

Can a Blood Clot in the Leg Break off with Movement?

Learning you have a blood clot (DVT) in the leg is frightening.
And even more unsettling is the thought that movement can cause it to break off and travel to the lung and become a life-threatening pulmonary embolism.
If the broken-off portion of the clot is big enough, it can block both entryways for oxygen to the lungs, resulting in a quick death.
A person who’s been diagnosed with a DVT, or who believes they have one, may be afraid to be up and about walking.
Should movement be limited in someone diagnosed with a DVT?
If you’ve been diagnosed with a deep vein thrombosis, you might be thinking that you should remain as still as possible so that it doesn’t break off and travel to your lungs.
“No, most DVTs are fixed to the wall of the vein and it is highly unlikely to dislodge unless the vein is exposed to vigorous compression or unnatural force,” says Darren Klass, MD, clinical instructor of interventional radiology at the University of British Columbia and the Vancouver Coastal Health Association.
When these blood clots do dislodge, it’s usually something that happens spontaneously, with no apparent trigger.
This is why if you suspect a blood clot in a leg, you should immediately go to the nearest emergency room. Have someone drive you!
Treatment will begin immediately after diagnosis.
A DVT may cause redness, warmth, pain, cramping and/or swelling in a leg or behind the knee.
Immobility
Dr. Klass adds, “Conversely, not moving with a DVT may increase the risk of the clot getting larger due to the lack of blood flow from the legs.
“For this reason, pneumatic compression devices are often used during and/or after major surgery when a patient is not ambulant in order to stimulate venous flow in the legs.”
 Dr. Klass specializes in interventional oncology, aortic intervention, PVD, venous disease and venous access. He has been inducted into The Leading Physicians of the World, published by the International Association of HealthCare Professionals. Vancouver Coastal Health
Dr. Klass specializes in interventional oncology, aortic intervention, PVD, venous disease and venous access. He has been inducted into The Leading Physicians of the World, published by the International Association of HealthCare Professionals. Vancouver Coastal Health
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Casa nayafana

