
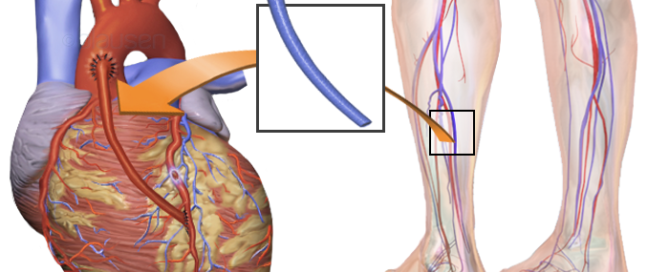
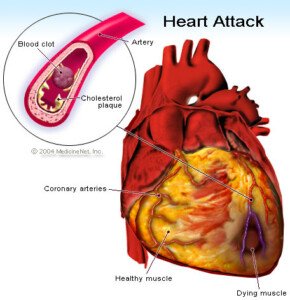
Coronary Bypass Surgery Post-op Complications that Seem Scary
If a loved-one has coronary bypass surgery, you as the visitor may become aware of a lot of interesting things that occur post-op.
Some of these will be considered “complications,” and they may seem very alarming, when in fact, they’re not as bad as they seem.
Atrial Fibrillation
The first complication that my mother had, while in the ICU after coronary bypass surgery, was “A-fib.”
You, as the visitor, will become aware of this when the heart rate monitor starts giving off a warning beep.
The monitor should be silent otherwise, so the sudden beeping will get your attention and be scary.
Staff will rush into the room and may awaken the patient if the patient is asleep during this event.
The first time my mother went A-fib, staff cleared her gown from her chest and attached monitors. This indeed looks frightening to the onlooking family member.
You may hear a nurse contacting a doctor by phone, describing the event and asking for directives.
You may see an EKG report being churned out of a computer and staff examining it.
And you will see, on the heart rate monitor, the heart rate continuously bouncing all over the place in the high range.
You will hear the word “A-fib” more than once being spoken. You may also remember that the heart surgeon told you, pre-op, that one possible complication of coronary bypass surgery is atrial fibrillation.
And you will remember, as I did, that the surgeon said it could easily be controlled, and that the more serious complication is ventricular fibrillation (V-fib).
Nevertheless, witnessing my mother’s first A-fib was nerve racking. So was the second one.
But each subsequent one was less alarming; you will notice that staff increasingly acts more casually, and that no doctors are present: a good sign.
You’ll learn that drugs control the situation, and that sometimes, the patient will spontaneously “pop out” of A-fib and the heart rate will return to normal.
If you witness several A-fibs, you’ll become very sensitized to the heart rate monitor’s distinctive beeping.
So that when you hear the monitors of other patients start beeping, you may have a conditioned response of anxiety and your own racing heart. Over time you’ll become desensitized to the beeping.
Kidney Function
Coronary bypass surgery may affect kidney function. A kidney doctor was called in to see my mother and explained she had mild kidney failure, and that they’d be just “watching it for now.”
Coronary bypass surgery causes the kidneys to be shorted of blood, and hence, they may “fail.”
The “failure” may only be mild, and is measured by a daily creatinine test. The doctor will be on top of this to see if the number gets above a certain value.
In the meantime, treatment will include fluid restriction.
The worst case scenario impression that I got was that if the kidneys didn’t “bounce back,” my mother would need dialysis. No mention of possible kidney transplant was ever made.
Mental State
The coronary bypass patient (or other type of surgery) may be delirious or confused even several days out from surgery; a definite alteration in normal mental status.

Shutterstock/Volodymyr Baleha
My mother thought I was her other daughter, for instance. Assume that off-the-wall comments, oddball questions and bizarre observations are the results of lingering anesthesia and/or the effects of powerful painkillers.
Chest Pain
The coronary bypass patient may complain of agonizing pain, particularly in the chest.
Don’t assume the patient is having a heart attack. Instead, remind yourself that the patient was very recently cut open in the chest.

