

How to Use Your Mind, Not Drugs to Stop Panic Attacks

You can stop a panic attack dead in its tracks with your MIND, without relying on drugs every again.
I’ve had only two full-blown panic attacks because by the time I started to get a third panic attack, my plan of curing panic attacks without drugs had already been set in place.
To understand how I cured panic attacks, without drugs, you’ll need to be taken through my first two panic attacks.
Contrary to popular belief, panic attacks are NOT always triggered by stress or anxiety. My first panic attack began in a dream while I was asleep.
In the dream I was with my brother, and nothing eventful was occurring.
Nevertheless, in the dream, my heart began beating faster and heavier. I then awakened to a pounding heart.
Actually, the panic attack didn’t start in the dream literally. My heart began spontaneously pounding, and this was then incorporated into my dream, like how sometimes the urge to urinate gets “scripted” into a dream.
Anyways, I awaken, and I immediately sat up, heart pounding and feeling very strange. I felt like I was about to have a heart attack.
I couldn’t shake the conviction that cardiac arrest was moments away, even though the preceding day, I had went on a grueling hike up a steep trail.
Anxiety and fear set in, my respiration increased, and my heart wouldn’t calm down.
I dialed 9-1-1 and requested an ambulance. I was in perfect health and fitness, an athlete, a weight lifter, a jogger and hiker. Yet I felt a need to dial 9-1-1 out of concern I was having a heart attack.
I did not have the foresight to bring money with me while I waited outside my apartment for the ambulance.
My heart was just pounding. I was wheeled into the ambulance, and couldn’t believe how my heart refused to stop racing.
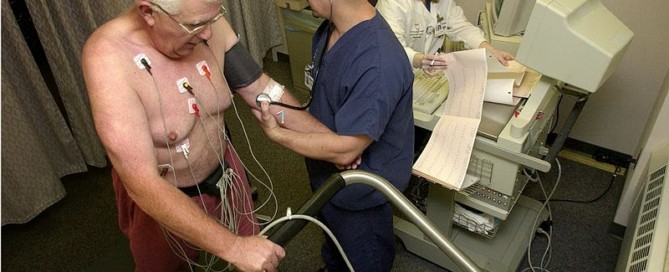
In the ER I was hooked to a heart rate monitor.
It took about two hours for my heart rate to slow down enough to where I could be discharged. Of course, the doctor said my heart was fine.
I noticed the numerical code for the diagnosis on the paperwork; I recognized it as being a code for anxiety, as I was familiar with these codes.
I couldn’t believe I’d had a panic attack and thought it would never occur again.
But not long after, another panic attack struck. Because I didn’t think I’d have another panic attack, I had devised no plan of prevention; I was caught off-guard by the second panic attack, which took place while at the workplace.
Again, no stress triggered this second episode. I had been assigned a very light workload and there were frequent periods of no work.
No Drugs!
During one of these periods I was standing but leaning over a countertop, reading a newspaper article – one that I had written, actually.
Suddenly, this feeling came over me. I immediately recognized it. It was happening again.
I straightened like a stiff board and felt like I might be dying. My heart began thumping.
My breathing seemed funny. I faced the head foreman and actually entertained the idea of asking him to dial 9-1-1.
No, I will not do that. I’ll just stick this out. I left my post without saying a word and began walking about the maze-like department, which was filled with people, several of whom I couldn’t stand.
How humiliating it would be to ask the foreman, a runt of a man whom I didn’t care for, to dial 9-1-1.
I maintained good posture, held my head high and continued walking all over the place, in the midst of a panic attack, while nobody had a clue.
I figured if I were really dying, someone would immediately dial 9-1-1, there were enough people around.
I made a few stops at the drinking fountain, and after several minutes, felt that the panic attack was subsiding.
I realized, if something were genuinely wrong with my heart, I wouldn’t be able to sustain such grueling steep hikes.
Further, if something were wrong with my heart, I’d experience cardiac arrest or angina while I was hiking, and I had to admit, my strenuous hikes always went without a hitch.
After about five minutes, I returned to my post, feeling normal again. I had out-psyched the panic attack.
For sure, I had to convince myself nothing was wrong with my heart; proof was in my hikes and heavy weightlifting.
A sick heart wouldn’t last on one of my hikes. Further, a bad heart wouldn’t get well spontaneously, either. THIS TIME, I decided, no more panic attacks. This was not going to happen again.
No Drugs Again!
Not long after, I was at the end of a hike and walking down a gravel road, my car in sight. Suddenly…that feeling came upon me. But I kept charging down the hill, pumping my arms, thinking,
Screw this. I don’t need this. I’m fit and strong. It’s all in my mind. Just ignore it. It wants my attention. It ain’t gonna get it.
Before I arrived at my car, the panic attack demon had given up on me.
The fourth – and last panic attack – occurred at night while I was awake but in bed. I bolted out of bed and began doing pushups. I intended on jogging outside, but the pushups scared off the panic attack demon.

