is if the stress test is normal, there is no restriction of blood that requires such a fix.”
But Dr. Santora explains that there are two key indications for the CT angiogram:
No. 1: “A stress test that is equivocal for decreased blood flow — that is, it is a little abnormal, but not enough to make a diagnosis.”
And No. 2: “Unexplained chest pain.”
If the patient with the very high calcium score undergoes a stress test with normal or negative-finding results, and he has not been having unexplained chest pain, then he does not need the CT angiogram. Dr. Santora says that CT angiograms are not screening tests.
So if you’re this type of patient with the exceedingly high calcium score, but a normal stress test result and no chest pain … what is your next step?
Well, it certainly isn’t to go home feeling safe, because there is a reason why your calcium score is so high.
You need to go on an aggressive treatment to prevent further calcification of the arteries, increase stabilization of the plaque, prevent or slow further plaque buildup, and even reverse some of the plaque buildup.
A normal stress test does not rule out the presence of the dangerous kind of plaque – the “soft” and unstable plaque that is prone to rupturing and causing heart attack.
Do not let a normal stress test fool you. A stress test simply detects blood flow through arteries.
It cannot tell how much soft plaque you have! The CT angiogram can do this.
But the CT angiogram, again, is pointless if the images are obscured.
Hence, you absolutely need to commit to aggressive treatment, which comes in the form of a change in diet, addition of supplements, and prescription drugs that are designed to put some brakes on coronary plaque buildup.
Daily, structured exercise is also part of this plan. If you smoke, quit, once and for all.
Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
No Family History of Heart Disease: You Sure About That?
You can be fooled into thinking that you don’t have a family history of heart disease!
Do you really know for sure? Would your relatives tell you they had heart disease?
My mother repeatedly told a steady stream of medical professionals, “I have no family history of heart disease,” and, “There is no heart disease in my family,” after she had a quintuple bypass surgery and mitral valve replacement.
There is no way my mother could know with certainty that she has no family history of heart disease.
She bases this on the fact that her own mother lived to 94 and was never diagnosed with heart disease. Her father died at 73 from an endocrine disorder.
We can’t rule out that her mother had heart disease.
We can only rule out that by the time she was 94, if she had heart disease, it had not yet reached the point of coronary attack.
And had her father lived beyond 73, who’s to say he wouldn’t have eventually developed chest pain, shortness of breath and even a massive coronary? He was not autopsied.
For all we know, at the time of his death, his coronary arteries were 90 percent blocked.
Had he lived another several years, who’s to say he would not have ended up in the ER with chest pain, and then next day, had emergent coronary bypass surgery?
My maternal grandparents were never diagnosed with heart disease, but then again, they also never underwent the following modern-day screening and diagnostic tests:
- echocardiogram
- catheter angiogram
- CT angiogram
- CT calcium score
- treadmill stress test
- adenosine perfusion scan (chemical stress test)
- C reactive protein blood test.
A person, such as my mother, could have very advanced heart disease yet still have a normal-sounding heartbeat under a stethoscope!
A cardiologist gave her a clean bill of health just 10 months prior to the emergent quintuple bypass surgery!
And this clean bill of health was based on a stethoscope exam, pulse-feel, blood pressure reading, an EKG that was impossible to discern due to a “left bundle branch,” height and weight chart, and questions about family history of heart disease!
I’ll assume that my maternal grandparents had routine physical checkups – that were very similar. You can see how heart disease can be missed with such rudimentary testing.
This happens contemporarily as well. People are told they are as fit as a fiddle, after a routine physical, and then shortly after keel over from a cardiac event caused by severe coronary artery blockages.
Both my mother’s parents could have easily had undiagnosed heart disease, even though they didn’t die from it. Many people with undiagnosed heart disease die from unrelated causes.
Pneumonia following hip replacement took my maternal grandmother. There was no autopsy. How do we know she didn’t have 90 percent coronary artery blockage?
I might add that my mother’s sister, about eight months prior to my mother’s coronary bypass surgery, had stents placed in her coronary arteries!
My mother’s sister has heart disease! This is family history! However, my mother didn’t know this (and still doesn’t) because my aunt never told her. I found out through another relative!
If you think you’re safe from coronary heart disease because you believe there’s no family history of it, you may want to revisit your conclusions good and hard.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/brgfx

Why Isn’t All Stable Angina Treated with Stents or Surgery?