Opening the chest. Shutterstock/sfam_photo
Complaints of severe pain may also center around the belly – where tubes will be inserted.
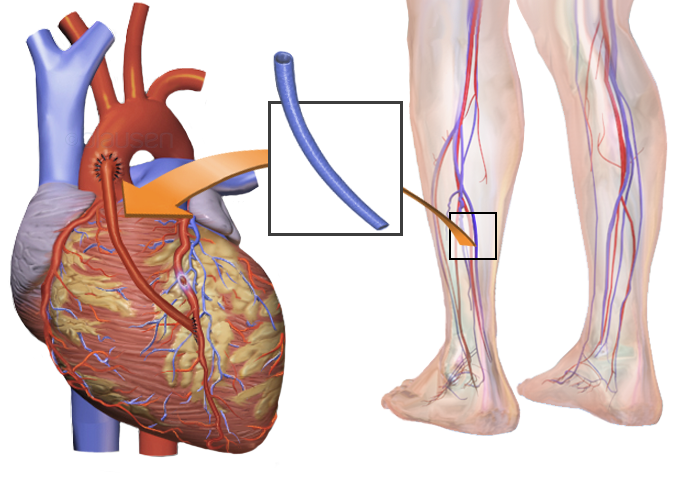
Very Swollen Legs
The coronary bypass patient will have significant visible swelling and bruising, especially in the legs if veins were harvested from the legs for the coronary artery grafting. This isn’t pretty, but it’s normal.
The coronary bypass patient will have fluid in the lungs; this is normal and is called pulmonary edema.
Fluid in the lining of the lungs, called pleural effusion, is also normal.
Drugs called diuretics treat this post-op condition.
Coronary bypass surgery is very frightening, but extremely lifesaving.
Enough visits to the coronary bypass patient and you’ll become acquainted with different kinds of beeping sounds that hospital equipment makes.
You may then develop a conditioned response of anxiety every time you hear things in daily life beeping, like your car when the seatbelt isn’t put on.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Blausen Medical Communications, Inc.

Can Stress Test Miss Severely Blocked Coronary Arteries?

If your stress test was normal, does this mean you can’t possibly have severely blocked coronary arteries?
How much faith should you put in the cardiac stress test?
“A stress echocardiogram or a nuclear stress test are each about 90 percent accurate in correctly identifying a severe coronary blockage, i.e., at least one of the coronary arteries has a narrowing greater than 70 percent).,” explains Dr. Larry Santora, MD, a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
“However about 10 percent of the time it will miss the blockage, and the stress test will be ‘falsely negative’,” explains Dr. Santora.
“These false negative stress tests are more common in women.
“It is more common to have a false negative if the blockage is in the circumflex artery which, on the back side of the heart, is more likely to be missed since it tends to be a smaller artery, and rarely, even if all three arteries are equally blocked (called ‘balanced ischemia’).”
The possibility of false negatives got me wondering, then, about someone with a high coronary calcium score who has a normal stress test.
They may worry that they might be in that 10 percent in which the test results are not accurate.
Dr. Santora explains, “There is no test in medicine that is 100 percent accurate; not a mammogram or colonoscopy, etc.
“If you have a high coronary calcium score and you are asymptomatic (no chest pain), and your stress test is normal, the probability of a severe blockage (meaning a narrowing more than 70 percent in one of the major coronaries) at that time is very, very low.
“If the patient had symptoms, even if the stress test is normal, then the chance of a severe blockage is perhaps 25 percent, and another test is needed, maybe a CT angiogram.”
The CTA will reveal amount of soft plaque versus hard (stabilized) plaque.
Soft plaque can rupture and block an artery.
Shutterstock/OSweetNature
“Anyway, it is the CAC that tells you if you need an aggressive approach to lower cholesterol and other risk factors,” says Dr. Santora.
So if you had a high coronary calcium score and normal stress test, this does not excuse you from taking aggressive measures to improve the state of your coronary arteries.
“The high coronary calcium score tells you that you must take aggressive risk reduction measures,” continues Dr. Santora.
“You cannot put full faith in a stress test. But some 90 percent blockages in the more distal ends (towards the end of the artery) can be treated without surgery or a stent, with risk modification.
“In these there can be plaque stabilization or some reversal, and the development of collaterals; that is, new arteries grow from a normal coronary over to the artery that is blocked.
“This can be promoted by exercise and external counterpulsation.”
If one’s coronary calcium score is deemed too high to allow a CTA image to be read (usually over 800), then Dr. Santora says, “You can still feel comfortable if you have no symptoms and a normal stress test, with vigorous risk modification.”
Modification would mean exercise, change in diet (e.g., severe restriction of refined carbohydrates and sugars, as well as saturated and trans fats), supplements and perhaps a pharmaceutical agent.
If the stress test is not clear, and you have a very high CAC, “then do an invasive cardiac catheterization and coronary angiogram,” says Dr. Santora.

Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Djohan Shahrin
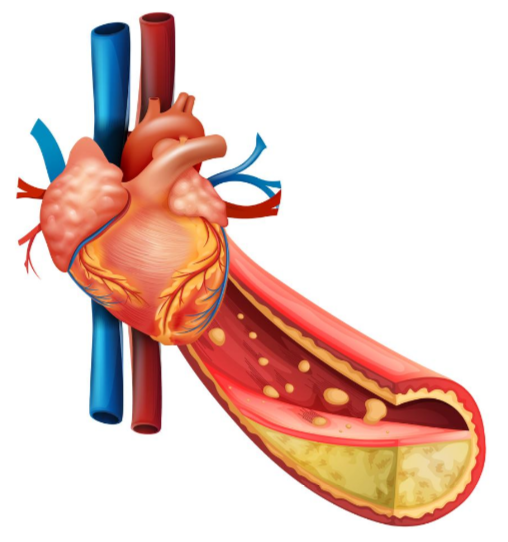
How to Make Diet Reverse Soft Plaque Buildup in Your Heart
There IS a way to make diet reverse the sludge plaque buildup in your heart’s arteries.
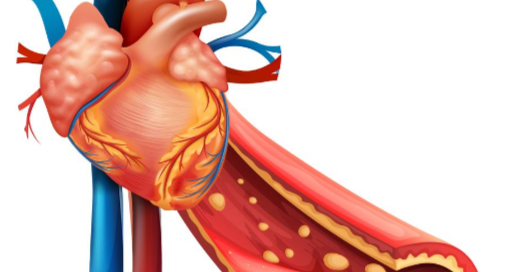
This dietary approach is not complicated. Coronary arteries are prone to getting clogged.
“Soft plaque can certainly be reversed, and so can some of the smaller areas of calcium,” says Dr. Larry Santora, MD, a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
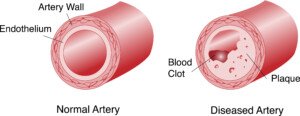
There are two kinds of plaque buildup in coronary arteries: soft and hard.
The soft plaque is the dangerous kind that can rupture and cause a heart attack (a fragment of this soft plaque breaks away from its base and travels through the coronary artery, blocking blood flow)
When someone has harmful levels of soft plaque, the goal is to stabilize this soft plaque.
Dr. Santora explains, “This means the plaque becomes more adherent to the inner vessel wall, and the cap on the plaque becomes stable and less likely to rupture.
“This occurs as soon as diet and medications are instituted, even before the cholesterol levels change.”
The diet for reversing coronary soft plaque is not a temporary diet; it is a permanent diet.
Dr. Santora says, “If you eat well 90 percent of the time, that is a reasonable way to go. So as a rule of thumb, all high glycemic foods like white bread, white rice, can be eaten, but only 10 percent of the time.”
The glycemic value of a food is a numerical measurement of how quickly its carbohydrates (sugars) are absorbed into the bloodstream after being eaten.
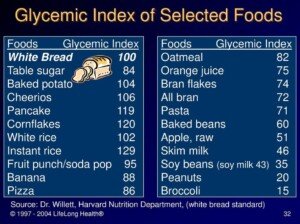
White sugars and simple, processed carbohydrates like white flour impose a terrible burden on the coronary arteries if eaten too often.
This means the occasional Boston cream pie is permissible, but knock out the white rice if you eat rice often; eat wild, basmati or brown rice instead.
Do you eat cereal every morning or most mornings?
It should be whole grain with no sugars added, and this includes high fructose corn syrup.
White flour is a ubiquitous food ingredient. Read ingredients lists. “Sugar” also shows up everywhere, including salad dressings and soups. Every “little bit” adds up.
What about whole eggs? Will whole eggs disrupt one’s dietary plan of reversing soft plaque?