Shutterstock/Slatan
This last panic attack attempt occurred about many, many years ago. I haven’t had a panic attack attempt since. The panic attack demon knows I’m too much work.
Don’t jump on the drug bandwagon too quickly; develop your mind over matter skills to cure panic attacks.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

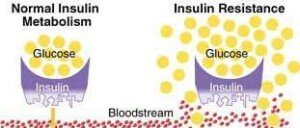
Time It Takes to Reverse Insulin Resistance?

How long would it take to reverse insulin resistance with diet and exercise?
So how long does it usually take to reverse insulin resistance with diet and exercise?
As far as how long it would take for insulin resistance to be reversed with exercise and an improved diet, there is no one-size-fits-all answer, says Craig Stump, MD, former chief of the UA Division of Endocrinology, Diabetes and Metabolism (2006 to 2016), University of Arizona, Southern Arizona VA Healthcare System.
He says, “Some people can reverse insulin resistance very easily. I have seen people improve by just cutting out fast foods or taking up a moderate walking program.
“Significant improvements can be seen in as little as 2-3 months. Indeed, a single bout of exercise in most people can improve insulin resistance for between a few hours to 24 hours.
“This is why it is often recommended that people partake in physical activity nearly every day.”
If you have not been exercising, and especially if your job has you seated for most of the time, then adding exercise to your life will be a significant variable in reversing insulin resistance if you have it.

Shutterstock/Jasminko Ibrakovic
A fasting glucose reading should be between 60 and 99 ml/dL. The range for pre-diabetes is 100 to 125.
“When glucose is elevated above 100, this is evidence that the body can no longer compensate for insulin resistance,” says Dr. Stump. Over 125 is considered diabetes.
However, it’s not that simplistic. One fasting glucose reading between 100 and 125 does not automatically get a person a diagnosis of insulin resistance.
Other factors must be considered, such as that person’s cholesterol profile, blood pressure and body weight.
A higher than normal fasting glucose reading may result from a bad night’s sleep the morning prior to the test, according to some preliminary studies (i.e., Spiegel et al).
Thus, if you plan on taking a fasting glucose test, make sure that it follows a good night’s sleep.
In an attempt to reverse insulin resistance, which is a major risk factor for type 2 diabetes, a person may not be getting the desired results, despite seemingly doing everything he or she is supposed to be doing. This includes a failure at weight loss.
Failure to lose weight can result from inefficient exercise.
For example, a man at the gym reported to me that he was not able to lose weight, despite using the treadmill faithfully.
One look at him while he was walking on the treadmill, and I instantly knew what the problem was:
He kept holding onto the equipment, and thus, wasn’t really walking at all, but just gliding through supported motions.
I told him to swing his arms; he lost eight pounds in one month without caloric reduction.
Dr. Stump says, “Some people tend to eat more (imperceptible) when they begin an exercise program (although they swear up and down that they are eating no different).”
This will interfere with weight loss attempts, and losing weight is so important for reversing insulin resistance – if you’re overweight, that is.
“Being slightly calorically negative through dietary restraint and physical activity is the best way to reduce insulin resistance,” continues Dr. Stump.
“This is nearly impossible if high caloric density foods such as fast food are plentiful.
“Other recommendations that are made are to avoid simple sugars and starches (white noodles, white rice, white bread and flour).
“Rather, it is advised to consume more complex carbohydrates and to mix these with protein and fat in a given meal.
“However, these are not uniformly accepted or recognized by medical and nutrition specialists as being effective.”
On the other hand, the fitness-professional industry swears by this protocol, that carbohydrates should be eaten with protein and “good” fats.
So if you want rice (wild, brown or basmati), have an egg white omelet cooked in olive oil with it, or a handful of nuts.
Plus, the best time for your body to metabolize any kind of carbohydrates is within 30 minutes or so of hard exercise.
To reverse insulin resistance, practice these guidelines and then have another fasting glucose reading taken (after a good night’s sleep) after a few months to see if there’s any improvement.
Dr. Stump’s research interests included insulin resistance resulting from physical inactivity, obesity and the metabolic syndrome, and identifying biological markers to predict progression of diabetes. Dr. Stump passed away in May 2019 after a brief illness.
research interests included insulin resistance resulting from physical inactivity, obesity and the metabolic syndrome, and identifying biological markers to predict progression of diabetes. Dr. Stump passed away in May 2019 after a brief illness.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can Anxiety and Stress Cause Insulin Resistance?

