

How Stress & Anxiety Cause Acid Reflux
Learn about mechanisms behind stress or anxiety causing acid reflux.
You may know full-well that acid reflux can be caused or triggered by anxiety and stress. But just how does this work?
“Stress may cause increased vagal nerve stimulation in the brain, which may lead to increased acid production in the stomach,” says Jonathan Zinberg, MD, chief of gastroenterology at South Nassau Communities Hospital, Oceanside, NY.
This was his first thought regarding this under-researched phenomenon.
Dr. Zinberg then explains, “There are many theories regarding stress and heartburn. Some say that increased cortisol/epinephrine leads to less blood flow to the stomach, with slow digestion and emptying of the stomach, with subsequent reflux.”
He continues, “Some point to decreased prostaglandin [a hormone] in the stomach, which helps to protect the lining of the stomach (so what?).
“Others blame stress for causing general poor habits (drinking alcohol, eating fatty foods, late bingeing and smoking) for causing worse reflux (maybe in some).”
Research Lacking
“There is little evidence for any of this,” says Dr. Zinberg. “The theory I mentioned about the vagus nerve sounded good, but I found no evidence for that either [after digging further into this after I sent in a few follow-up questions].
“In fact, a scientific study from 2005 showed no evidence for increased acid reflux at all during stress, despite increased symptoms of heartburn.
“So stress probably causes an increased perception of pain from minor stimuli rather than actual increased reflux.”
This may very well apply to some individuals, while others will swear that stress or anxiety (acute or chronic) is strongly associated with symptoms that clearly spell acid reflux.
I myself once developed what could only be acid reflux making its way into my throat and causing a cough every few minutes.
It’s no coincidence that at the time the cough developed, I was facing a colonoscopy to find out why I had sudden-onset diarrhea and weird-looking stools (I feared colon cancer).
And the procedure was two days after my beloved dog was euthanized for brain cancer — after I spent eight agonizing weeks trying to save him.
If this isn’t severe chronic anxiety and stress, I don’t know what is.
The cough vanished immediately after the gastroenterologist told me that everything looked normal, and it never returned.
I also developed a mild burning in my upper abdomen, plus dull aching in my chest, that coincided perfectly with the onset of a urine and feces stench that began invading my home through the ventilation and pipes — from the hoarder neighbor next door who was literally living in his wastes and accumulated garbage.
I was told by several authorities that nothing could be done about this.
I was faced with living with this disgusting foul odor in my own home indefinitely.
I was on the phone for hours on end with every conceivable authority in an attempt to get the neighbor evicted. If this isn’t extreme anxiety and stress, I don’t know what is.
The acid reflux symptoms vanished (and never returned) the day the police chief contacted me with news that the landlord was served a notice to remove the tenant within 72 hours!
How do stress and anxiety cause acid reflux? Maybe the best answer is: You decide.
 Jonathan Zinberg, MD
Jonathan Zinberg, MD Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Cause of White Sticky Slime in Mouth Walls & Prevention

Finally, an explanation for what causes that gooey, white, slimy substance inside the walls of your mouth.
As annoying as that white, sticky and gooey substance inside the walls of your mouth is, it’s actually not a medical issue and nothing to worry about.
Yes, it’s gross, and it’s embarassing when it makes its way to the corners of your lips and someone asks you about it.
But other than inconvenience and potential embarassment around other people, that gooey stuff is actually nothing to worry about in terms of your health.
What causes the white, sticky substance inside the mouth?
“Oral mucosa, like skin cells, will slough off as newer mucosal or skin cells develop,” explains Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
“This can be exacerbated by certain mouthwashes and toothpastes.
“Especially if the toothpaste or mouthwash is in for an excessive period of time. This is similar to exfoliating the skin.”
If you’ve had the problem of a white, slimy and sticky goop inside your mouth, have you noticed it forms after you’ve brushed your teeth or used a mouthwash?
Your Toothpaste Could Be Causing a Sticky White Slime
Toothpaste can sometimes cause a white, slimy substance to form inside the mouth, which may be due to a few different factors.
1. Sodium Lauryl Sulfate (SLS): Many toothpastes contain sodium lauryl sulfate, a common foaming agent.
For some people, SLS can cause irritation or a reaction in the mouth’s soft tissues, leading to the formation of a white, mucous-like substance.
This reaction can result in a slimy or coating effect inside the mouth. Avoid toothpastes that contain this chemical.
2. Oral Mucosa Reaction: The mouth’s mucous membranes might react to certain ingredients in the toothpaste, such as flavorings, preservatives or fake colorings.
3. Dry Mouth: Toothpaste can sometimes contribute to dryness in the mouth, particularly if it contains alcohol or other drying agents.
Dry mouth can lead to an accumulation of dead cells and bacteria, which may appear as a white film.
4. Bacterial Growth: A white, slimy goo could also indicate an overgrowth of bacteria or yeast in the mouth, which might be aggravated by certain toothpaste brands ingredients.
Switch toothpaste brands and see what happens. Not all toothpastes are the same. The one that finally works best for you may be pricier, but the extra cost will be well worth it.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Alexander Raths

