
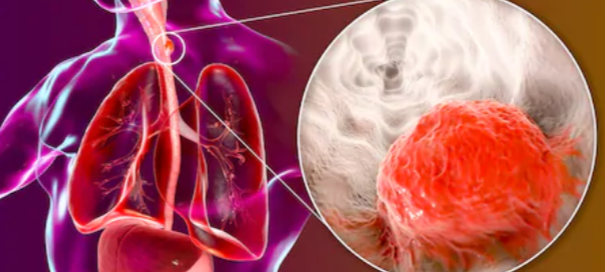
How Many Americans Under 65 Get Esophageal Cancer Every Year?
A GI doctor addresses the question of percentage of people younger than 65 years who develop esophageal cancer.
*****
Even though esophageal cancer is most prevalent in people over the age of 65, this does not mean that younger adults can’t develop this disease.
“The following is from a SEER database, and represents data collected between 2005 and 2009,” says Steven Fleisher, MD, a gastroenterologist in Rosedale, Maryland, with 20+ years of experience.
The Data
Dr. Fleisher explains, “From 2005-2009, the median age at diagnosis for cancer of the esophagus was 68 years of age.
- Approximately 0.0% were diagnosed under age 20
- 0.3% between 20 and 34
- 2.3% between 35 and 44
- 12.2% between 45 and 54
- 26.1% between 55 and 64
- 27.4% between 65 and 74
- 23.7% between 75 and 84
- 8.0% 85+ years of age.”
You may be wondering why the percentage drops as the age exceeds 74, since the older one gets, the weaker their body’s cancer surveillance system gets.
The drop in percentage reflects (not necessarily to the full degree) the fact that many people simply do not live beyond age 75 due to succumbing to America’s No. 1 killer: heart disease.
Other cancers, followed by stroke, also take out a significant number of people every year before their 75th birthday.
It is also believed by many researchers that if one’s genes (“super genes”) allow them to live past 85, they would not be as vulnerable to malignancies.
Acid Reflux and Esophageal Cancer
“The type of esophageal cancer associated with GERD is called adenocarcinoma,” says Dr. Fleisher.
“This type of esophageal cancer has been rising in incidence in the United States over the last three decades, particularly in Caucasian men.
“Between 2000 and 2004 one U.S. cancer registry had the incidence of adenocarcinoma of the esophagus in white men at 5.69 per 100 000.
“GERD is a risk factor for adenocarcinoma, and a history of heartburn is found in up to 60% of those diagnosed with esophageal adenocarcinoma.”

Dr. Fleisher was named a 2015-2018 “Top Doc” by Baltimore Magazine for gastroenterology.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Kateryna Kon
How Long Can Esophageal Spasms Last?
Find out what a gastroenterologist says about how long or short an esophageal spasm might last.
*****
You may be wondering for how long or for how brief an esophageal spasm may be.
They can be quite painful, but at other times the pain can be at a more moderate level.
The “Esophageal Spasm”
“‘Esophageal spasm’ is a lay term,” begins Steven Fleisher, MD, a gastroenterologist in Rosedale, Maryland, with 20+ years of experience.
“It implies some form of discomfort, or clinical symptom such as difficulty swallowing associated with or purportedly due to abnormal function of the esophagus with intense or abnormal contraction or ‘spasm.’”
Dr. Fleisher says that an esophageal motility study is the “best test of esophageal dysfunction supporting evidence of increased pressure in the esophagus and hence ‘spasm.’”
An esophageal motility study measures how well the esophagus moves food to the stomach using pressure sensors during swallowing.
Duration of Spasms
“In these studies, the duration of contractions or ‘spasms’ is important,” says Dr. Fleisher.
“For example, to meet the criteria for the entity ‘diffuse esophageal spasm,’ one is required to have contractions that last for greater than six seconds, are repetitive, and do not often progress down the esophagus in the normal way.
“Other important criteria include increased pressure in the esophagus.”
He continues: “Esophageal spasms can vary in duration. Clinically important contractions need to persist for more than six seconds.”
If pain in the esophageal area lasts only a second to a few seconds, it could be a spasm of a skeletal muscle.
When that happens, ask yourself if you did an upper body workout within the past few days.
As far as getting the correct diagnosis, Dr. Fleisher explains that an esophageal spasm is “often a clinical diagnosis, and a diagnosis of exclusion.
Endoscopy is a poor test for evaluation. X-ray study such as a barium swallow will provide better physiological information suggesting disordered contraction but are poor at associating symptoms with the observed abnormality.”
Dr. Fleisher was named a 2015-2018 “Top Doc” by Baltimore Magazine for gastroenterology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Anti-Seizure Drug Prophylactically after Head Trauma?