Wondering if insulin resistance can be caused by anxiety and emotional stress?
“Insulin resistance is when insulin is no longer able to trigger the same physiological response as it once did, or as is normal,” says Craig Stump, MD, former chief of the UA Division of Endocrinology, Diabetes and Metabolism (2006 to 2016), University of Arizona, Southern Arizona VA Healthcare System.
Insulin resistance is a forerunner to diabetes, says Dr. Stump.
If you clicked on this article, you probably already know some facts about insulin resistance, such as that “it requires more insulin to achieve the same effect as a lesser amount did under normal or insulin sensitive conditions,” continues Dr. Stump.
The primary causes of insulin resistance (or prediabetes) are lack of exercise; being overweight; and a diet with too many quick-acting carbohydrates (such as those found in any sugary foods, plus white rice, white bread and fruit juice).
Dr. Stump continues, “Stress can definitely cause insulin resistance and this is partly due to stress hormones including those produced by the adrenal gland.
“However, when I say this I am talking about severe stress such as severe injury, illness, surgery or deprivations.”
But what about stress of the psychological kind, such as the stress of daily living?

Can anxiety and stress be a cause, or even a contributing factor, to insulin resistance?
After all, stress increases production of certain hormones that, when left circulating and unopposed in the body, can be detrimental over time (e.g., high blood pressure, increased stroke risk).
“For example, anxiety may prolong the daily release of the stress hormone cortisol, which is predominantly released at dawn under normal conditions,” says Dr. Stump.
“Vigorous exercise likely opposes cortisol through a variety of mechanisms.
“Therefore, if you suffer from chronic stress while remaining sedentary, then slight but persistent cortisol elevations could contribute to metabolic dysregulation and deterioration of your health.”
Dr. Stump says he frequently hears about stress from his patients.
“They are forever blaming their lack of blood sugar control on increased stress.
” This is a much more difficult question which is fraught with potential abuse for excusing all sorts of unhealthy behavior, because if insulin resistance or poor glucose control can be blamed on ‘stress,’ then it is no longer the patient’s responsibility; it is due to outside influences beyond their control.
“This hypothesis also falters in that there are plenty of people with stress who are not insulin resistant.”
Even if anxiety and mental stress can outright cause prediabetes or insulin resistance, this does not absolve the patient from responsibility.
Because if you suffer from anxiety, this is all the more reason to ramp up physical activity.

Shutterstock/Jacob Lund
Bouts of intense physical exertion of a structured nature increase release of human growth hormone and testosterone (in ladies, too), and these potent fat-burning substances neutralize cortisol and another stress hormone, adrenaline.
And when you stick to an exercise program, you are more inspired to eat healthy foods and cut back on sugary foods.
So, with healthier eating and exercise adherence at play, what’s the invariable result?
Weight loss! With a healthier body and dramatically improved mood from exercise, you will sleep better, and sleep is very important for stabilizing blood sugar levels.
Dr. Stump explains, “The most notable and intriguing may be that relative sleep deprivation can cause insulin resistance.
“There have recently been preliminary studies suggesting that even one night of poor or inadequate sleep can make one more insulin resistant.
“On the other hand, exercise is definitely a physiological stressor that is well-known to improve insulin sensitivity.
“Whereas, remaining sedentary would not be considered ‘stressful,’ yet this is a primary cause of insulin resistance.”
In conclusion, no matter how much stress you have in your life…I’m going to be simplistic with this…but…hit the gym.
Anybody who engages in bouts of intense exercise will tell you that this does wonders for a harried, stressed-out soul.
Don’t fight anxiety and stress by overeating or filling up on sugary sodas, ice cream, cakes and cookies — which can lead to prediabetes or insulin resistance.
Dr. Stump’s research interests included insulin resistance resulting from physical inactivity, obesity and the metabolic syndrome, and identifying biological markers to predict progression of diabetes. Dr. Stump passed away in May 2019 after a brief illness.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

Insulin Resistance: How Long Does It Take to Reverse?

Insulin resistance can be reversed with diet and exercise, but how long does it usually take?
So how long should it take to reverse your insulin resistance? I asked Dr. David Edelson, MD, board certified in internal and bariatric medicine, one of the top obesity experts in the U.S., and founder and medical director HealthBridge and thin-site.com.
Insulin resistance can lead to prediabetes, which of course can morph into type 2 diabetes.
Thus, it’s extremely important to reverse insulin resistance, even though the time it takes will not occur overnight.
How long it took to acquire insulin resistance didn’t happen overnight, either.
Dr. Edelson explains, “I’ve seen our patients with early stage insulin resistance able to reverse it and normalize their fasting insulin levels in 6-12 weeks.”
The three key areas to work on, when it comes to reversing insulin resistance, are:
Weight Loss
Exercise
Changes in Diet
Dr. Edelson continues, “If you let the ‘fuse burn’ too far, it becomes harder and harder to reverse insulin resistance.”
Insulin resistance can be thought of as being on a continuum. On one end, the left side, is normal glucose metabolism.
All the way at the other end, on the right side of the continuum, is type 2 diabetes. These two points are connected by a fuse.
It ignites at the left end at early insulin resistance, but if left untreated, that lit fuse burns its way along the continuum, towards the prediabetic point, and as it progresses further down the continuum, it becomes more difficult to reverse.
Dr. Edelson says, “There also is a point where it can no longer be reversed, when the pancreas has essentially ‘burned out’ and can no longer produce enough insulin to meet the body’s needs.
“This is why it is so important to intervene as early as possible in the course of this condition.”
Weight Loss