Freepik.com
“As far as eggs go, they are now considered health foods; eating one or two per day, if not fried, are healthy since the cholesterol in eggs is not converted to cholesterol in the bloodstream,” says Dr. Santora.
What about going by the USDA Food Pyramid?
The food pyramid is ambiguous in that it names only food groups. At the bottom of the food pyramid are breads, for instance.
This does not mean make a staple out of a highly processed bread product like Wonder bread, bagels, English muffins or pancakes.
In fact, just about all commercial breads are full of synthetic chemicals; many contain high glycemic carbohydrates like molasses, corn syrup and even sugar.
Even breads at so-called health food stores may contain these heart-unhealthy items. Read ingredients lists.
The food pyramid doesn’t differentiate between carbohydrate sources and does not show information on “bad” fats.
A pancake mix labeled as “whole wheat” may still contain partially hydrogenated oil, which is a very bad fat: a trans fat.
So as far as the food pyramid, Dr. Santora explains, “The food pyramid is fine as long as the carbs are the good low glycemic type, and the fats are the good fats like monosaturated fats, and no trans fats. Simply avoid cookies, crackers and chips.”
A “little bit” (of a bad thing) can indeed hurt, because “a little bit” often morphs over time to a lot of “little bits.” Remember the 90 percent rule.
In order for diet to halt soft plaque progression, or even reverse soft plaque levels, you must not adopt an “a little bit won’t hurt” mindset.
Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Explode

How to Lower Your Coronary Calcium Score

Yes, it’s possible to actually lower your calcium score–the number that’s calculated from a CT scan of your heart’s coronary calcified plaque.
You may have been led to believe that coronary calcium score cannot be lowered; that the coronary calcium score progression can only be slowed down, or at best, halted.
But according to cardiologist Larry Santora, MD, you can, indeed, lower your calcium score.
“Yes, you can reverse the plaque,” says Dr. Santora,a cardiologist with Orange County Heart Institute and Research Center, and author of “OC Cure for Heart Disease.”
To achieve this, it’s through commitment to:
- A “clean” diet
- Exercising daily
- A statin drug
- Certain supplements
Sounds simple, right?
Well, it’s not as straightforward as you may think.
The statin part of lowering calcium score is as simple as taking it as prescribed.
Same with the supplements that are known to potentially lower calcium score and benefit heart health.
The confusion is with the diet and exercise part.
I can’t begin to tell you how many people whom I’ve encountered — including clients when I was a personal trainer — who truly believed they had a “healthy diet” — but just the opposite was true.
A perfect example of this is my mother. She was floored upon being told she needed emergency quintuple bypass surgery.
“How could this have happened to me?” She kept asking.
“I’ve always ate a healthy diet,” she’d say. “I’ve been on the Mediterranean diet! I’ve always been active!”
My mother has never had a coronary calcium score test; she had a catheter angiogram.
I can assume that had she had a calcium score test, the result would have been a very high number.
Re-evaluate your understanding.
Do YOU think you’re on the Mediterranean diet because you cook your white rice with olive oil, or because you dip potato chips in yogurt, or because you eat a daily salad with dressing that contains added sugar?
Is your idea of aerobic exercise doing housework and walking about at Walmart?
The calcium score can be lowered, says Dr. Santora, but not without pinpointed changes in diet and exercise habits.
Lowering Your Coronary Calcium Score

G.steph.rocket, CreativeCommons
Think whole foods in their natural state.
Not foods that come in a box, can or bag. Exceptions are all-natural whole grain foods, or the actual grains, that are sold in plastic bags.
• Go very light on red meat and eat only grass-fed beef; grain-fed beef contains a lot of “bad” fats.
• Replace chicken from frozen dinners with whole chicken.
• Eat a lot of wild-caught fish.
• Don’t even look at processed meats.
• Eliminate foods with white flour, high fructose corn syrup and sugar.
• Avoid partially hydrogenated vegetable oils.
• Eat as many raw vegetables as possible and snack on fruit.

• Adherence to such a drastic change in lifelong eating habits can be very daunting for most people.
If this means occasionally indulging in a single serving of forbidden foods (e.g., candy, cake, a donut, slice of pizza, pretzels) to prevent burning out from the natural diet, then do so…with control.
For many people, 100 percent elimination of favorite foods is simply not possible.
Otherwise, battling to achieve this could collapse their discipline.
Embrace Exercise
Exercise should include strength training (e.g., weight machines, free weights, tension tubing) and cardio workouts (e.g., group fitness classes, hiking, jogging, martial arts, inline skating).

