
Can Exercise Cause Soft Plaque to Rupture?
Just who should worry about soft plaque rupture every time they work out?
“We define plaque in two ways,” begins Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
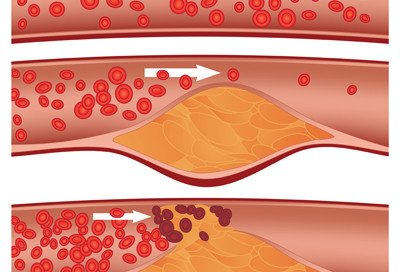
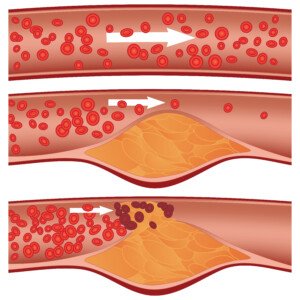
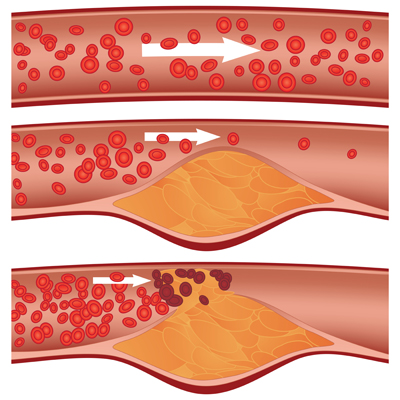
“Soft/unstable vs. stable/calcified plaque. Soft plaque is considered more unstable and is the plaque thought to rupture to cause myocardial infarctions [heart attacks], whereas stable plaque is more likely to cause predictable angina with exertion.”
Dr. Stevens-Cohen continues, “Soft plaque may rupture at any time. Normally, it doesn’t cause symptoms,” in that, despite the rupture, blood flow is not inhibited.
“We don’t know what causes soft plaque to suddenly rupture and trigger the sequence of events culminating in MI [heart attack].
Can exercise increase the odds of soft plaque rupturing?

Shutterstock/Liderina
“A sudden increase in demand of the heart, i.e., by increasing heart rate (strenuous exercise or any exercise in a patient not used to exercising) can change the workload of the heart and precipitate symptoms.”
If as an absolute rule, intense exercise (or any level exercise) increased the risk of soft plaque rupture, then people in gyms, on tennis courts, hiking trails, etc., would be dropping left and right from heart attacks.
But then again, bear in mind that people who regularly engage in gym workouts, tennis and basketball games, jogging, etc., in general have far better heart fitness and health than do sedentary people.
The problem is when a sedentary person, whose heart is NOT used to a hard workout, one day engages in a hard workout (shoveling snow, chopping wood, helping a friend move, hiking for the first time in years, etc.).
THIS is the person who’s at greater risk of suffering a soft plaque rupture that can result in a heart attack.
“Yes, most sudden MIs or what we call massive heart attacks that change the ECG (the true medical emergency where we want the vessel open in < 90 minutes), occur in the rupture of soft plaque,” says Dr. Stevens-Cohen.
“With the increase in demand caused by sudden exercise/excitement [in a deconditioned person], a not so stable plaque may rupture, exposing the inside of the plaque to the bloodstream and causing a thrombus to form.”
So if your body is already well-acquainted with intense exercise, you don’t need to worry as much about a soft plaque rupture as you perform your deadlifts, chin-ups to exhaustion, squat jumps or high intensity interval training.
It’s your paunchy, sedentary neighbor who’s out there hurriedly shoveling snow who’s at notable risk of that soft plaque rupture.
Though the cold air adds a burden to the heart, this individual is at risk of a soft plaque rupture even in warm weather should he decide one day to engage in strenuous exercise (i.e., a pickup basketball game with the neighborhood teenagers).
The degree of stable/calcified plaque that’s present in the coronary arteries is strongly correlated to the amount of soft plaque present, and is strongly correlated to likelihood of a cardiac event within three years of such a finding.
In other words, if a person at low risk for heart disease has a calcium score of zero, chances are pretty high that this person has very little, if any, soft plaque buildup.
The higher the calcium score, the greater the chances of having soft plaque buildup.
Exercise is great for the heart and helps prevent soft plaque buildup.
The problem is when a sedentary person, especially one with risk factors for heart disease and attack (e.g., high blood pressure, diabetes, abdominal obesity, overall excess body fat, smoking, standard American diet), takes on way too much exercise at once.

Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Diamond_Images

Survival of Untreated Mild Heart Attack

If you have a mild heart attack but no surgical treatment, how long will you survive?
“The short answer is we don’t know,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
“If we suspect a silent MI (based on ECG, echocardiogram or stress test results), patients are immediately targeted for secondary prevention and are placed on an aggressive regimen including cholesterol lowering medication, aspirin and usually anti-hypertensives.”
I’ve always wondered about this because a man I used to work with in an office one day was absent. I later learned he had a “mild heart attack.”
He was 47 and a few days later was back at work. He had been driving when he felt chest pain and drove himself to the ER.
He’d had no bypass surgery, no stent. The only difference was that he was bringing grapefruits to work and saying how his heart needed the “roughage” of the fruit.
So this begs the question:
If someone has a mild heart attack but no surgical treatment, how long can they be expected to live?
Seems to me that if nothing is done (either surgically or major lifestyle changes), a major heart attack will surely occur.
Dr. Stevens-Cohen explains, “It may have to do with the wording. Sometimes, the blood tests (positive troponins) can be positive, but when you perform an angiogram or a stress test, there is no damage, area of ischemia or significant blockage.”
Troponins are enzymes that damaged heart muscle release, so when someone has a heart attack, these proteins WILL be released and show as elevated in the blood test. Ischemia refers to oxygen supply being cut off.
But back to the “mild heart attack”…
“Some physicians may word this type of event as a mild heart attack (almost comparable to the phrase chemical pregnancy),” says Dr. Stevens-Cohen.
“We see a change in the blood levels but no evidence of pregnancy and then the patient gets their period.
“If we don’t see anything of significance on the angiogram or stress test, a physician may opt for medical management.
“I would assume that a statin and baby aspirin would be indicated and you observe the patient. But lifestyle changes should also be a part of that conversation.
“In order for a CABG [bypass surgery] to be successful, there must be an area on the native coronary vessel that makes for a good target (a good bypass target).
“With diffuse disease, sometimes, there is no target to drop the bypass graft, and evidence shows us these grafts fail.
“Surgeons look at cath images to decide on targets, and if they don’t see a good one, they usually leave the vessel alone.”
One of the greatest things you can do to avoid a major and mild heart attack is to eliminate processed foods. Think this is impossible?
Processed foods are an invention of modern man. What do you think people were eating before canning factories and food manufacturing plants were invented?
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can a Troponin Level Be Normal After a Heart Attack?

A myocardial infarction is a heart attack. Troponins “leak” from damaged heart tissue and make their way to the bloodstream.
Normally in the absence of a heart attack the levels are very low. A heart attack will substantially spike the levels.
But can there be an exception to this rule?
“No. The definition of a myocardial infarction is myocardial/muscle damage, and that is defined by the presence of troponins in blood,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
If someone has chest pain and an abnormal ECG, but negative troponins, Dr. Stevens-Cohen says that the diagnosis would be unstable angina.
“The management is the same. However, the definition of infarction implies muscle necrosis [death] and we measure that by troponins and CPK levels.”
CPK is an enzyme found in the heart. “The levels usually rise within six hours of presentation and can remain elevated for 1-2 weeks following an event.”
If you go to the emergency room complaining of chest pain or “shortness of breath,” a doctor will order a test to check the level of troponins.
The doctor wants to rule out (or in) a heart attack as quickly as possible, and in fact, the results of this highly sensitive blood test will come back amazingly fast.
However, one test is not enough. If you had a heart attack, that initial blood draw — if done soon enough after the cardiac event–won’t necessarily show an elevation into the heart attack range.
Remember, it takes several hours for the levels to rise.
This is why at least four hours after the first test the doctor will want to have another blood draw taken.
If the patient indeed suffered a heart attack, then for sure, several hours later (it may be four, five or six, depending on the ordering-physician), the troponin level will be elevated into the definitive range for a myocardial infarction.
So maybe five minutes after a heart attack the troponin level is normal, but it won’t be several hours later — it will clearly be elevated enough to show heart muscle damage.
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Robert Kneschke

Is Intense Exercise Possible with Clogged Arteries?