Make sure this is loss of fat, not muscle. A “starvation” or severe calorie restriction diet won’t work long-term.
Portion control is the key. Take inventory of the kind of portions you usually have!
So practice portion control and don’t skip meals; long periods in between meals may slow metabolism in some people and sabotage fat loss efforts.
Exercise
Ancient man exercised hard nearly every day. The idea that’s been perpetrated out there, that you shouldn’t exercise every day, is full of nonsense.

Shutterstock/YAKOBCHUK VIACHESLAV
But don’t confuse this with the rule that you should not lift weights with the same muscles two days in a row.
Do an hour of exercise daily, alternating cardio days with weight days. Or replace a cardio day with yoga.
Your highest carbohydrate meal of the day should be consumed within an hour of exercise, if possible.
Diet
Avoid as much as possible foods with ingredients lists that name anything “hydrogenated” as well as sugar and high fructose corn syrup.
Eat whole fruits instead of juice as much as possible. Restrict saturated fats.

Take omega-3 fish oil supplements, vitamin D3 supplements, and a B3 supplement (niacin).
Take the fish oil and D3 simultaneously for a synergistic effect.
Stick to these guidelines and your insulin resistance will almost always be reversed within a reasonable time period.

Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

How Effective is Cymbalta for Treating Depression?

Cymbalta snuffed out my mother’s crippling depression.
Yes, the antidepressant Cymbalta literally saved my mother’s life. Cymbalta wiped out my mother’s depression and panic attacks, with no side effects save for a few brief dizzy spells at the beginning.
My mother became disabled from depression, which included a weight loss of 12 pounds (mostly muscle) from refusing to eat, and reverted to weeping over the tiniest issues.
I didn’t need medical training to recognize a textbook case of clinical depression, and I recommended an antidepressant (though not naming Cymbalta specifically).
It all began when I planned on living with my parents for about three days, to help my mother recover from knee arthroscopic surgery.
Little did I know that a power-hungry depression awaited me and would hold me hostage there for over two months.
In hindsight, I realize that subtle signs of depression had been present for several weeks preceding the surgery.
However, the depression began stomping its feet the morning of the knee surgery, and had an unforgiving accomplice: panic attacks.
My mother had had orthopedic surgeries before, but never sobbed or was convinced she was dying like this time.
The problem was merely a meniscus tear in the knee. She also complained that the fingers of both hands were tingly.
Several days after the surgery, I suspected clinical depression and I began urging my father for “psychiatric intervention,” and that “she needs an antidepressant!”
Both my mother and father adamantly opposed antidepressants.
My mother denied having depression, and attributed her apathy, overall weakness, inability to hold herself together while doing simple shopping, comments about wanting to die, excessive crying, loss of appetite and withdrawal from daily activities to:
1) post-surgical knee discomfort, and then 2) a developing pain in both hands and arms, along with continuing tingling in the fingers.
My father admitted something was wrong, but attributed it to “lingering effects of anesthesia” (even five days out from surgery), and then to the hand pain (eventually diagnosed as carpal tunnel syndrome).
Meanwhile my mother often talked about her funeral, gave us “If I die…” talks, and often said her entire body hurt.
“She has depression!” I kept harping to my father, who still opposed antidepressants and accused me of trying to play doctor.
After six weeks of taking care of my mother, including daily battles to get her to eat, I finally convinced my exhausted father to embrace an antidepressant.
I chose Cymbalta because at the time, we thought that her frequent shoulder pain (which would trigger hard sobbing) was residual nerve pain from the double carpal tunnel syndrome surgery.
In addition to nerve pain, Cymbalta is prescribed for panic attacks, and my mother often felt as though death were imminent.
I showed my father information from a Web site about how major depression can cause whole-body pain and amplify pre-existing joint pain by heightening a person’s perception of pain.
I just had a gut feeling that the Cymbalta would take out the depression like a tank.
That evening my mother took one 30 mg Cymbalta capsule. “I don’t know how long it will take before it kicks in,” I told her, “But believe me, this is the RIGHT thing to do.”
Next morning, my mother awakened feeling vibrant, pain-free, and eager for a big breakfast.
Absent was the scene for the past six weeks: a withered, crying, wasted-looking stranger. My mother’s eyes were alive, voice robust. She said, “I feel GREAT!”
I said, “It’s the drug, the Cymbalta, it worked!”
My mother needed no help sitting upright; she popped right up and got ready for the day as though nothing were wrong. “For the first time in weeks, I feel human!” she said.
And for the first time in seven weeks, she washed her hair. My father was floored by the drug’s effect.
The Cymbalta prescription was 30 mg daily for the first week, then 60 mg the second week.
The Cymbalta was working so beautifully that on the eighth evening, I kept the dose at 30 mg (I was in charge of administration).
Next day, my mother had a partial relapse and asked, “Do you think it’s because you didn’t double the dose?” I said, “Yes. Well, tonight you’re getting 60 mg.”
Early next morning while still in bed, my mother boldly said, “I feel SO strong, like I can just swing my legs off the bed and stand right up!”
She then began talking about going out for breakfast and doing some shopping to buy ingredients to make bread and meat pies — while still in bed.
Another three weeks on 60 mg worked wonderfully, and then we had to increase to 90 mg. Cymbalta restored my mother’s appetite, wiped out panic attacks, brought back her laughter, resurrected social connections, and motivated her to stick to an exercise plan.