Must some people live with angina instead of getting it treated with stents or bypass surgery?
So many people live with stable angina rather than get stents or bypass surgery.
“It is rare that angina can’t be treated with stents or CABG in this day and age, but it does occur.” CABG stands for coronary artery bypass grafting,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Severe diffuse narrowings throughout the entire length of an artery may be untreatable with either method,” continues Dr. Fiocco.
“There are also cases not suitable for stents, but may be anatomically fine for CABG, but other medical conditions make CABG prohibitive (i.e., severe lung disease, terminal illness, etc.).
“There are patients whose angina is well-controlled with medication, and that is an appropriate treatment method as long as the patient is followed closely.”
In 2006, 10.2 million U.S. people were living with angina.
Angina is when there is restricted blood/oxygen flow to the heart due to narrowing and blockage of the coronary arteries.
Every year about 500,000 people in the U.S. are diagnosed with stable angina: Symptoms occur only upon physical exertion and sometimes mental stress.
That’s a lot of people living with a condition that seemingly could be corrected with stenting, angioplasty or bypass surgery, but obviously, that is not the case.
Dr. Fiocco continues, “Many patients control their angina for years with medication. Yes, they may have to curb their lifestyle (no chopping wood, running marathons, etc.), but this is an acceptable treatment regimen.
“If symptoms worsen, become more frequent or difficult to control, then they may need stenting or CABG.
“Some may have no choice but medical treatment due to other health problems or strictly based on coronary anatomy.
“Others prefer to avoid the more invasive procedures, which is acceptable as long as their symptoms remain stable.”
Medications used to treat stable angina are the following: aspirin, nitrates, beta blockers, statins, calcium channel blockers, ACE inhibitors, and ranolazine.
A person with angina should also make lifestyle changes, such as quitting smoking, losing weight, exercising and managing mental stress better.
The reason that coronary bypass surgery is not the treatment of choice for stable angina is because balloon angioplasty with stent placement has been shown to be an effective treatment, and of course, it’s not nearly as invasive as CABG.
Medications will still probably be necessary after the stenting.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
Sources:
americanheart.org/presenter.jhtml?identifier=4591
mayoclinic.com/print/angina-treatment/HB00091/METHOD=print

Are You Scared of a Catheter Coronary Angiogram?