A neurosurgeon addresses taking anti-seizure drugs after head trauma even if there are no symptoms, just in case to prevent a seizure.
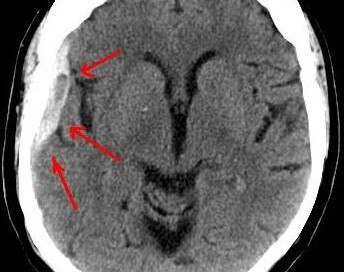
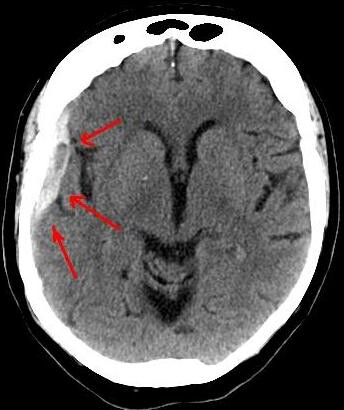
Keppra is an anti-seizure drug that may be given to a patient who has been diagnosed with a chronic subdural hematoma following a head trauma, such as hitting the head in a fall.
A chronic subdural hematoma is a slow brain bleed which may not start causing symptoms until two or three months after the trauma.
The drug is given when there are neurological symptoms from the head trauma, but not necessarily a seizure-type symptom.
After my mother underwent surgical draining of a chronic subdural hematoma, she was prescribed Keppra, because the risk of a seizure exists post-surgically for this condition, which affects mostly people over 65, though younger people can suffer from it.
Seizures are one of the more uncommon symptoms that arise from a chronic subdural hematoma prior to treatment.
More common symptoms are headaches, mental changes and weakness on one side of the body.
If you know that seizures (though not commonly) can result from a chronic subdural hematoma (that develops after head trauma), you then might wonder this:
Why not take an anti-seizure drug even if the CT scan is normal and the patient has no symptoms — just to play it safe?
After all, a normal CT scan doesn’t predict a future normal CT scan.
Remember, a chronic subdural hematoma may take up to 90 days to develop enough to start causing symptoms, which as mentioned, can include a seizure.
So why not be ready for a seizure by taking an anti-convulsant medication on a “just in case” basis?
Otherwise, the patient, unaware that a brain bleed is developing, might have a seizure from it while driving or walking down a flight of stairs.
To all of this, here is what Ivan Mikolaenko, MD, says:
“No prophylactic antiepileptic drugs are recommended in a patient with normal CT scan and no seizure following head injury!!!”
Dr. Mikolaenko is a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.

Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Masha Petrakova

How Soon after a Normal Head CT Can You Drive?
It’s a fair question: For how long should you avoid driving after hitting your head, even though the CT scan is normal and you have no symptoms?
You hit your head and that day, get a CT scan to see if there’s any sign of subdural hematoma. The CT scan is normal.
However, you also know that a normal CT scan the day of head trauma, and even 24 hours later, doesn’t guarantee you can’t develop a slow brain bleed (chronic subdural hematoma) over the next few months…causing disturbing neurological symptoms.
Some of the symptoms that a chronic subdural hematoma can cause are sudden and profound weakness of one or both legs or arms; a seizure; cognitive impairment; and a searing headache.
In fact, a symptom from chronic subdural hematoma can mimic that of stroke or transient ischemic attack. Imagine driving while a symptom (or two) suddenly strikes.
Could you control the car while your brain is bleeding?
You may not even KNOW you’re having a symptom, and thus, begin losing control of the car and not even know it!
This begs the question:
For how long should a person (particularly elderly) avoid driving even if their CT scan (and next-day follow-up CT scan) is normal, and they are sent home with no symptoms?
“It depends on severity of initial presentation,” says Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
“I usually recommend to take a rest and don’t drive until all symptoms are gone, and I usually recommend to repeat CT scan in 3-4 weeks after head injury in patients older than 60 years.
“After that, given normal exam and normal imaging, patient can go back to driving.”
In other words, no symptoms at initial presentation in ER, and with a normal CT scan, mean that the patient is free to drive.
However, the patient should never drive TO the ER after hitting their head, since at that point, no diagnosis has been made.
You should always have someone drive you to the ER even if you “feel fine.”
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Mortality of Chronic Subdural Hematoma Soon After Drainage?