Shutterstock/Straight 8 Photography
A lengthy visit to Costco does not replace your exercise session for that day.
Supplementation
Supplements that will help lower calcium score (in combination with the other lifestyle changes just mentioned) are niacin (vitamin B3) and vitamin D3, along with magnesium citrate, turmeric, green tea, aged garlic extract, fish oil and plant sterols.
Though there is some controversy over whether or not some of these supplements actually aid in lowering calcium score, there are plenty of studies (e.g., Malinski et al, Kuriyama et al), showing that all of these supplements are very beneficial to heart health.
Dr. Santora says, “I had my first heart scan in 1999, and then every two years since, and have had a reversal of some plaque.
“But remember, you do not have to reverse the plaque; you just need to stabilize the plaque so that it does not rupture.
“Studies [e.g., Journal of the American College of Cardiology, March 26, 2013] show that if the plaque does not progress more than >10 percent per year; the chance of a heart attack is low.”
If you’ve never had your calcium score taken, this is something you’ll want to consider — depending on your risk factors for coronary artery disease and your age.
Dr. Santora’s areas of interest include interventional cardiology – coronary stenting; cardiac CT – CT angiography, and coronary calcium screening with EBCT. He is board certified in cardiovascular disease and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Brian A Jackson
Can a Blood Test Tell if You Had a Heart Attack?
A simple and highly sensitive blood test can detect if you just suffered a heart attack–and this test is so super sensitive that it can detect even a mild heart attack.
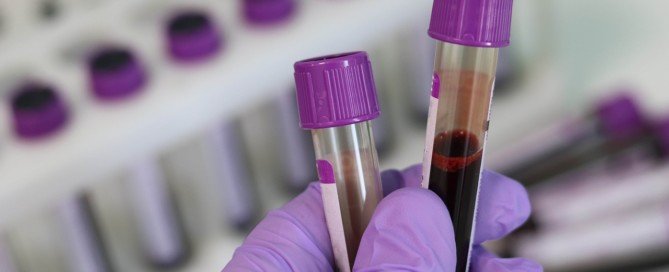
The blood test is for an enzymatic protein called troponin. The troponin blood test for heart attack is highly sensitive and is considered the gold standard for determining damage to cardiac muscle.
“Cardiac enzymes are chemicals contained within heart cells,” says Christopher J. Hanifin, PA-C, who was previously a physician assistant in open heart surgery with Cardiothoracic Surgery of South Bend in South Bend, IN.
“Normally, they are essentially undetectable in the bloodstream,” continues Hanifin.
“When a person suffers a heart attack, cells in the heart die and rupture, releasing these enzymes into the blood where they can be detected.
“Diagnosis of a heart attack (myocardial infarction) is usually based upon the detection of elevated levels of these chemicals in the blood.”
If you go into an emergency room complaining of current or recent chest pain, the doctor or physician assistant will order a blood draw to check your troponin levels.
“So if a patient goes to the emergency department with chest pain and their cardiac enzymes tests are negative, are they in the clear? Not necessarily,” says Hanifin.
“It takes some time for cardiac enzymes to appear in the blood. If a patient is tested in the early stages of a heart attack, it is very possible that their levels will be within normal ranges.”
However, an elevated troponin level alone should not be used to outright diagnose heart attack.
Conditions other than heart attack can result in elevated troponin such as chronic heart failure , atrial fibrillation, kidney failure and a blood clot in a lung.
It’s never elevated by accident. As mentioned, this blood test is super sensitive.
So if the troponin is elevated, something has happened or is going on.
Chest Pain in the ER
The marvel of this blood test is that it can detect a heart attack that occurred more than a day previous, since troponin levels remain elevated in the blood for that long.
It can stay elevated for one to two weeks.
If you present with chest pain or a complaint of recent chest pain, a nurse will promptly take a blood sample.
Results may be in within 30 minutes.
Patients with chest pain and other worrisome symptoms may be told that the first test result is “normal.”
This is NOT a good time to leave the emergency room.
“A single negative test provides little useful information aside from establishing a baseline level,” says Hanifin.
“If the patient is held in the emergency department and several tests are drawn and compared over the course of several hours, a much more confident diagnosis can be made.
“If the levels remain steady, there is less grounds for concern. If the levels are rising – even within the range considered ‘normal’ – further investigation is warranted.”
Troponin takes a while to elevate if you’ve had a heart attack, so the second blood draw will be taken at least four hours later.
Depending on that result, a third one will be taken at least four hours later.
Hanifin explains, “The take-home message for both providers and patients is fairly simple.
“A positive test can be great at ruling a disease in, but one must be extremely cautious in assuming a negative test rules something out.”
 Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University, NJ.
Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University, NJ.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Catheter Angiogram vs. CT Angiogram for Heart Disease Detection