Are you scared to have a catheter angiogram, but need one?
A catheter coronary angiogram is an invasive procedure, and if your doctor recommends you should have one, you may end up too afraid to go through with the procedure — once the risks are outlined to you.
“The definitive test for the diagnosis of coronary artery disease remains cardiac catheterization/angiography,” says Christopher J. Hanifin, PA-C, who was previously a physician assistant in open heart surgery with Cardiothoracic Surgery of South Bend in South Bend, IN.
“In this test a catheter is guided to the heart, and dye is introduced into the coronary arteries.
“Images can then be obtained to determine the extent and location of any blockages. In many cases, the cardiologist can perform angioplasty and relieve the blockage on the spot.”
My mother was told she should have a catheter coronary angiogram. She was verbally told the risks, then given paperwork detailing the risks.
When she was done reading, she put the papers aside and refused the procedure, wanting to go home (she had been admitted to the cardiac unit after visiting the ER with chest pain).
I insisted she have the catheter coronary angiogram, even though I, too, was quite nervous about the risks.
Risks of a Catheter Angiogram
Heart attack, stroke, tear in an artery, blood clots, excessive bleeding, kidney damage and infection. That’s enough to scare away an elephant.
At the same time, I knew that the coronary catheter angiogram would get to the bottom of my mother’s problems.
The procedure would be able to — with 100% accuracy — rule out, or in, blockages in the coronary arteries.
My mother had been experiencing peculiar symptoms for a few months, and especially over the few days preceding the hospital admission.
I was fearful of the coronary catheter angiogram, but more fearful of not finding out what was causing the shortness of breath and chest pain.
How to Put Your Anxiety Over a Catheter Angiogram at Ease
Think about what could happen if you skip this procedure out of fear, and go home … and then a few days later, you feel a large brick pressing down on your chest: a heart attack.
Tell yourself there’s a very good reason your doctor wants you to undergo this procedure.
If you’re having symptoms that fit the bill for coronary artery disease and especially an impending heart attack — and you’ve been repeatedly dismissing these symptoms as yet another panic attack, anxiety attack or acid indigestion — for once and for all, have the coronary catheter angiogram if your cardiologist recommends it.
This procedure is not a standard screening tool and if you don’t present with certain criteria, your doctor will advise against it.
Though the procedure is invasive and carries the frightening risks, the chances of serious complications are actually small.
I’m certainly glad I talked my mother into having the catheter coronary angiogram.
I had told her: “If you go home, you’ll be back to square one and be wondering if something’s wrong with your heart. Just get this procedure done and you will finally have answers, and a treatment plan in place.
“Otherwise, if you skip this and go home, you’ll be empty handed. And what if something really is wrong with your heart? No treatment plan in place, you’re home, heart attack, you’re screwed.”
My Mother’s Cath Angiogram Results
The catheter coronary angiogram revealed extensive blockage in five of my mother’s coronary arteries.
Within two hours of this result, she was in the OR for quintuple bypass surgery. She fully recovered.
 Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University, NJ.
Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University, NJ.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/MAD.vertise
CT Abdomen Scan Can Predict Heart Disease and Mortality
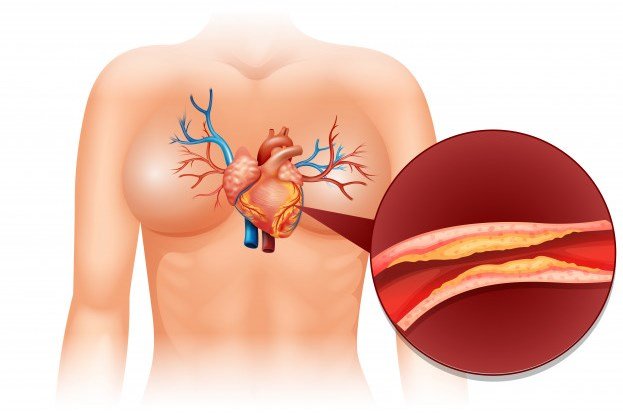
Plaque in your abdomen is a strong clue that there is plaque in your heart: coronary artery disease, or “sludge” in your heart’s arteries.
When a CT abdominal scan shows very high degrees of abdominal aortic calcium, these patients are about 60 percent at risk of having CAD: coronary artery disease.
Plus, the presence of the abdominal aortic calcium (high levels) means a higher risk of death.
Not surprisingly, the absence of abdominal aortic calcium is associated with low risk of the coronary artery disease.
“The typical abdominal CT (whether or not it includes the pelvis) starts above the diaphragm and includes some of the lung base and some of the bottom of the heart,” says Brett Mollard, MD, a board certified diagnostic radiologist who specializes in abdominal imaging and nuclear medicine.
“The coronary arteries are generally at least partially visualized, particularly the right coronary artery, allowing us to see if any atherosclerotic calcifications are present.
“Coronary artery calcifications are used to help risk stratify patients for underlying coronary artery disease.
“While a CT of the abdomen won’t fully assess the coronary arteries, it can tip off an ordering provider to the presence of coronary artery calcifications and lead to further risk stratification and/or a dedicated coronary calcium screening CT.
“Occasionally, incidentally detected coronary calcifications may be the most important finding we make on an abdominal CT.”
Risk Factors for Coronary Artery Disease
- smoking, obesity and overweight (especially the “apple” shaped body)
- high fat diet
- high salt (sodium) diet
- lack of exercise
- emotional stress
- family history
- diabetes
- high blood pressure.
- untreated obstructive sleep apnea
Additional Risk Factors
- chronic sleep habits of less than six hours a night
- chronic sleep habits of more than nine hours a night
- ingestion of trans fats (manmade fat found in many foods)
- insulin resistance (forerunner of type 2 diabetes).
A less invasive but accurate diagnostic tool for coronary artery disease is the CT angiogram.
The CT calcium score is also a highly regarded diagnostic tool.
 Brett Mollard, MD, completed his residency in diagnostic radiology and nuclear medicine at the University of Michigan where he served as Chief Resident. He subsequently completed a fellowship in abdominal imaging at the University of California, San Francisco (UCSF). He currently works in private practice.
Brett Mollard, MD, completed his residency in diagnostic radiology and nuclear medicine at the University of Michigan where he served as Chief Resident. He subsequently completed a fellowship in abdominal imaging at the University of California, San Francisco (UCSF). He currently works in private practice.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Cessna152