A certain percentage of people will die soon after having their chronic subdural hematoma drained.
The drainage procedure takes only 15 to 20 minutes, yet within 30 days, five percent of patients will be dead.
A 5% Mortality Rate within 30 Days of Burr Hole Drainage of a Chronic Subdural Hematoma
Just prior to my mother undergoing the 15-20 minute drainage procedure for her chronic subdural hematoma, the neurosurgeon told me that the biggest risks were infection and recurrence.
He made no mention of a mortality rate for the noninvasive procedure.
However, I’ve read in several online neurosurgery journals that there’s a well-documented mortality rate in patients within 30 days of the burr hole drainage of their chronic subdural hematoma.
One study said a 5 percent mortality rate. Another said a 6 percent mortality rate out of the 157 patients investigated.
“Although most of cSDHs often appear innocuous, severe complications may occur,” says Ivan Mikolaenko, MD, a board certified neurologist with subspecialty certification in neurocritical care, Neurological Surgery, P.C., New York.
Dr. Mikolaenko says those include the following.
“- Devastating intracerebral hemorrhage due to rapid brain decompression leading to hyperemia (increased blood flow) immediately beneath the hematoma or at any other area of the brain which was shifted and compressed for many days before surgery.
“- Failure of the brain to re-expand, especially in patients with pre-surgery low subdural fluid collection pressure: These people very often will have re-accumulation of the subdural fluid.
“- Intractable seizure post-op with or without status epilepticus.
“- Longstanding cSDH with conversion to subdural empyema (collection of subdural pus).
“- Untreated severe pneumocephalus (collection of bubble of air in place of evacuated subdural collection).”
As frightening as this mortality information all sounds to anyone who’s been diagnosed with a cSDH, it’s very important to realize that the death rate is still relatively low.
If you’ve hit your head recently, or know someone who has, be on the very vigilant lookout for any new-onset suspicious symptoms.
This includes out-of-character change in mood, memory issues, weakness, change in gait pattern, apathy, sudden headaches, or anything that just doesn’t seem right with the individual.
A chronic subdural hematoma is a slow bleeding in the brain, beneath the dura mater, and may take up to 90 days to begin producing symptoms.
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Volodymyr Baleha
Chronic Subdural Hematoma Questions Answered by Doctor
Here is where you may find the answers to your symptom questions about chronic subdural hematoma—right from a neurosurgeon.
Here are three questions about chronic subdural hematoma symptoms answered by Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
How much time must pass (“incubation period” or “grace period”) after the head trauma before the patient can know he won’t develop a chronic subdural hematoma, that he’s in the clear?
Of course, let’s assume that the initial CT scans, that were taken soon after the incident, were normal, and the patient had no symptoms.
“There is no clearly defined maximum ‘incubation period,’ but I agree that if someone will repeat CT scan of his head after three months of head injury and study will be normal, most likely patient is ‘in the clear,’” says Dr. Mikolaenko.
“I usually recommend to repeat CT scan in 3-4 weeks after head injury in patients older than 60 years.
“Yes, seizure can occur actually at any time after brain injury; even smallest scar on the brain might become epileptogenic focus for the rest of the patient’s life.”
Percentage of people with normal CT scans after hitting head who eventually develop a chronic subdural hematoma?
Dr. Mikolaenko says, “CSDH generally occurs in elderly, with average age being 63 years old, and head trauma is identified in almost 50% of these patients whose initial CT head [scan] was normal.”
Is the presence or absence of neurological symptoms at the time of head injury (fall on head, getting hit in head) predictive of likelihood of a chronic subdural hematoma developing?
In other words, if a patient can’t remember what happened to him and can’t follow instructions right after the accident, is he more likely to develop a cSDH than if he displayed no neurological symptoms whatsoever (he was lucid)?
“Yes, many cSDHs probably start out as acute SDHs,” says Dr. Mikolaenko.
“More severe symptoms at presentation very often indicate more severe head injury with even negligible blood within the subdural space, not visible on imaging, but enough to evoke inflammatory response and trigger complex chain of events on molecular level leading to formation of cSDH.”
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Lucien Monfils
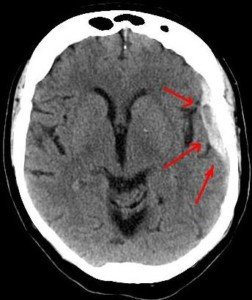
Chronic Subdural Hematoma: Follow-up CT Scan & MRI Timelines
![]()
Find out the ideal timelines for follow-up CT and MRI imaging for a chronic subdural hematoma.
A chronic subdural hematoma is typically diagnosed with a CT scan after a patient suffers a head trauma, or, after the patient begins displaying neurological symptoms weeks after the incident (which may have been forgotten due to its seeming triviality), and the image is ordered.
Suppose an elderly patient, who suffers a bang on the head, has a normal CT scan several hours, and then perhaps about 24 hours after that.
Now, how soon after this second imaging procedure should the patient have a follow-up, and should it be computed tomography or an MRI?
MRI is more sensitive and doesn’t deliver radiation: two reasons a savvy patient may request it over the CT scan.
Another point to consider is if the patient isn’t displaying any neurological symptoms that would suggest the presence of a chronic subdural hematoma.
Why have the procedure if there are no apparent symptoms of a chronic subdural hematoma?
Because maybe the patient wants to get ahead of the game; if a tiny, asymptomatic bleed is discovered, the patient may then decide to take it easy over the ensuing days (no driving, no activities that can cause a fall, etc.), and adhere to watchful waiting.
“If patient after head injury was hospitalized or spent around 24 hours in ER for observation, and had two CT scans at least six hours apart and they both were normal,” then the patient should not have a follow-up study as long as there were no neurological symptoms at the get-go, and no new-onset symptoms, explains Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
What if the patient had neurological symptoms at the get-go, and after one month, the symptoms have not resolved or improved?
Dr. Mikolaenko says that if the patient “is still symptomatic one month post-head injury, then I would order a brain MRI and make sure special hemosiderin sequences (GE or SWI) are done to detect microbleeds or small cSDH.”
He explains further: “Special hemosiderin sequences like gradient echo (GE) or susceptibility weighted imaging (SWI) are very sensitive for detecting even the smallest microbleeds or thinnest cSDH regardless how old was the bleed.”
MRI, then, not only is more sensitive, but doesn’t yield radiation exposure.
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Duet PandG