Under-Eye Wrinkles: Have Surgery; TCA Peel Won’t Work

A TCA peel won’t work for under-eye wrinkles, says a plastic surgeon.
A big question out there is:
Does a TCA peel work for wrinkles under the eyes?
“TCA is an excellent peel, but it doesn’t work for under-eye wrinkles,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
“This is usually caused by thinning of the skin and weakening of the under-eye muscle, or even the bulging of under-eye fat, all of which can be improved surgically.”
How does a TCA peel work?
Dr. Gabriel explains, “TCA is a great way of rejuvenating the skin. It works by removing the top layers of the skin and after the skin sloughs (3-7 days), the new rejuvenated skin is exposed.
” This helps with pigmentations and melasma and can overtime support with regenerating collagen as long as other prescription products are used in conjunction such as retin-A.
“However, under-eye wrinkles are multifactorial and generally a surgical treatment is needed to correct the deformities already stated. Combination of skin treatments and surgery is ideal, as it will add to the longevity of the results.”
How to Minimize Under-Eye Wrinkles in the First Place
You should be very cognizant of what your hands and fingers do when they make contact with your face.

Freepik.com
Do you ever rub or scratch at the skin below your eye? This pulling action, when done too much and over time, can loosen the skin.
What about how you clean the skin below your eye? Does this involve any pulling, e.g., rubbing at the area with a Q-tip swab in an attempt to remove dirt or makeup?
What about when you’re at the computer with your face in a palm? This, too, can elongate the skin.
Be alert to how you sleep. Sleeping on your side can stretch the delicate skin underneath your eye!
Finally, be very gentle and patient when you apply creams in the skin under the eye, such as sunscreen or moisturizer.
Don’t rub it in. Dab it on with the pad of a fingertip.
 Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Sylvie Bouchard

Why Age Spots Can Return after a TCA Peel

Learn how many TCA peels you need in order to get rid of brown (age) spots and why they might return.
Age spots typically appear on the face and hands, and they may resemble freckles or little moles.
An age spot is also known as a “sun spot.”
These lesions are the result of excessive sun exposure, which may take decades to start showing.
Another name that’s often used to refer to a sun or age spot is lentigo (plural: lentigines).
Age spots are harmless, but any new spot that resembles a mole should be examined by a dermatologist.
The TCA Peel and Age Spots
A TCA peel can get rid of brown or age spots, which “are due to pigment cells that have been trapped in the upper layer of skin,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
“By exfoliating the surface of the skin and exposing the undamaged underlying smooth skin, the brown spot is removed with top layer skin,” adds Dr. Gabriel.
“Allowing the natural cycle of skin to continue and peeling every 30 days, can lead to an enhanced skin texture with less brown and aged spots.
“Multiple peels may be needed to achieve the final results.”
Why might age spots reappear after a TCA Treatment?
“Benign spots can reappear if there is over-stimulation of cells that produce pigment,” says Dr. Gabriel.
The cells that produce pigment are called melanocytes. The pigment is called melanin.
“Controlling this with a prescription bleaching medication that is included in the skin care regimen is critical,” says Dr. Gabriel.
“Therefore, when one discusses skin concerns, an overall treatment plan for rejuvenation should be outlined.”
In addition to the face, TCA peels can be done on the neck, chest, back, the arms and the legs.
However, if age spots are located on the face, the success of a TCA peel is better than it is on other parts of the body.
This is due to the face’s skin having better natural healing abilities.
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Accutane & Rhinoplasty: Plastic Surgeon Gives Instructions