Top 4 Causes of Swollen Legs after Surgery

There are four main conditions that can cause legs to swell after surgery.
“There are a number of reasons for swollen legs post-operatively,” says Darren Klass, MD, clinical instructor of interventional radiology at the University of British Columbia and the Vancouver Coastal Health Association.
“The majority of the causes for this is fluid leaking into the soft tissues due to low protein in the blood, poor heart function, deep vein thrombosis, lack of mobility.”
Surgery that causes swollen legs need not involve the lower part of the body.
Coronary bypass surgery can leave both legs quite bloated.
DVT not the Leading Cause in Bilateral Swelling
“Unless the swelling is only on one side, the chance of this being a deep vein thrombosis is less than other causes,” says Dr. Klass.
“A deep vein thrombosis may not cause swelling of the leg initially and patients may be completely asymptomatic. It is only when the return of blood to the heart from the legs becomes compromised, do we see swelling from DVT.”
The swelling in the one leg may not be noticeable at first. But if the patient believes that the lower leg is looking just a little bit bigger than the other, they should point this out to their nurse and doctor.
If a DVT is suspected, a bedside ultrasound will be taken of the leg. It will immediately show if there is a blood clot.
If the result is negative, this is no reason to let your guard down. Do keep monitoring your legs, since a DVT may still develop.
Other Symptoms of DVT
Some hospitals will make sure that no matter what kind of surgery, the patient will postoperatively have on pneumatic compression devices for their liower legs.
These deliver intermittent compressing motions that help keep the blood from pooling.
To further help prevent a blood clot, some hospitals will mandate that all patients receive a daily injection of the blood thinner heparin.
Other signs of a deep vein thrombosis are reddish or purple or pale discoloration of the leg, tenderness, cramping or pain.
The pain may even persist even if you’re at rest or sitting. Pain can also occur in the pelvic area.
If both legs are swollen soon after surgery but feel fine and are not discolored, the patient should always be DVT-conscious.
Dr. Klass specializes in interventional oncology, aortic intervention, PVD, venous disease and venous access. He has been inducted into The Leading Physicians of the World, published by the International Association of HealthCare Professionals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com/ pressfoto
Can a Pulmonary Embolism Be Diagnosed without Imaging?
A doctor may strongly suspect a pulmonary embolism based on a patient’s circumstances, such as suddenly struggling to breathe the day after hip replacement surgery, or sudden chest pain.
Even if the patient has other classic symptoms of a pulmonary embolus such as coughing up blood-tinged sputum, a doctor in good faith cannot just order administration of a clot busting drug unless the diagnosis is confirmed with imaging.
“The use of medication to bust up clots carries with it a risk of bleeding elsewhere in the body, as the medication stops blood from clotting,” says Darren Klass, MD, clinical instructor of interventional radiology at the University of British Columbia and the Vancouver Coastal Health Association.
“The physician responsible for administering the medication knows this and will ask specific questions to the patient to ensure it is safe.
“The patient must be closely monitored after this medication has been administered and therefore requires hospital admission.”
What leads to a pulmonary embolism?
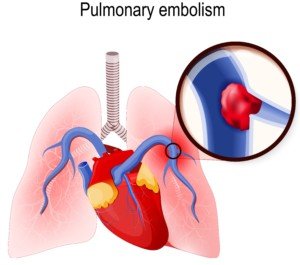
Shutterstock/Designua
A pulmonary embolism is a blood clot in a lung (sometimes both; there can be multiple) that originally developed in a lower-extremity vein (lower leg to hip).
Such a blood clot is called a deep vein thrombosis (DVT) and are considered an emergency situation because it can dislodge at any time — and head straight for the lungs.
So to prevent a pulmonary embolus, one must take measures to lower their risk of a DVT.
Major Risk Factors for a DVT
- Obesity
- Smoking
- Birth control pills
- HRT therapy
- Excessive sitting throughout the day
- Sitting immobile in cramped quarters for hours without a break
- Long airplane rides
- Recent joint replacement or abdominal surgery
- Excessive bed rest
- Pregnancy
- Older age
A DVT is easily diagnosed with an ultrasound. A pulmonary embolism is diagnosed with a CT scan.
PE symptoms in combination with a positive result of a specific blood test will raise strong suspicion of this blood clot, but are not enough for an official diagnosis.
“Aside from this, PE can only be confidently diagnosed using medical imaging such as a CT scan,” says Dr. Klass.
“The clinical signs of pulmonary embolus are non-specific and cannot be confidently made without imaging.”
Dr. Klass specializes in interventional oncology, aortic intervention, PVD, venous disease and venous access. He has been inducted into The Leading Physicians of the World, published by the International Association of HealthCare Professionals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Thousands of PVCs, Normal Echo: Get EP Testing

A cardiologist says that if you have thousands of PVCs but a normal echo, you should get an EP test for a possible arrhythmia.
If you have PVCs (premature ventricular contractions), you may have developed an understanding along the way that these “skipped heartbeats” are benign as long as your echocardiogram is normal.
“Just because the echo is normal, that doesn’t mean that the person does not have bad coronary artery disease or a PVC focus that is causing all the PVCs,” says Dr. Sameer Sayeed, MD, a cardiologist at ColumbiaDoctors of Somers, NY.
Coronary artery disease can cause these “skipped heartbeats,” and an echocardiogram cannot detect or evaluate plaque buildup in arteries.
Other tests can evaluate for the existence of heart disease or assess heart disease risk: coronary calcium scoring, and the CT angiogram.
“If there are many thousands of PVCs, the patient’s coronary arteries should also be evaluated,” says Dr. Sayeed.
“If they are normal, then EP testing should be performed to determine if there is a PVC focus and if it should be ablated.”
An EP test is an electrophysiological exam of the heart to see if there is a rhythm disorder.
It takes about three hours and is administered by a cardiac electrophysiologist.
A doctor threads thin catheters with electrodes through veins into the heart, records signals and may try to trigger arrhythmias.
This helps diagnose and guide treatments like ablation or pacemaker placement, usually under sedation.
“When there are excessive PVCs, the heart is at risk for an arrhythmia or weakening of the muscle [cardiomyopathy] due to the excessive stimulation by the excess PVCs,” says Dr. Sayeed.

Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Why a PVC Can Cause Coughing

A cardiologist offers a simple explanation for why PVCs can cause some people to cough.
PVC stands for premature ventricular contraction, and some people can’t help but cough after having one of these episodes.
The coughing is usually just a single or double, and all it takes is just one PVC to trigger this.
“You may cough due to the phenomenon of post-PVC beat where the heart has a stronger contraction after a PVC, and this can irritate the diaphragm or phrenic nerve and cause cough,” explains Dr. Sameer Sayeed, MD, a cardiologist at ColumbiaDoctors of Somers, NY.
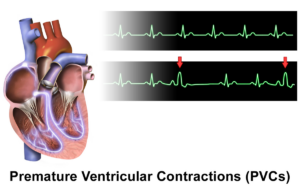
Source: BruceBlaus/CreativeCommons
The phrenic nerves (a pair) come down from the cervical area of the spinal cord and control breathing by innervating the diaphragm.
Both phrenic nerves pass very closely to the heart.
It’s also possible, though less likely than the explanation above, that the cough is triggered by sudden anxiety over feeling a “skipped heartbeat.”
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can an Ultrasound Miss a DVT (Deep Vein Thrombosis) ?

It’s very true that an ultrasound can actually miss a DVT, but other tests are more definitive.
Staci Stringer’s DVT was missed by an ultrasound.
In September 2010, she experienced a deep vein thrombosis and pulmonary embolism.
When the DVT developed, Stringer was on birth control, but she also had lupus anticoagulant syndrome and rheumatoid/psoriatic arthritis.
Ultrasound Misses DVT
“It started as a pain in my leg, and after a week I went to the ER and had an ultrasound; they said it was nothing,” says Stringer on her site.
“The following Monday I was admitted to the ER with a PE,” which had caused chest pain.
“After a week or so the PE cut off blood flow to a portion of my lung which caused a pulmonary infarction.”
Another way of saying this is a “heart attack in the lung,” in that oxygen was cut off by the blood clots to the lung tissue, permanently damaging it.
Symptom Detail
“I started to feel the symptoms of a DVT in my right calf,” says Stringer’s account.
“It was swollen, extremely painful, hard to walk. I ignored the symptoms because I figured it was just arthritis pain.”
She continues: “I spoke with my general practitioner after a week and she told me to go to the ER for an ultrasound.”
Ultrasound is a standard diagnostic tool for DVTs.
“The technician thought he saw something but sent me home. I started to get a fever; my calf became so stiff I couldn’t walk.
“I walked up two flights of stairs to my apartment and was so out of breath I was grasping for air for 10 minutes.
“Next day I walked up the stairs to my office and I was so out of breath I fainted. I was admitted to the ER. After the CT scan they found a pulmonary embolism.”
How does an ultrasound miss a DVT?

Scientific Animations, Creative Commons/BY-SA/Attribution-ShareAlike 4.0 International
“I regularly order a venous Doppler to rule out DVT,” says Reena Patel, MD, a board certified family medicine physician who treats patients at Garnet Health Urgent Care in NY.
“An ultrasound uses sound waves and compression [of the blood vessel wall] to see blood flow in the veins of an extremity and can find an obstruction.
“There is room for error. Specifically, human error can result in a false negative, so it’s important to see the patient as a whole.”
A probe is used and if it slides off the vessel wall, a false-negative finding can result.
“It’s important in my experience, if suspicion is high and Doppler is negative, to have a backup plan,” says Dr. Patel.
“I may order a D-dimer. This is a sensitive test and can be very helpful to back up your diagnosis and warrant further imaging.
“I consider their history, the current symptoms and calculate their risk using reliable scoring such as the Wells’ score [a numerical value derived from the patient’s answers to numerous questions].”
Additionally, if you believe an ultrasound has missed a DVT, you should ask about a color flow venous duplex scan.
This should be of the vessels close to your pelvis as well as extending down to the foot.
If the D-dimer blood test is positive, the protocol is to have the patient undergo a chest CT scan.
The younger the patient, the more likely that a positive D-dimer means a blood clot, since old age can cause a false-positive with the D-dimer.
What caused Stringer’s DVT?
“The doctors weren’t sure if it was my birth control, my arthritis flare that caused the DVT,” says Stringer, “but I later found out I have lupus anticoagulant syndrome. I’m on warfarin for life.”
 In addition to treating many chronic conditions, Dr. Patel treats urgent conditions that affect every part of the body. Instagram: That_dr_next_door
In addition to treating many chronic conditions, Dr. Patel treats urgent conditions that affect every part of the body. Instagram: That_dr_next_door
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/TANAPAT LEK.JIW