Postmenopausal Women: Fast Resting Pulse Linked to Heart Attacks

A fast resting pulse rate in postmenopausal women is correlated to a higher risk of heart attacks and coronary deaths.
But should you allow this study’s unexpected results to scare you into worrying about your heart simply because you’re past menopause and have a fast resting pulse?
What’s startling is that, according to this research, resting pulse rate in the women was able to predict coronary events (heart attack, coronary death) independent of common risk factors for heart attacks, and also independent of the level of physical activity.
Study Summary
For this study (appearing on the British Medical Journal website, 129,135 postmenopausal women were followed.
None of the women had a history of any heart problems. Resting pulse rate can be affected by certain things, such as high cholesterol, high blood pressure, drinking and smoking.
So at the beginning of the study, these items were taken into consideration.
For an average of 7.8 years, the postmenopausal subjects were monitored, and this tracking included any hospital stays that occurred as well as all coronary events.
- During the 7.8 years, the number of heart attacks and coronary deaths totaled 2,281.
- And the number of strokes reached 1,877.
Scary News
Women who had the highest resting pulse (exceeding 76 beats per minute), were substantially more likely to experience a coronary event, than were the women who had the lowest resting pulse (defined as 62 beats or less per minute).
Additional analysis revealed that this correlation (coronary event, not fast pulse) was not influenced by physical activity, or whether or not the subjects had diabetes.
However, the correlation was more pronounced in women who were 50 to 64, than in subjects over age 65. There was no correlation between resting pulse and stroke, however.
Researchers’ Conclusion
Resting heart rate in postmenopausal women independently predicts the occurrence of heart attacks as well as coronary deaths.
Is fast resting pulse as strong a predictor of heart attacks in women, as are smoking and diabetes? No.
But the researchers believe that the association is strong enough to have clinical significance.
What to Do if Postmenopausal and You Have a Fast Resting Heart Rate (76+ bpm)
“While this may be true in that there is some association, I would not advise my patients to excessively worry about their resting heart rate,” says Sendhil Krishnan, MD, a board-certified adult general cardiologist with advanced subspecialty training in interventional cardiology.
“Just being anxious and worrying about something can, in fact, lead to a higher baseline heart rate.
“It was also noted that during this study that physical activity was inversely related to a resting heart rate.
“This is a well-known phenomenon: People who are physically fit and more conditioned tend to have lower heart rates (athletes for example can have resting heart rates 10-20 beats slower than the general population).”
Though the study found that physical activity was not associated with the cardiac events, keep in mind that the faster heart rate WAS.
The study did not specifically explore postmenopausal athletes who had fast resting pulses to see if they had a higher rate of heart attacks.
“Another important thing to realize is that patients who were on medications that can slow the heart rates (beta blockers or digoxin, etc.) were excluded from this trial,” says Dr. Krishnan.
“This information would’ve been helpful because it could suggest that patients with a faster heart rate may be put on a beta blocker just to slow the pulse down. However, we do not have this data to suggest doing this at this time.
“My recommendation for any patient is to continue to do all things necessary to be cardiovascularly fit which includes proper health, exercise, not smoking, maintaining proper cholesterol levels and controlling blood pressure.
“A treadmill exercise stress test will help identify early onset of coronary artery disease and help prevent significant problems down the road.
“It’s also important to realize that a fast heart rate may be secondary to other arrhythmic conditions such as atrial fibrillation which can cause intermittent episodes of tachycardia [rapid heart rate].
“Patients should be screened with at least an EKG or even wear a portable event monitor to catch any arrhythmic events.”
The Questions this Study Begs
#1) What about a study of premenopausal women, resting pulse and heart attacks? That will span a longer period of time, but is worth it.
#2) And what about the cause of the fast resting pulse?
Wouldn’t there be a difference in association with heart attacks, if the fast resting pulse is caused by persistent anxiety in an otherwise healthy super-fit, postmenopausal woman, versus a disease process ?
 Dr. Krishnan is with Pacific Heart & Vascular, where you can view his videos on heart disease and healthy living. He has numerous publications and often speaks at local and regional events.
Dr. Krishnan is with Pacific Heart & Vascular, where you can view his videos on heart disease and healthy living. He has numerous publications and often speaks at local and regional events.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Elena Ray
Source: sciencedaily.com/releases/2009/02/090203192429.htm