Can an Entire Glass of Beet Juice Go Undigested?

Just how much beet juice are you seeing in the toilet bowl?
Are you one of those individuals, like me, who swears that you’ve emptied into the toilet bowl just about all the beet juice that you drank?
I’d hate to think this is what actually happens, being that the only reason I drink this blazing crimson beverage is for the powerful antioxidants.
“The red color in the urine or stool is from a chemical called betanin, which accounts for less than 1% of the beet juice solids,” says Jonathan Zinberg, MD, chief of gastroenterology at South Nassau Communities Hospital, Oceanside, NY.
“This occurs in a small percent of the population (10 to 14%). The other nutrients are likely absorbed just as well in those people as in the rest of the population.”
Thank goodness! Now I know that I’m not passing most of the beet juice’s nutrients when I have a bowel movement.
Amazing Benefits of Beet Juice

Shutterstock/Africa Studio
• Helps lower your blood pressure.
• Low in calories; great part of a fat loss program.
• Strong source of antioxidants.
• Good source of potassium.
• Good source of minerals.
• Good for the liver.
Beverages that Can Be Spiced up with Beet Juice
Beet juice can add a vibrant color and earthy sweetness to a variety of beverages.
Here are some creative ways to incorporate beet juice into drinks:
1. Smoothies: Beet juice pairs well with fruits like apples, berries and oranges.
Blend beet juice with ingredients such as spinach, banana and almond milk for a nutritious and visually appealing smoothie.
2. Lemonades: Add a splash of beet juice to traditional lemonade for a colorful twist.
The beet juice will complement the tartness of the lemon and create a refreshing, eye-catching drink.
3. Mocktails: For a non-alcoholic option, mix beet juice with sparkling water, a squeeze of lime and a bit of honey or agave syrup for a refreshing mocktail.
4. Juice Blends: Combine beet juice with other vegetable or fruit juices, such as carrot, apple or ginger juice, to create a healthful and tasty juice blend.
5. Herbal Teas: Brew a mild herbal tea and mix in a small amount of beet juice.
This can add depth of flavor and a hint of sweetness to the tea.
6. Milkshakes: For a fun and colorful twist on milkshakes, blend beet juice with vanilla or chocolate ice cream and milk.
7. Sports Drinks: Beet juice is known for its potential performance-enhancing benefits.
Mix it with coconut water and a pinch of sea salt to create a natural sports drink.
 Jonathan Zinberg, MD
Jonathan Zinberg, MDLorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/bitt24

Can Burping Be the ONLY Symptom of Acid Reflux ?