Mild Congestive Heart Failure’s Effect on Exercise

Mild congestive heart failure may not even be noticeable to the person who has it, even when they are exercising.
“Usually if the mild congestive heart failure comes on very gradually and it is only mild diastolic CHF, then it may not be noticeable or only noticeable with very rigorous exertion,” or activity that’s more than usual for the individual, says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
So if you’ve always gone out every morning to leisurely walk your dog for half a mile, and all along your diastolic heart function is getting a little worse such that it’s in the range of mild heart failure — you probably won’t be suddenly panting at the end of that half mile.
Diastolic CHF: The heart is stiff, not relaxing properly. It does not fill up with the right amount of blood to be pumped out.
Thus, less blood is pumped out, meaning less oxygen throughout the body.
“If it is more severe diastolic CHF, then it may be a more acute and rapid decline,” says Dr. Sayeed.
“If it is systolic CHF and the ejection fraction [pumping force] goes below 40 percent, then the symptoms may come on more rapidly and with minimal exertion like [walking] a block or two or one flight of stairs.”
Systolic CHF: decreased pumping function. The heart’s “squeeze” is not optimal.
Dr. Sayeed explains, “The fatigue is usually most noticeable with exertion, particularly stairs and inclines, and the patient may suddenly report not being able to go up stairs or a hill or do competitive sports, etc.
“Symptoms won’t be so apparent at rest or with things like golf or easy activities where it may go unnoticed.”
If you’ve been working out all along, it’s smart to keep a record of your key workloads, which may be measured in amount of resistance, distance, speed or time.
As we age, these values will gradually decrease, e.g., your fastest one-minute run on a treadmill may be 12 mph at age 50, but 11.5 mph at age 55. This is normal decline.
If a performance deficit, however, is suspiciously rapid with no explanation (such as recent injury), then this warrants a medical evaluation.
Congestive (chronic) heart failure can be one of numerous causes of an inexplicable deficit in aerobic stamina or strength.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Congestive Heart Failure Cause Only Edema?

Edema refers to fluid retention such as that in the lower legs that causes swelling, but can this be the ONLY symptom of congestive heart failure?
Can a person feel and function just fine otherwise, despite the puffy lower legs and ankles from the congestive heart failure’s edema?
Congestive heart failure can cause numerous symptoms, including the fluid retention of edema.
Sometimes, this backed-up fluid goes higher than knee level, affecting the upper legs and even the groin area.
“Congestive heart failure can just cause edema and no other symptoms if it is due to purely right [heart] sided failure,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“But this is rarer, as right sided failure is usually caused by left heart failure which would cause dyspnea.”
The “failure” refers to the heart’s right or left ventricles failing to perform efficiently. And dyspnea means shortness of breath.
In heart failure, the pumping action of this organ is either inadequate, and/or the heart’s chambers don’t refill with as much blood as they should prior to each beat.
The end result is an insufficient supply of oxygenated blood circulating throughout the body.
So what this all means is that many more times than not, a patient will have, in addition to edema from the congestive heart failure, a problem with shortness of breath or getting out of breath fairly easily.
For example, activities that historically did not leave the patient breathing hard, now leave him or her winded, such as walking up a flight of stairs, walking quickly on an inclined parking lot, doing housework or lightly playing with the grandkids in the backyard.
They will fatigue more quickly from day-to-day activities that had never tired them out before.
When the excess fluid is in the groin area, it can impose upon the bladder, reducing urine output. This fluid would be visible on a CT scan.
Other Symptoms of Heart Failure
In addition to edema and shortness of breath, CHF can cause nausea, appetite suppression, a cough with white or pinkish phlegm, and chest pain.
Consult with your cardiologist if you have any concerning symptoms including new-onset ankle or lower leg swelling in BOTH legs, which could signal congestive heart failure.
If you have new-onset swelling in only one leg, particularly the lower leg, this could be a deep vein thrombosis.
This needs immediate attention, as this blood clot could detach and very quickly travel to the lungs and be life threatening.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/futurewalk
Source: mayoclinic.com/health/heart-failure/DS00061