Early Menopause, Heart Attack Risk: Thin Fit vs. Obese Women

The research-verdict is out that early menopause appears to double heart attack risk and increase risk of cardiovascular disease.
But does this take into consideration variables of exercise, diet, body weight and smoking history?
The research points out that cardiovascular disease, for which early menopause is a potential risk factor, is the No. 1 killer of American women.
But working hard to improve modifiable risk factors will go a long way at helping to prevent cardiovascular disease. Modifiable risk factors include:
- Dietary habits
- Exercise habits
- Smoking
- Stress management
- Sleep habits
- Blood pressure
- Cholesterol profile
The study had over 2,500 participants of varying races.
The medical definition of early menopause is having completed the process (either naturally or surgically) before a woman’s 46th birthday.
Completion of menopause is when a woman goes 12 months without menstruating, and if this happens before she turns 46, it is “early.”
Surprising News
The researchers had adjusted for modifiable risk factors.
But despite that, early menopause was determined to be an independent risk factor for a higher risk of heart attacks and other cardiac events.
The reason why this is has not been established, as this was an observational study.
Two questions should hang before the savvy health-conscious woman:
Does early menopause increase heart attack risk?
Or, does cardiovascular disease bring on early menopause?
Says Nanette Santoro, MD, Professor and E. Stewart Chair of Obstetrics and Gynecology, University of Colorado at Denver School of Medicine:
“CVD burden may well have a connection to earlier menopause, and there are a few cohort studies that have shown that. This study (Wellons) shows that in a sizable, multi-ethnic cohort – – which is meaningful.”
Question to Ask
Were the early menopause women actually divided into several groups such as 1) never smoked, 2) never were overweight, 3) long history of intense exercise, 4) long history of clean all-natural eating habits?
What would make an intriguing study?
A study in which the heart attack rates of obese early menopause women are compared to the heart attack risks of never-overweight early menopause women, and so on; it’s nearly endless as far as which groups to compose for comparisons:
1) lean, never-smoked, vegetarians
2) obese but who’ve always exercised
3) obese who never smoked
4) obese heavy smokers
5) exercise enthusiasts with low body fat
6) exercise enthusiasts with high body fat
7) exercise enthusiasts with poor stress management and frequent junk food binges.
What to Do in the Meantime
If you’re obese or even moderately overweight, don’t wait till menopause, retirement or some other distant event to start making lifestyle changes to reduce excess body fat.
Two Major Weapons Against Obesity
- Compound strength training
- High intensity interval training
The mistake that many big women make is that of using tiny weights. I’ve seen this time and time again — and it just doesn’t beget the results they’re looking for.

Trade those tiny dumbbells for a heavy barbell for optimal fat loss. Shutterstock/Lisa F. Young
The general rule is that for optimal weight loss, you must use an amount of weight that makes it absolutely impossible to complete more than 12 repetitions.
However, you should be able to perform at least eight reps.
A compound exercise is one in which more than one joint is used.

Preparing to squat, which works the glutes, thighs, hamstrings and core. Shutterstock/Reshetnikov_art
The best compound exercises are the squat, deadlift, leg press, any barbell pressing motion, and pulling movements such as the seated row.
If you’re already in the midst of menopause, or you sense that it’s around the corner, don’t let this stop you from embarking on a serious strength training program.
Not only does strength training benefit the heart, but even more so, high intensity interval training will boost heart health and significantly reduce the risk of cardiovascular disease.

Dr. Santoro has been an active clinician and researcher in reproductive endocrinology beginning in 1986.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Estrada Anton
Sources: sciencedaily.com/releases/2010/06/100621133948.htm;
endocrinetoday.com/view.aspx?rid=65730