You keep burping.
People around you keep noticing. Could this burping, without any other symptoms, be acid reflux or something else?
Burping As the Only Symptom of Acid Reflux
“Yes, there is increased salivation and swallowing in the body’s effort to clear the refluxate from the esophagus,” says Jonathan Zinberg, MD, chief of gastroenterology at South Nassau Communities Hospital, Oceanside, NY.
In acid reflux, the contents of the stomach make their way up into the esophagus and in some cases, even the throat and, believe it or not, the nose (this will cause a burning sensation).
Triggers of Acid Reflux
- This can be triggered by certain foods, particularly spicy.
- Heavy eating, particularly rushed, can also lead to it.
Dr. Zinberg further explains, “With each swallow, even subconsciously, air is swallowed as well (aerophagia), and this leads to burping of the accumulated air.
“Other causes of aerophagia include post-nasal dripping and anxiety.”
Preventing Burping from Acid Reflux
You’ll want to pay more attention to the kinds of foods that you eat. Acid reflux is commonly called heartburn because it causes a burning sensation in the chest.
But as Dr. Zinberg mentioned, it can also produce only one symptom: that of burping. And of course, belching in the presence of others is far more embarrassing than is feeling some heartburn.
So as far as the foods you should avoid or cut back on, they are as follows:
- Liquor, especially red wine
- Garlic, raw onions, black pepper
- Spicy foods
- Chocolate
- Caffeinated beverages
- Citrus fruits and citrus juices
- Peppermint
- Tomatoes
Another way to help prevent or reduce acid reflux is to avoid eating a lot of food at once.
In addition, if you tend to rush through your meals, this could lead to some burping. Slow down if you’re a fast eater.
Be mindful of whether or not you’re swallowing air with each spoonful, forkful or drink of your beverage of choice, even if it’s just water. Reducing acid reflux means reducing burping.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Nik Stock
Does Frequency of Heartburn Affect Risk of Esophageal Cancer?