A plastic surgeon gives advice about Accutane following a rhinoplasty (nose job).
Accutane is a drug that is commonly prescribed for the treatment of acne.
A regular user of Accutane for this purpose may wonder if there should be changes in the use of this medication after undergoing a nose job.
Is it safe to take Accutane after a rhinoplasty?
“This depends on the physician who did the surgery, as they would know how extensive the rhinoplasty was, and also on the prescribing physician, as they would have to make sure that everything has healed and there are no contraindications,” explains Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
“The tip of the nose would be the concern, as this is sebaceous [contains a lot of sebaceous glands] and would be affected by Accutane.”
Sebaceous glands are small glands in your skin that secrete a lubricating oily substance called sebum into the hair follicles to lubricate the skin and hair.
Yes, your nose has hair follicles — plenty of them. It just doesn’t seem that way because the hair on your nose is light and very short. But it’s there.
Dr. Gabriel continues, “I would wait six months minimum before starting Accutane after facial surgery, given the fact that the scars are still healing and Accutane can significantly impact the healing phase.”
If you have not yet had your rhinoplasty, write down the questions about Accutane that you would like to have the answers to — and present them to the surgeon who is going to perform your nose job.
Make sure that your rhinoplasty surgeon and the physician who prescribed the Accutane are in communication with each other.
Then follow your doctors’ orders after the surgery. You may be instructed to gently massage, with your fingertips, your healing nose postoperatively for a while to aid in the healing process.
Side effects of Accutane include:
• Dry Skin and Lips: One of the most frequent side effects is severe dryness of the skin and lips, often leading to chapped and peeling areas.
• Dry Eyes and Nose: Accutane can cause dryness in mucous membranes, resulting in dry eyes, irritation, and nosebleeds.
• Increased Sensitivity to Sunlight: The medication can make your skin more sensitive to UV rays, increasing the risk of sunburn.
• Joint and Muscle Pain: Some users experience aches and pains in their joints and muscles, which can range from mild discomfort to more severe pain.
• Headaches: Frequent or severe headaches can occur as a side effect of Accutane treatment.
• Nausea and Digestive Issues: Gastrointestinal symptoms such as nausea, vomiting, and abdominal discomfort may arise.
• Mood Changes: There is a potential for mood swings, depression, or anxiety.
Although a direct link between Accutane and severe psychiatric symptoms is debated, it’s important to monitor any significant mood changes.
• Hair Thinning: Some users report thinning hair or temporary hair loss during treatment.
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Evgeny Atamanenko

What to Do about Hard Tip of Nose after Rhinoplasty

A plastic surgeon offers advice about a hard nose tip after a rhinoplasty…
It’s common for the tip of the nose to be hard after a rhinoplasty.
This is normal, and its occurrence depends on “what procedure was done, whether it was grafting, sutures to bring the tip together, all of which can lead to scar, and it takes 1-2 years for any scar to soften up,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
Why does the end get hard after a rhinoplasty?
“The firmness of the tip allows for stabilization of the tip until the scar matures and softens.
“Generally, it is not recommended to massage the area aggressively, as it can displace and deform the tip.
“After the splint removal, swelling can persist for months, and one has to remain patient throughout the healing phase which can last up to one year.”
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Breast Spasm Pain after Augmentation: Solutions

Find out what you can do about painful spasms after breast augmentation surgery.
“Depending on where the implant was placed, it [pain] could be due to occasional spasms that one would have,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA..
“This is just more noticeable as weight (implant) is pushing against the muscle.”
How long might these painful breast spasms last?
“It is very difficult to assess without a history and exam and I recommend for one to see a board certified plastic surgeon.
Treatment for breast spasm pain from augmentation?
“During the first three months, the spasms are more common and can be daily,” says Dr. Gabriel.
“Stretching the chest and being involved in yoga and Pilates will minimize the spasms.
“It is important to have a good posture and not allow the shoulders ‘roll in.’ It is important to always stretch the pectoralis muscle. Think of a ‘Charlie Horse.’
“We stretch against it to lengthen the muscle; the same should be done with the muscles of the chest.”
Tingling
“The first year as the internal scar is maturing and nerves are regenerating, the internal ‘tingling’ can be noticeable.
“After the first couple of years, spasms and tingling will be minimal but still present since it would have been present with or without the implant.”
A qualified surgeon can be found on this website: plasticsurgery.org
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Theerapol Pongkangsananan

Breast Augmentation: Dissolvable Stitches not Dissolving?