Since taking Cymbalta, my mother has had NO “my whole body hurts” episodes, and the shoulder pain (eventually diagnosed as rotator cuff tears) has significantly diminished — or perhaps her perception of it has.
And when the shoulder pain does occasionally act up, my mother doesn’t sweat it, whereas pre-Cymbalta, she’d sob away and completely shut down.
About five weeks after starting Cymbalta, my mother’s energy level began plummeting; she felt increasingly drained and excessively sleepy, even though her mood remained normal.
We took her to the ER, and a blood test revealed a medical condition, hypothyroidism, that’s known to cause depression.
She started treatment the next day. In retrospect, my mother had been showing signs of low thyroid for several months, but we didn’t think much of the subtle symptoms.
Also, about five weeks after beginning Cymbalta, my mother signed with a new medical plan that didn’t cover Cymbalta, and thus had to gradually transition to a comparable dose of Effexor. These two unexpected developments extended my stay with my parents.
Effexor, like Cymbalta, is a seratonin/norepinephrine reuptake inhibitor. The transition from Cymbalta to Effexor was smooth, save for a disabling case of persistent dizziness on the last dose-changing day — yet despite that, my mother was upbeat.
In summary, my mother is now gradually tapering off Effexor; apparently, the depression is now under control with the treatment for that medical disorder.
There are NO problems with the Effexor tapering, and absolutely NO relapse of the depression, which is strong evidence that the depression’s underlying cause was the low thyroid.
(Original publication date: January 2010)
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Can Heavy Lifting, Squatting, Deadlifting Cause Aneurysm?
Does that nasty headache from heavy weightlifting mean you might have an aneurysm?
Sometimes heavy weightlifting (squats, deadlift, etc.) can cause a headache and make you think this is an aneurysm.
I’m a former certified personal trainer and know for certain that a headache, while doing heavy lifts, can be brought on by dehydration, even though you may not feel thirsty.
To help rule out dehydration as the cause of a bad headache that occurs during or after deadlifting, squatting or some other heavy weightlifting routine, drink plenty of water prior to working out; a tall glass worth.
- Fifteen minutes into your routine (including any warming up), drink some more water.
- Every 15 minutes drink four ounces (half a cup) water.
Also make sure that you’ve been adequately nourished throughout the day with nutritious food.
If you nevertheless develop a headache during your weightlifting or shortly after, the first possible cause may be due to an increase in the venous pressure of the brain.
A primary thunderclap headache can be caused by heavy weightlifting. And we all know how heavy and wicked a set of deadlifts and back-squatting can be.
The primary thunderclap headache is related to the vasoconstriction of the blood vessels that feed the brain.
If you’ve been worrying about an aneurysm being triggered by your weightlifting, or if you’re troubled by headaches following your workouts, even though you’ve been drinking plenty of water, speak to your physician just to play safe.
What about an aneurysm?
If you experience a sudden-onset bad headache while working out, stop immediately.
“Patients with a history of brain aneurysm or family history of aneurysm may be at increased risk of bleeding during intensive exercises like heavy lifting or weight-squatting,” says Atif Zafar, MD, medical director of St. Michaels Hospital in Toronto, Ontario, and former director of the stroke program at University of New Mexico Hospital.
A ruptured aneurysm is called a hemorrhagic stroke.
“These exercises do not cause aneurysm per se,” adds Dr. Zafar.
An aneurysm is a bulge in a blood vessel. This can remain dormant for many years, though over time, may increase in size.
The bigger it gets, the weaker its walls get, making it more prone to rupture — at any time of the day.
So if you already have an aneurysm, then there’s a small chance that heavy squats and deadlifts – by themselves — may cause it to get bigger.
However, if you have perfectly healthy blood vessels in your brain, lifting weights will NOT cause the actual formation of the bulge. Do not mix up formation with rupture.
The actual cause of formation may be genetic as well as from smoking and uncontrolled high blood pressure. And yes, there are weightlifting enthusiasts who smoke.
Hypertension rarely presents with symptoms. So even if you feel great, don’t smoke and can lift the entire gym building, get your blood pressure checked! You can do this with a home device.
• Heavy powerlifting or other styles of strength training do not cause chronic hypertension.
• A high sodium diet can lead to hypertension.
• It’s believed that in some cases, chronic high blood pressure has a genetic cause.
• Chronic hypertension can also be caused by untreated obstructive sleep apnea.
Though middle age and excess body fat can bring this out, a younger leaner person can still have it simply due to the natural structures of their throat, such as a large tongue base.
Dr. Zafar also explains, “Now if a person is taking cocaine or amphetamines or has underlying hypertension, in that case, every time they would do heavy lifting or deadlifting, naturally their blood pressure will spike even more.”
So what’s the most likely cause of a worsening, pre-existing aneurysm in someone who powerlifts?
“The long-term effect of uncontrolled hypertension or drug use can cause strokes or worsen the underlying aneurysm, rather than the primary effect of these heavy exercises,” says Dr. Zafar.
A ruptured aneurysm typically presents with a most horrible, very sudden headache that incapacitates a person.
If one eyelid is drooping with the headache, this is HIGHLY SUSPICIOUS for a rupturing aneurysm. Other possible symptoms are nausea/vomiting and confusion.