If you’ve been diagnosed with heart disease, does this mean that strenuous exercise is off-limits?
Is intense exercise even POSSIBLE with blocked arteries?
First of all, let’s define strenuous exercise. Some people think this is running 10 miles nonstop.
Others see it as deadlifting twice your body weight for five repetitions. There are multiple ways to define “strenuous exercise.”
As a fitness expert, I’ll define it as brief bursts of very intense activity. Thus, deadlifting for an 8-12 rep max, with only one minute of rest in between sets, is quite strenuous.
Dashing up a hill for 15 seconds five times with a three minute slow-walking rest in between each dash is a strenuous workout.
Heavy kettlebell swings that leave you breathing too hard at the end to complete sentences is strenuous exercise.
Can a person who’s been diagnosed with heart disease carry out any of these types of strenuous or very intense exercises?
“This largely depends on how well the coronary artery disease is being managed and other complications associated with CAD,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
CAD stands for coronary artery disease.
Dr. Stevens-Cohen continues, “Important things to note: Is the patient fully revascularized? Does the patient have normal left ventricular systolic function?
If the answer to both of these questions is yes, I would expect the patient to perform strenuous activity with no specific limitations.”
Revascularization refers to a bypass surgery. The heart’s left ventricle pumps or “squeezes” blood into the aorta great blood vessel to be distributed throughout the body. The strength of this pump is referred to as systolic function.
If the contraction to pump out this blood is weak, then there won’t be adequate blood supply throughout the body. So imagine the burden that intense exercise will place on a heart with weak ventricular systolic function.
Though this won’t necessarily damage the heart, the patient simply won’t have enough circulating oxygen to perform intense workouts.
Dr. Stevens-Cohen continues, “Not uncommonly however, we are unable to fully revascularize patients. Sometimes we cannot stent arteries due to vessel size or diffuse nature of coronary artery disease. There are vessels that are not amenable to stenting nor bypass.
“In these situations, we try and optimize with aggressive medical therapy. However, patients may experience angina or anginal equivalents with strenuous activity.”
Angina refers to chest pain. Shortness of breath may also result, though shortness is what will happen even when the fittest person performs strenuous exercise (that which results in considerable fatigue and heavy breathing soon after commencement).
However, the shortness of breath in a person with heart disease may occur during the warmup, making intense levels of exercise impossible.
“If there is significant pump damage (decreased systolic function) following a large infarction [heart attack] or diffuse coronary disease, patients may also be limited by symptoms and unable to engage in strenuous activity,” says Dr. Stevens-Cohen.
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Interpass

Unexplained Jump in Triglyceride Levels in Healthy Adult

Find out a possible explanation for why your triglyceride level has jumped from last time you had it taken.
You awaken at 7 a.m., knowing that at 10 a.m. you’ll be going to the medical clinic to get your blood drawn for a lipid panel.
You drink nothing, no water, not even coffee. That’s because along with the blood draw for the lipid panel, you’re also getting blood drawn for the fasting glucose reading.
The results show a marked jump in your triglyceride level compared to last time.
What on earth? You haven’t changed your eating habits; you still exercise; have not gained weight.
Though menopausal transition can cause a spike in triglyceride levels, what if this happens but you’re nowhere near menopause or you’re a man?
“Prolonged or chronic dehydration can cause cell walls to thicken and increase production of cholesterol, making the numbers falsely elevated,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
“Many physicians counsel of fasting but do not remind patients to stay well-hydrated.”
So there’s a pretty good chance that your triglyceride jump is due to the dehydration that preceded it.
Think about that: No water for three hours since awakening; no water during the eight hours you slept; no water for three hours preceding bedtime. That’s 14 hours without fluids.
• What if you’re well-hydrated at bedtime, but then drink no water between awakening next morning and your lipid panel draw several hours later?
• How much of an elevation in triglycerides might this cause?
“I don’t think we have an actual answer to that,” says Dr. Stevens-Cohen. But she does say this:
“I do not believe that fasting the day of the test would cause a significant increase in triglyceride levels.
“Most labs suggest patients remain well-hydrated, but they do not define how long it would take to cause a significant increase in triglyceride levels.”
Having a repeat test a few weeks later would be a good idea if you still haven’t figured out why there was a jump.
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sukiyaki