A plastic surgeon explains what to do about stubborn dissolvable stitches following breast augmentation.
You’ve had breast enlargement surgery and were sutured with dissolvable stitches—but they’re not dissolving. What’s going on here?
“Depending on what type of suture was used to close the incision, the sutures can last anywhere from three weeks to nine months,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
“During this time, thick scar tissue can form around the sutures and it will take one to two years for the scars to soften up,” he continues.
“Massaging the scar and pinching the scar will help expedite the sutures, and scars soften.”
Type of Sutures in Breast Augmentation
“It is generally preferred to use a longer lasting suture in areas of more tension such as a tight incision where the implant is pressing against it,” says Dr. Gabriel.
“This will also improve the scar long-term, as it will have fewer tendencies to stretch.
“Using shorter lasting sutures may affect the quality of outside scar. So there is a fine line between what we feel and what we see.
“Feeling a thicker scar that can be massaged is probably preferred over having a stretched-out, discolored outside scar that may last forever.”
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Kanashkin Evgeniy

Ears Blocked in the Morning: Causes & Solutions

Find out from an ENT doctor what you can do about blocked ears in the morning and what causes this.
Ever awaken with one ear “blocked” or both of them?
“Causes of blockage in the ears are wax impact in the ear canals, middle ear fluid and Eustachian tube congestion,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
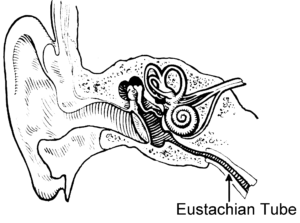
“The Eustachian tube allows air to go from the back of the nose to the middle ear,” continues Dr. Silvers.
“When the tube is clogged or congested the ear feels blocked with occasional pressure.”
What else can cause this annoying symptom?
“Allergies or a cold are usually contributing factors,” continues Dr. Silvers.
“Flying with a bad cold can cause fluid in the ear that might not be fully felt until the morning.
“Eustachian tube congestion can be treated with Sudafed, and it can be prevented with decongestants if you have a cold or nasal congestion, or allergy medication if you have allergies.”
As the day goes on, this symptom will eventually dissipate.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Estrada Anton

Why Ear Pain Can Be Caused by Sinus Problems

If you’ve been wondering if the pain in one or both of your ears can be coming from something wrong in your sinuses, you may very well be correct.
But it’s important to realize that this particular symptom — persistent ear pain — can have any number of possible causes (including serious such as a brain tumor or throat cancer) that are unrelated to the sinuses.
Another unrelated cause, believe it or not, is TMJ (temporomandibular joint) disorder.
A problem with the jaw joint can radiate pain to the ear, since the pivotal area of the jaw is located very close by.
Infection is always a consideration, but should respond very well and quickly to a course of antibiotics.
Other benign causes unrelated to the sinus include acid reflux, allergies, arthritis of the neck (cervical) spine, earwax buildup and an impacted tooth.
If your ear pain persists despite being told by an ENT doctor that there is nothing going on with your sinus cavities, then you should pursue this symptom with your primary care physician.
Connection Between Sinus Problems and Pain in the Ears

Shutterstock/Elen Bushe
“Sinus problems commonly cause ear pain,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
“The nasal and sinus linings are the same membranes that line the Eustachian tube,” explains Dr. Silvers.
“The Eustachian tube ventilates the middle ear. When the nasal or sinus lining is a little swollen or congested, the ear tube (Eustachian tube) can be swollen as well.
“This leads to negative pressure in the middle ears which can lead to pressure and/or ear pain.”
Additionally, continues Dr. Silvers, “Nasal blockage from congestion or a deviated septum can decrease airflow through that side of the nose and reduce air that gets into the Eustachian tube on that side. This can cause ear pain.”
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}