Dr. Zafar is author of the book, “Why Doctors Need to Be Leaders.” His interests include vascular and endovascular neurology, and the neurosciences.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

How a Cardiologist Can Miss Severe Heart Disease in Women

A cardiologist provides insight into how a specialist can examine a woman with severe heart disease and then tell her she’s in great shape
Cardiologists do indeed miss severe heart disease in women (men as well, but more prevalently, women).
One reason is because despite all the mounting media attention given to women’s heart disease, many doctors take the symptoms more seriously in men, and also, symptoms of heart disease in women oftentimes differ from those in men.
“Communication between doctor and patient is critical,” says Suzanne Steinbaum, MD, a New York cardiologist for 20+ years and founder of SRS heart — a groundbreaking program for womens’ holistic health prevention.
We have all heard many stories of young women who were dismissed by their doctors as being healthy, only to find out later that they had heart disease.
“It is important, from the patient’s perspective to discuss all the symptoms, and address all concerns,” says Dr. Steinbaum.
“Discussing family history is crucial in giving your doctor a true understanding of your own risk.”
Dr. Steinbaum adds, “Heart disease is invisible until is presents itself, so even if you are thin and fit, you can still be at risk.”
Diet is a big player in coronary artery disease. No matter how hard you train in the gym, you cannot out-train bad nutrition.

Shutterstock/Altagracia Art
You may look great and be able to knock off pushups and run 5Ks, but a processed-food diet and mental stress can cause plaque to build up inside your coronary arteries.
“Baseline EKG’s, echocardiograms and blood tests don’t always predict who is going to have a heart attack, and even simple stress tests without imaging studies may be misleading,” says Dr. Steinbaum.
“Communicating symptoms and changes in activity levels might be the first clues that there are cardiac problems.”
Unfortunately, though some women are aware of recently-new symptoms, they don’t connect them to possible severe heart disease.
My mother experienced shortness of breath for months and attributed this to narcotic painkillers, which CAN cause labored breathing
Then one morning she upchucked, after suffering shortness of breath, and still, did not make a connection.
My father even questioned her on what she ate the day before! Severe coronary plaque buildup was the last thing on their minds at this point.
However, the vomiting tipped me off and I took her to the ER where she was diagnosed with reflux disease and released!
Two days later I took her back for chest pains. She was admitted, and the next day I was told by three doctors that a massive heart attack was imminent due to blockages of at least 97 percent in five coronary arteries.
Ten months prior, my mother’s cardiologist (not one of the three) told her, “You’re the last person I’d ever think would have a heart attack.” Ten months later she had emergent quintuple bypass surgery.
Dr. Steinbaum says, “Sometimes your sixth sense tells you somethingis significantly wrong. As a patient, you must empower yourself.”
One way a woman can do that is to undergo a calcium score test which is pretty accurate for determining the likelihood of coronary artery disease, and near-future heart attack, which kills about 267,000 U.S. women every year – over six times the rate of breast cancer death.

Dr. Steinbaum has been awarded a New York Times Super Doctor, a Castle and Connolly Top Doctor for Cardiovascular Disease, and New York Magazine’s prestigious Best Doctors in the New York edition. She is on the NYC Board of the American Heart Association.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Depositphotos.com
Source: womensheart.org/content/HeartDisease/heart_disease_facts.asp
High Calcium Score but Normal Stress Test: Should You Worry?