Fast Rotator Cuff Tendonitis Pain Treatment without Surgery

The procedure is minimally invasive, nonsurgical and provides immediate pain relief from rotator cuff tendonitis.
A minimally invasive procedure to treat tendonitis in the rotator cuff provides immediate symptom relief, according to a study.
For some patients, their rotator cuff can accumulate calcium residue and be resistant to physical therapy.
“Calcific tendinopathy often resolves on its own but can become chronic,” says Jessalynn Adam, MD, who specializes in primary care sports medicine with OrthoVirginia.
“Often, a combination of physical therapy and shoulder injection with/without percutaneous needle tenotomy is sufficient treatment.
“The U.S.-guided procedure is effective but is uncomfortable. Patients are often sore following the procedure for a couple of days as well. However, there are good results.
“A study demonstrated that at one year, patients who underwent needling had more improvement than simple cortisone injection alone.
“Surgery is uncommon for this condition and only indicated for patients with refractory symptoms for six months or more (about 10% of cases).”
Another study found that ultrasound-guided nonsurgical therapy significantly reduces pain from calcific tendonitis of the rotator cuff and restores lasting mobility after treatment.
The treatment resulted in a single and inexpensive approach that was effective, says the study’s author, Luca M. Sconfienza, MD.
In severe cases, patients may require shockwave treatment or open surgery to remove the calcium.
Open surgery requires a hospital stay and rehabilitation and, on rare occasions, may result in major complications, such as tendon rupture.
How the Procedure Is Done
For the 20-minute procedure, the shoulder is anesthetized and, with ultrasound guidance, a radiologist injects a saline solution into the rotator cuff to wash the area and break up the calcium.
A second needle is used to aspirate, or withdraw, the calcium residue. Recovery time is about an hour.
Complete absence of the pain, following only a single procedure, is not guaranteed, but may be well worth it for chronic sufferers.
Symptoms of Rotator Cuff Tendonitis
• Pain in the upper side of the arm when lifting the arm straight out at one’s side
• Same pain when reaching overhead, especially with straight arms.
• Same pain when slipping the arm through the sleeve of a coat or jacket.
 Dr. Adam specializes in the care of athletes and active individuals of all ages, offering prevention, diagnosis and treatment of sports and exercise injuries. Dr. Adam’s care focuses on muscle injuries and biomechanics.
Dr. Adam specializes in the care of athletes and active individuals of all ages, offering prevention, diagnosis and treatment of sports and exercise injuries. Dr. Adam’s care focuses on muscle injuries and biomechanics.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/xmee
Source: sciencedaily.com/releases/2009/06/090630074949.htm

Parkinson’s: What Cardio Exercise Intensity Works Best?

Find out what a study says about the best cardio intensity level for Parkinson’s patients.
Will those with Parkinson’s disease benefit more from low intensity cardio exercise or higher?
Researchers at the University of Maryland School of Medicine and the Baltimore VA Medical Center wanted to find out what would be a preferable exercise for those with this neurological disorder.
Study Results
The low intensity group experienced the greatest degree of consistent improvement in gait and mobility.
For the study, subjects with Parkinson’s disease walked on a treadmill and also did resistance and stretching exercise.
There were three groups:
1) 50-minute treadmill walk for low intensity, 2) 30-minute incline walk for high intensity, 3) resistance exercise for the legs.
All Parkinson’s groups exercised for three months, three times a week.
“These results show that exercise in people with Parkinson’s disease can make a difference in their function,” explains Lisa Shulman, MD, the lead study author, professor of neurology at the University of Maryland School of Medicine.
In the report she adds, “Exercise may, in fact, delay disability and help to preserve independence.”
People with Parkinson’s should strongly consider low intensity cardio workouts.
Walking on a Treadmill for Parkinson’s Disease
Based on this study, it appears that treadmill walking will produce the greatest benefits for ambulation, when compared to using other kinds of cardio equipment.
After all, to get from point A to point B, we usually walk rather than pedal or step upward.
Walking is the most natural form of human movement, so the treadmill is the obvious choice for improving ambulation.
As far as cardiovascular benefits, any cardio equipment will suffice.
Getting Started on a Treadmill
Those with Parkinson’s disease should begin slowly on the treadmill and work on avoiding the habit of continuous holding on, as this will reproduce a gait pattern similar to that of using a walker. The image below demonstrates this.

Continuous holding on can also lead to repetitive stress injuries in the hips, plus “mold” posture into an incorrect form.
As your balance improves, gradually increase speed.
Again, the key is starting out at a slow-enough speed rather than a speed that makes you feel too off-balance to let go.
When I was a personal trainer, I noted that whenever someone told me they feared falling off a treadmill unless they held on, they had the speed at least 3.5 mph and often had a high incline.
If you must start out at only 1.5 mph, or even just one mph, at zero incline, then do so.
Then from there, gradually increase your speed over time, but never too much that you feel that you’ll lose your balance.
Holding on momentarily for balance checks is encouraged, but again, do not get into the habit of CONTINUOUSLY holding on — and this assumes that you can already walk in day-to-day living without a walker or cane.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}