

So your calcium scan score is high, but your stress test was negative and showed no diminished blood flow through your coronary arteries.
Are you off the hook?
Do you wonder about the implications of a high coronary calcium score and a normal-result stress test (either chemical or exercise) in the same patient?
After all, a stress test measures blood flow through the coronary arteries.
A stress test does not show plaque buildup, including the “soft” type of plaque, which is the type that has the potential to rupture and cause a heart attack.
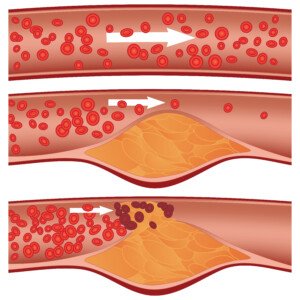
Soft plaque rupture. Shutterstock/Diamond_Images
For such a patient with both findings (high calcium score but normal stress test), Larry Santora, MD, explains:
“Never assume all is well. Look it as a great opportunity to change your life and make things better.”
Dr. Santora is a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
He explains, “You cannot ignore the calcium or plaque, but now that you have identified it and you know what your heart is like, there is no longer any question that you have coronary disease. You can take charge; you can now control it.”
There is a third variable, besides the high calcium score and the normal stress test: absence of symptoms (e.g., chest pain, difficulty breathing).
Suppose a patient has a really high calcium score, but the stress test is normal, and he or she is not experiencing any symptoms and even “feels fine.”
Dr. Santora says that such a patient does “not need an invasive angiogram or stent or bypass surgery.”
In fact, the general consensus is that if the stress test is normal, the patient has no symptoms, but the calcium score is high, it is not warranted to have an elective bypass surgery or even stent procedure.
But does this come to terms with the phenomenon that sometimes, the first symptom of severe heart disease is a heart attack?
Is it smarter to wait to see what might happen?
Should this patient undergo the invasive catheter angiogram which carries the risk of heart attack and stroke?
After all, a high calcium score means something is wrong.
Perhaps a CT angiogram is in order, to get a clearer picture of the arteries and see how much soft plaque (the dangerous plaque) there is.
Only problem is that if the calcium score is high enough, this will contraindicate a CT angiogram; the presence of all that calcium will obscure the imaging.
So what should the patient do?
Dr. Santora says, “You need to make lifestyle changes and be on a combination of cholesterol medications (even if cholesterol is normal) to prevent the plaque from progressing, or worse, suddenly rupturing and causing a heart attack.

Freepik.com/schantalao
“The calcium score (think of it as a plaque score) tells us: how low to get your cholesterol and the types of cholesterol medications, and how frequently to get a stress test; for instance, if you have zero calcium you do not even need a stress test if you have no symptoms.”
Just when you thought the plan sounds simple, keep in mind that taking a cholesterol-lowering drug to prevent plaque progression doesn’t guarantee this result.
For example, a person has a calcium score of 450, which is considered high risk for heart attack, or severe heart disease.
He or she goes on a statin drug to help prevent plaque progression.
Over the next 10 years, the patient doesn’t bother with follow-up calcium scans, but finally has a second calcium scan 10 years later:
The score is nearly 1200. Yet all this time he’d been on the cholesterol-lowering drug.
What happened?
These drugs do not guarantee prevention of further plaque buildup, especially if the patient has a junk food diet.
The coronary calcium score is the “total amount of plaque in all the arteries and gives a very good prediction of heart attack risk over 10 yrs (that is, long-term risk), and chance of short-term risk, that is, what is the chance of having an abnormal stress test due to the artery being significantly narrowed,” says Dr. Santora.
And then there is the coronary calcium percentile, which “reflects how aggressive your atherosclerosis is.”
Dr. Santora explains, “If you have a percentile of 75%, that means you have more plaque than 75% of others of similar sex and the same age. You need aggressive treatment.”
Aggressive treatment starts with setting goals.
Dr. Santora says that the HDL cholesterol should be greater than 50; and the LDL cholesterol should be less than 70.
The LDL in this case should be less than 70 “if you have a high score (>300 or percentile >70%),” adds Dr. Santora.
“However, if the score is zero, then an LDL cholesterol <160, near 130, is fine. A big difference in your cholesterol based on calcium score.”
Diet should consist of a moderate amount of carbohydrate (about half of total calories), and slow-absorbing carbs at that; 25% protein and 25% “healthy fats” like olive oil and safflower oil.
The patient is prescribed a statin.
Dr. Santora adds, “If the percentile is >75%, we order an advanced lipid panel to look for LDL size, HDL subtypes, and Lp(a); these abnormalities respond to niacin which, when added to a statin, provides the best chance in preventing plaque progression.”
If this article provided you with helpful information or reassurance, please consider supporting my work through Ko-fi. Donations help me continue writing detailed medical content that’s easy to understand.

Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

