So your calcium scan score is high, but your stress test was negative and showed no diminished blood flow through your coronary arteries.
Are you off the hook?
Do you wonder about the implications of a high coronary calcium score and a normal-result stress test (either chemical or exercise) in the same patient?
After all, a stress test measures blood flow through the coronary arteries.
A stress test does not show plaque buildup, including the “soft” type of plaque, which is the type that has the potential to rupture and cause a heart attack.
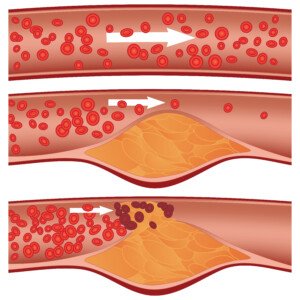
Soft plaque rupture. Shutterstock/Diamond_Images
For such a patient with both findings (high calcium score but normal stress test), Larry Santora, MD, explains:
“Never assume all is well. Look it as a great opportunity to change your life and make things better.”
Dr. Santora is a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
He explains, “You cannot ignore the calcium or plaque, but now that you have identified it and you know what your heart is like, there is no longer any question that you have coronary disease. You can take charge; you can now control it.”
There is a third variable, besides the high calcium score and the normal stress test: absence of symptoms (e.g., chest pain, difficulty breathing).
Suppose a patient has a really high calcium score, but the stress test is normal, and he or she is not experiencing any symptoms and even “feels fine.”
Dr. Santora says that such a patient does “not need an invasive angiogram or stent or bypass surgery.”
In fact, the general consensus is that if the stress test is normal, the patient has no symptoms, but the calcium score is high, it is not warranted to have an elective bypass surgery or even stent procedure.
But does this come to terms with the phenomenon that sometimes, the first symptom of severe heart disease is a heart attack?
Is it smarter to wait to see what might happen?
Should this patient undergo the invasive catheter angiogram which carries the risk of heart attack and stroke?
After all, a high calcium score means something is wrong.
Perhaps a CT angiogram is in order, to get a clearer picture of the arteries and see how much soft plaque (the dangerous plaque) there is.
Only problem is that if the calcium score is high enough, this will contraindicate a CT angiogram; the presence of all that calcium will obscure the imaging.
So what should the patient do?
Dr. Santora says, “You need to make lifestyle changes and be on a combination of cholesterol medications (even if cholesterol is normal) to prevent the plaque from progressing, or worse, suddenly rupturing and causing a heart attack.

Freepik.com/schantalao
“The calcium score (think of it as a plaque score) tells us: how low to get your cholesterol and the types of cholesterol medications, and how frequently to get a stress test; for instance, if you have zero calcium you do not even need a stress test if you have no symptoms.”
Just when you thought the plan sounds simple, keep in mind that taking a cholesterol-lowering drug to prevent plaque progression doesn’t guarantee this result.
For example, a person has a calcium score of 450, which is considered high risk for heart attack, or severe heart disease.
He or she goes on a statin drug to help prevent plaque progression.
Over the next 10 years, the patient doesn’t bother with follow-up calcium scans, but finally has a second calcium scan 10 years later:
The score is nearly 1200. Yet all this time he’d been on the cholesterol-lowering drug.
What happened?
These drugs do not guarantee prevention of further plaque buildup, especially if the patient has a junk food diet.
The coronary calcium score is the “total amount of plaque in all the arteries and gives a very good prediction of heart attack risk over 10 yrs (that is, long-term risk), and chance of short-term risk, that is, what is the chance of having an abnormal stress test due to the artery being significantly narrowed,” says Dr. Santora.
And then there is the coronary calcium percentile, which “reflects how aggressive your atherosclerosis is.”
Dr. Santora explains, “If you have a percentile of 75%, that means you have more plaque than 75% of others of similar sex and the same age. You need aggressive treatment.”
Aggressive treatment starts with setting goals.
Dr. Santora says that the HDL cholesterol should be greater than 50; and the LDL cholesterol should be less than 70.
The LDL in this case should be less than 70 “if you have a high score (>300 or percentile >70%),” adds Dr. Santora.
“However, if the score is zero, then an LDL cholesterol <160, near 130, is fine. A big difference in your cholesterol based on calcium score.”
Diet should consist of a moderate amount of carbohydrate (about half of total calories), and slow-absorbing carbs at that; 25% protein and 25% “healthy fats” like olive oil and safflower oil.
The patient is prescribed a statin.
Dr. Santora adds, “If the percentile is >75%, we order an advanced lipid panel to look for LDL size, HDL subtypes, and Lp(a); these abnormalities respond to niacin which, when added to a statin, provides the best chance in preventing plaque progression.”

Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

CT Calcium Scoring & Radiation Cancer Risk: EBCT vs. 64 Slice

Fear of radiation exposure keeps some people from getting a calcium score done for their coronary arteries.
The calcium score is a strong predictor of likelihood of a future heart attack. The equipment used for calcium scoring is the CAT scanner, also known as “CT.”
The amount of radiation delivered during most CT calcium score tests is 2-3 millisieverts up to 8 millisieverts (msvs).
A millisievert is a unit of radiation emission. We are exposed to radiation all around us, and a year’s worth of radiation, in general, amounts to around 3 millisieverts.
You may have heard about a recent study that concludes that the risk of getting cancer from a CT scan is “one in 1,000.”
However, this study leaves several questions, such as how many CT scans would it take to produce this result?
And what about the length of time in between each CT scan? What about age of the patient? What about type of CT scanner (msvs delivered)?
Regarding the one in 1,000 conclusion, “There is no reliable statistic for this and I believe the fear is well-overblown,” says Dr. Larry Santora, MD, a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
He explains, “That being said, it is wise to adhere to the lowest radiation dose possible. There are various types of CT scanners.
“The premier and fastest scanner for coronary calcium screening is the EBCT ( also called ULTRAFAST CT).”
EBCT stands for electron beam computed tomography.
Dr. Santora continues, “This is the gold standard for coronary calcium screening, the fastest and most accurate, and the lowest radiation dose, about the equivalent of two chest X-rays.
“The standard CT scanners are called a spiral or multi-detector CT scanner, like the ‘64 slice CT,’ which can also be used for calcium screening, but are less accurate and much higher radiation, about 15 to 30 chest X-rays of radiation.”
Dr. Santora’s group at the Orange County Heart Institute has been using only EBCT scanners for coronary calcium scoring for 15+ years.
The Institute, however, uses the 64 slice for CT angiography for the coronary arteries, to measure for possible narrowing and levels of “soft” plaque.
“The cancer risk from an EBCT heart scan is infinitesimally small,” he continues.
How many millisieverts of radiation does an EBCT calcium scoring emit? Six-tenths of a millisievert.
This is less than one dental X-ray, says Dr. Santora, or the equivalent of one abdominal X-ray.
A much lower radiation dose isn’t the only benefit with EBCT.
Dr. Santora explains, “The X-ray beam comes only through the patient from behind throughout the back, whereas regular CT spirals (multi-detector CT like 64 slice) go around.
“The thyroid and breast tissue are the most sensitive organs to radiation, so with EBCT they get very little radiation, while they get a lot with other CT.
“So EBCT is overall less radiation, and the most sensitive organs get a lot less.”
Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Brian A Jackson

Can You Be Too Young to Have Calcium Buildup in Heart Arteries?

How young is too young to have measurable plaque buildup in the coronary arteries?
A coronary artery calcium score exam has been proven to be very reliable at predicting the likelihood of a coronary event such as a heart attack, one to three years out from having the exam.
I wondered, however, if a person can be too young to have a buildup of calcium in their coronary arteries; I don’t mean as in toddler young, but more like young adulthood or teenage-hood.
“I think you mean at what age does calcified plaque develop. It is rare to see calcified plaque in men younger than 30 or woman younger than 35,” says Dr. Larry Santora, MD, a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
Dr. Santora continues, “We start to develop very minor ‘fatty streaks’ as the earliest development of atherosclerosis in our early 20s.”
Atherosclerosis is the term for plaque buildup in arteries.
Dr. Santora continues, “This was determined during autopsies on Korean War Vets. We usually do not do EBCT scans on men younger than 35 or woman younger than 40 since it is unusual to see calcification in the plaque at ages younger than this.”
EBCT is electron beam computed tomography, a type of CAT scan that is used for calcium scoring (and other imaging studies).
EBCT emits lower radiation than does the more common 64-slice CAT scanner.
“The radiation is equivalent to 2-3 chest X- rays using EBCT scanners, vs, 10-15 chest X-rays for conventional CT scans,” says Dr. Santora.
“In addition, the radiation beam comes from behind the back, exposing very little radiation to breast and thyroid, using EBCT, whereas the X-ray beam encircles the body when using conventional CT.”
There are exceptions when it comes to getting coronary calcium buildup at an early age, continues Dr. Santora.
He explains, “…dialysis patients, juvenile diabetics who smoke, anabolic steroid abusers, and those with familial hyperlipidemias who have family history of heart attacks in their 30s.” Hyperlipidemia is excess fat in the circulating blood.
- About 75 percent of women age 45 to 49 are found to have a coronary calcium score of zero, meaning no measurable atherosclerosis.
- Over 95 percent of women age 30-34 have a coronary calcium score of zero.
- For men in this age group, it’s close to 90 percent.
- For men under 30 it’s 99 percent. Dr. Santora says, “Atherosclerosis is a very unusual cause of death in someone under 25 years old.”
This doesn’t mean that young adults and teens have a green light for living on a junk food diet, smoking and avoiding exercise.
A young adult may have a zero coronary calcium score, and thus think he or she can get away with regularly eating heart-harmful foods and not exercising.
But the predictive factor of calcium scoring is short-term (1-3 years), and 10 years down the road, that young adult who feels invincible may end up having a growing problem inside his or her arteries.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}