Ovarian Cancer vs. IBS Symptoms Explained by Doctor

Here’s what a cancer-gyn doctor says about ovarian cancer vs. IBS symptoms.
There are many articles or forum postings online with titles like “ovarian cancer vs. IBS” or “Is it IBS or ovarian cancer.”
I decided to get information straight from a gynecological oncologist: a physician who specializes in cancer of the female reproductive system.
Justin Chura, MD, is a gynecological oncologist in Philadelphia, PA.
Dr. Chura refers to a report by Goff et al. that appeared in JAMA 291(22): 2705-12, 2004.
The report consists of two tables that show a comparison between the symptoms of ovarian cancer and non-OC-related symptoms, as well as IBS.
“The first [table] shows that ovarian cancer patients were more likely to have pelvic pain than IBS patients,” says Dr. Chura.
“They were also more likely to have bloating, increased abdominal size and urinary symptoms compared to IBS patients.
“Additionally, ovarian cancer patients were more likely to have a combination of 3-4 symptoms compared to the IBS patients.”
The Vagueness of Ovarian Cancer Symptoms

Shutterstock/fizkes
“The issue is that the symptoms for ovarian cancer are what we call non-specific,” says Dr. Chura.
“Patients with uterine cancer have a very clear symptom which is bleeding after menopause.
“Thus, these patients get diagnosed at an early stage because they seek medical care.
“For ovarian cancer, there is no symptom that identifies the disease at an early stage.
“Furthermore, there is no screening to identify the disease at an early stage.”
IBS Symptoms
Some IBS patients report a lot of pain, which can be in the leg and back (OC can also cause these symptoms), and they can get a lot of diarrhea and constipation—including alternating.
The overlap between the symptoms of IBS and ovarian cancer have the potential to be markedly similar — and on paper, outright identical.
So what should you do?
First of all, get this in your head: IBS is a diagnosis of exclusion! A doctor shouldn’t be sure that you have IBS unless all other causes of your symptoms have been diagnostically ruled out.
“You could have IBS” is told to patients quite often, and I myself even heard this from the GI nurse who was prepping me for my colonoscopy to find out why I was having strange diarrhea and altered BMs.
My condition turned out to be microscopic colitis—but the diagnosis was verified under a microscope. However, IBS remained a differential diagnosis up till that point.
There is no diagnostic test for IBS.
If you’re being told you have IBS, you’d better be sure that all serious (and benign) differentials have been diagnostically ruled out.
Unfortunately, the only diagnostic test for ovarian cancer is a biopsy of the “mass” on/in the ovary. Even an internal ultrasound cannot diagnose.
If you’re having troubling symptoms or “vague,” “non-specific” symptoms that, on paper, point equally to IBS and ovarian cancer, see a gynecologist first. Ask, “Are my ovaries okay?” Then take it from there.
 Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Angina Be Ruled out with a CT Scan?

Is it possible for a CT scan to rule out angina?
Angina is chest pain caused by blockages in the coronary arteries: coronary heart disease.
It may also be accompanied by shortness of breath and/or nausea.
A CT (“cat”) scan uses radiation to create an image of the heart, so can this device detect angina?
“No. Angina is a symptom that must be provoked by a stressor or stress test,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
“A coronary CT is a non-provocative test. You can see soft plaque and calcified plaque and measure the degree of obstruction.
“However, you cannot tell if a patient’s symptoms are related to that obstruction.
“This is the limitation of coronary CT and why provocative testing with stress tests is the preferred method for diagnosing angina.”
A stress test is often done with a treadmill; the patient walks slowly while the angle of the tread surface is gradually increased to simulate a hill.
Another way is with a stationary bike. A third way, for people who are unable to use their legs such as those with knee problems, is with a drug that makes the heart think that it’s exercising.
As for the CT scan and angina detection — think of it this way: Can an X-ray show joint pain? No. It can show arthritis, but it can’t show the symptom of pain.
Angina is a symptom — chest pain and/or shortness of breath are the two most common — that’s caused by inadequate blood supply through the heart — due to excessive plaque buildup that narrows the inner diameter of the arteries.
Risk Factors for Clogged Arteries — no particular order
- Smoking
- Obesity
- Absence of structured exercise regimen
- Excessive daily sitting
- Untreated sleep apnea
- Junk food diet, or diet of mostly processed goods, even if you’re thin
- Cocaine use
- Advancing age
- Family history of early-onset coronary artery disease
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/airdone

Can You Accidentally Shave Off Melanoma?