Why Eating and Swallowing Increase Heart Rate

Ever notice an increase in heart rate when eating or swallowing?
Perhaps you can feel your heart rate increase upon eating or swallowing; or, maybe you accidentally discovered this by happening to take your pulse while eating.
At any rate, there is a distinct reason why heart rate can increase as a result of eating, which includes the act of swallowing. As far as a faster heart rate, eating and swallowing are one and the same.
“Eating and swallowing affect the autonomic nervous system,” says Teresa Caulin-Glaser, MD, a cardiologist and senior vice president with Service Lines, OhioHealth.
“The autonomic nervous system has two arms that can impact the heart rate:
1) the sympathetic system, which increases the heart rate
2) the parasympathetic, that slows the heart rate. When a person is eating and swallowing, the parasympathetic nervous system, specifically the vagus nerve, is inhibited.
“As a result of the inhibition of this nerve when eating and swallowing, there is a temporary increase in a person’s heart rate (by inhibiting the parasympathetic component of the nervous system the heart rate increases).”
So that’s the reason why heart rate increases while you are eating or swallowing.
Not knowing why this occurs can be scary for some people, particularly people who have risk factors for a heart attack, or who’ve had cardiovascular issues in the past.
Rest assured, a faster HR while eating is nothing to worry about. What you should be more concerned with is what you’re eating.
Some food items are harmful to cardiovascular health, such as trans fats, hydrogenated or partially hydrogenated vegetable oils, and saturated fats.
Read ingredients on the back of the packaging, box or can to see if these fats are in the product.
Forget what it says on the front of the package.
“No trans fat” simply means less than a minimal amount of trans fat in the serving size that’s listed on the nutrition label.
This is a manufacturer’s trick.
The real story is in the list of ingredients.
So next time your heart rate speeds up while eating and swallowing, go easy on the red meat and butter, and heavy on the whole grains, vegetables and fruits. And that’s, of course, after you exercised for a full hour.

Dr. Caulin-Glaser is an experienced physician, teacher and researcher in the specialty of cardiovascular disease, and formerly the system vice president for Heart & Vascular Services at OhioHealth.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Obesity & Overweight Cause Congestive Heart Failure?

When one thinks of obesity’s harm to the heart, it’s usually clogged arteries.
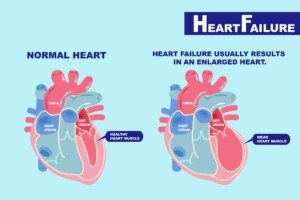
But being fat can impair the heart’s pumping action: heart failure.
- The heart fails to pump the amount of blood it’s supposed to.
- And/or, the heart’s chambers fail to fill up with the amount of blood they’re supposed to before each beat.
“Extra fat around the heart can be dangerous because of the mechanical constriction of the heart muscle,” says Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“If the heart is surrounded by fat, it can’t beat as efficiently, and that can lead to heart arrhythmias or heart failure.”
These days, “congestive” heart failure is becoming increasingly referred to as chronic heart failure, since not all patients with this common disease suffer from congested fluid in the body.
Being Fat Is As Much a Risk for CHF As It Is for Heart Attack or Stroke

Shutterstock/nger Anne Hulbækdal
Exactly how obesity creates a risk factor for congestive heart failure is not clearly understood.
Researchers believe the mechanism may be an indirect effect, in that all the extra internal fat often leads to high blood pressure, heart attack or type 2 diabetes … which all put a person at risk for CHF.
However, some researchers indeed believe that obesity has a direct effect on heart muscle.
Shutterstock/EstherQueen999
Thin people get CHF too, but you must realize that CHF has multiple risk factors. One is obesity.
Others are lack of exercise, smoking, untreated sleep apnea, and of course, high blood pressure, heart attack and diabetes.
The mechanical problem that’s created by the excess fat surrounding the heart may not be the only pathway that leads to CHF in the very overweight person.
Fat cells may behave as endocrine tissue, secreting harmful substances.
Weight Affects Heart Function
A study by Thomas H. Marwick, PhD, compared the left ventricles of normal-weight people, with the left ventricles of severely obese people.

Shutterstock/ Motortion Films
In the overweight participants, there was a very weakened ability of cardiac muscle to contract, and a diminished ability of cardiac muscle to fully relax.
The full-relax is important for enabling the ventricle to be refilled with blood during rest periods between the heartbeats.
The study showed impairments of left ventricular function in mildly obese, as well as overweight, subjects.
“The study showed a direct relationship between the level of obesity and the degree of myocardial dysfunction,” says Dr. Marwick in the paper.
And this finding was independent of other risk factors.
“We think this indicates a direct metabolic effect of obesity on the heart muscle,” says Dr. Marwick.
More than half a million cases are diagnosed in the U.S. every year, and the condition kills about 53,000 Americans yearly, as primary cause of death.
However, if congestive or chronic heart failure was named on death certificates as contributing cause of death, the annual death rate would jump to over 260,000.
Congestive failure usually starts in the left ventricle, and may be diagnosed as diminished left ventricular function.
Regular exercise (strength training and cardio) plus prevention of obesity and even overweight, will go a dynamically long way in preventing congestive or chronic heart failure.
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}