Just how often must you have acid reflux from GERD (heartburn) to be at risk for esophageal cancer?
Esophageal cancer is one of the most frightening cancers to have, because its prognosis is poor in so many cases.
The disease is frequently diagnosed at an advanced stage because early symptoms can be vague or mistaken for less serious conditions.
Advanced stages of esophageal cancer often involve significant tumor growth or spread to other organs, making it harder to treat effectively.
19.2% – Number of people who are alive five years after a diagnosis of esophageal cancer, according to the National Cancer Institute Surveillance, Epidemiology and End Results Program.
As mentioned, this disease is typically discovered only after it has spread, making successful treatment very unlikely for the long-term.
There’s over 22,000 cases of new esophageal cancer diagnoses each year in the U.S., says the American Cancer Society.
People age 20 to 44 make up 2.3% of the cases, while those 65 to 74 make up 30.6%.
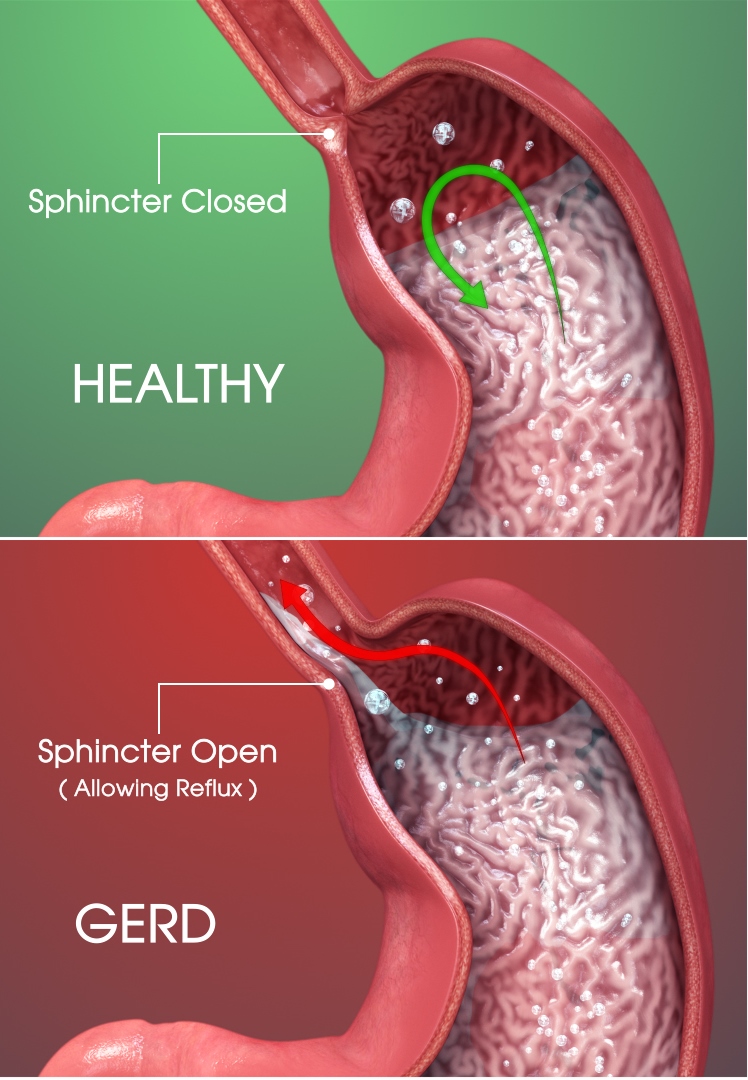
Heartburn, Acid Reflux
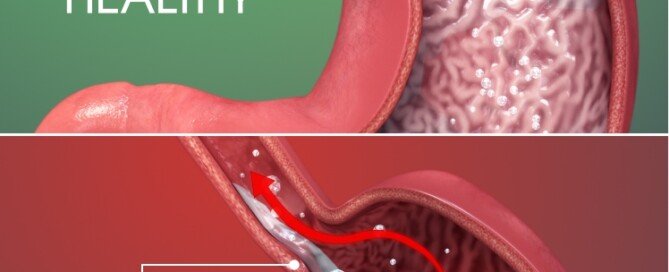
You may already know that GERD or chronic heartburn can lead to Barrett’s esophagus, which in turn is a risk factor for cancer of the esophagus.

Scientific Animations, Creative Commons/BY-SA/Attribution-ShareAlike 4.0 International
“Generally, we consider high risk for Barrett’s esophagus and subsequent esophageal cancer, those who have prolonged reflux symptoms requiring medication at least three times per week for more than five years, especially if older than 50,” explains Jonathan Zinberg, MD, chief of gastroenterology at South Nassau Communities Hospital, Oceanside, NY.
“However, new onset symptoms past the age of 50 should also be suspect and evaluated.
“Some patients with Barrett’s have few if any symptoms, so these are merely guidelines for higher suspicion.
“Those with a family history of esophageal cancer are also at a somewhat higher risk.”
If you have GERD, commonly known as acid reflux, you need to prevent Barrett’s esophagus.
Barrett’s esophagus is a condition where the lining of the esophagus changes due to chronic acid exposure, increasing the risk of esophageal cancer.
To control GERD, consider making dietary changes, such as avoiding spicy, fatty or acidic foods, and refrain from eating close to bedtime.
Elevating your chest (not just the head) while sleeping can also help reduce acid reflux by keeping stomach acids from traveling up the esophagus.
If Barrett’s esophagus is diagnosed, lifelong surveillance is necessary.
This involves regular endoscopic examinations to monitor the esophagus for any precancerous changes or abnormalities.
Don’t be afraid of an upper endoscopy. This procedure is a valuable diagnostic tool that allows doctors to examine the esophagus, stomach and the beginning of the small intestine.
An upper endoscopy is typically performed using a thin, flexible tube with a camera, called an endoscope, which is gently inserted through the mouth and into the digestive tract.
The procedure is done under sedation, so you won’t feel discomfort during the examination.
In fact, you may even completely fall asleep from the sedation during the procedure, and after what seems like only a minute or two, you’re told that the procedure is over.
If any abnormalities are found, the doctor can often take biopsies for further analysis or provide immediate treatment.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}