Maybe you’ve read a few things about “picking off” a melanoma, but what about shaving it off—by accident?
Are you wondering if melanoma can be picked off?
“It is moles and nevus or seborrheic keratosis which get picked off while shaving or by fingernails,” says Rajiv V. Datta, MD, Medical Director, The Gertrude & Louis Feil Cancer Center; Chair, Department of Surgery, South Nassau Hospital. Dr. Datta performs surgeries on melanoma.
“To remove a melanoma, it has to be deliberate, not accidental. You cannot accidentally shave off melanoma, as it is deep,” he further explains.
“Even if you dig it out with a fingernail, the site does not heal, as it is a melanoma.”
A nevus is another name for a mole (pronounced knee-vus). A seborrheic keratosis is a harmless skin barnacle that can look like a mole, and at times, even resemble melanoma.
A seborrheic keratosis can suddenly start changing in color as well as color distribution, mimicking a malignancy.
Do not pick these off, even though they often look “pickable.” It’s best to have a dermatologist suspect any suspicious lesions.
But as for the idea that melanoma can accidentally be shaved off, Dr. Datta adds:
“Melanocytes are normal cells at the basal layer of the epidermis. These are single cells and can sometime get shaved off.
“Melanoma cells are cancerous which means that they have gone through their cell wall and invaded the surrounding cells; they are also proliferative, meaning that there are a lot of these cells.
“A combination of these makes it difficult to accidentally shave it off.”
 Dr. Datta is an international leader in surgical oncology. Under the direction of Dr. Datta, South Nassau uses leading-edge surgical technologies to remove skin cancer.
Dr. Datta is an international leader in surgical oncology. Under the direction of Dr. Datta, South Nassau uses leading-edge surgical technologies to remove skin cancer.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Oleksandr Nagaiets

Schiff’s MegaRed Krill Oil Capsules Contain Sorbitol: Not Natural

If you’re eager to buy Schiff’s “MegaRed” krill oil capsules, you may want to know that they contain sorbitol—a synthetic version.
When I first saw the TV commercials for Schiff’s MegaRed krill oil capsules, I was very excited that there seemed to be, finally, a high quality omega-3 capsule, since I could not find any at Whole Foods.
I could not find them at regular grocery stores, either, so I had to order them online.
I couldn’t find information about ingredients online, but I figured, what could possibly be in these krill oil capsules that’s bad?
I know that some supplements contain soy, but I banked that Schiff’s MegaRed would not contain soy. And the product doesn’t.
However, doggone it, this product contains sorbitol.
- My question to Schiff: Is this really necessary? SORBITOL?
- Is this an essential ingredient that without it, these krill pills would be useless?
Sorbitol, a sugar alcohol commonly used as a low-calorie sweetener, has been linked to several health issues.
One major concern is its gastrointestinal effects. Sorbitol can cause digestive distress, including bloating, gas and diarrhea, especially when consumed in large amounts.
This occurs because sorbitol is poorly absorbed in the small intestine and fermented by bacteria in the large intestine (Gibson et al., 2007).
Furthermore, sorbitol has a known laxative effect, which can lead to diarrhea if intake exceeds recommended levels.
This property is utilized in some over-the-counter laxatives (Tucker, 1993).
Additionally, despite having a lower glycemic index than regular sugar, sorbitol can still affect blood glucose levels, making it a concern for individuals with diabetes.
It is metabolized more slowly than glucose but can still contribute to overall blood sugar levels (Mann & Cummings, 2004).
Why is this chemical in the MegaRed product?
Now, I don’t know if the amount of this chemical in Schiff’s MegaRed constitutes the same amount that has been linked to a variety of adverse side effects, but what I DO know is this:
1) If something is truly safe, long-term use should not be associated with adverse side effects.
2) Even though I’m not a chemist, I can’t for the life of me imagine why Schiff feels it’s necessary to include this synthetic substance in its MegaRed product.
3) There’s enough seemingly legitimate information on synthetic sorbitol to make me NOT want to buy another bottle of Schiff’s MegaRed.
I’ll just make a point of eating more fish and continuing to take my omega-3 fish oil capsules.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
The Next Step if Your Breast Lump Isn’t on a Mammogram?



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}