So which is better for diagnosing heart disease: CT angiogram or a catheter angiogram, which is invasive and carries big risks?
Are you aware of the less-invasive procedure of CT angiography to obtain images of blocked arteries in your heart?
The CT angiography also goes by the name computed tomography angiography (CTA).
It’s not as expensive as the invasive angiogram, the latter requiring catheterization (tubes) inserted into your body — beginning at the groin and threaded through the blood vessels leading into your heart.
Angiography via catheter carries the same risks as major surgery, including blood clots, cardiac arrest and infection.
A CT angiograph, however, does not pose these risks, and according to a study done at Thomas Jefferson University, the CT angiography is a good alternative for people who had a cardiac stress test (usually done with a treadmill) indicating coronary artery disease — but also have below a 50 percent chance of having significant blockage.
Why would a person undergo a cardiac stress test in the first place?
Some people, upon reaching a milestone age such as 50, will undergo this procedure simply to see if their heart is healthy.
Others will be spurred by a family member’s recent heart attack or, perhaps, a stent placement after the family member complained of symptoms.
And while others will get the test ordered due to complaints of symptoms such as chest pain and shortness of breath upon mild exertion.
In either group of patients — those without symptoms and those with symptoms — a positive stress test (showing blockages in the arteries) — a referral is often given for a cardiac catheterization.
The TJU study showed that even for patients with chest pain, the CT angiogram was a viable alternative that could effectively triage those patients.
What exactly is a CT angiogram?

CT (“CAT”) scan. Shutterstock/Tyler Olson
“CT angiogram is preferable, as it is a non-invasive test, particularly for patients who are likely to be NOT requiring stents or need to be treated with medications only,” says Asim Cheema, MD, who’s board certified in internal medicine, cardiovascular diseases and interventional cardiology by the American Board of Internal Medicine. Dr. Cheema is with Your Doctors Online, an online doctor chat site.
The CT angiogram involves lying in the CT scanner, after being injected with a contrast dye to show images of the coronary arteries.
The test is painless but does come with radiation exposure from the CT scanner.
This is something the patient will have to speak to his or her doctor about, as far as any increase in the risk of a future cancer development.
Nevertheless, the CT angiogram does not pose any immediate life-threatening risk such as a stroke, heart attack or infection — though a life-threatening allergic reaction to the dye can happen in very rare cases.
Amount of Radiation
The amount of radiation received from one CAT exam is the equivalent of about the same amount of “background” radiation a person receives over a time period of eight months to three years.
Background radiation comes from naturally occurring radioactive materials. CAT scans are not recommended for pregnant women.
Possible Side Effects
Though a life-threatening allergic reaction to the contrast dye is rare, less serious complications can occur, such as nausea, flushing and itching.
Kidney damage can also result. People with the following conditions may not qualify for a CT angiography:
- Kidney problems
- Diabetes
- Pre-existing allergy to contrast dye
- Weight of over 300 pounds (some X-ray tables do not support this load).
This all sounds scary, but here are possible complications of the angiogram (cardiac catheterization), but note that they are rare:
- Heart attack
- Stroke
- Injury to the catheterized artery
- Injury to the heart
- Excessive bleeding
- Blood clots
- Kidney damage
- Allergic reaction to the dye (yes, a dye is used for this procedure too).
- X-ray exposure should also be considered.
The biggest risk of all, however, is having extensive blockage in your arteries (coronary artery disease), and delaying getting an accurate diagnosis.
If a cardiologist recommends that you need a catheter angiogram, there’s a very good reason for this, as the CT angiogram is NOT the gold standard for identifying the details of heart disease. Only the catheter procedure is.

Your Doctors Online offers a free 7 day trial where you can ask a doctor questions online and get answers in minutes from anywhere 24/7. Learn more here. Dr. Cheema teaches and provides supervision to graduate students at the Institute of Medical Sciences, University of Toronto.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/MAD.vertise
Sources: sciencedaily.com/releases/2010/04/100421162617.htm; radiologyinfo.org/en/info.cfm?pg=bodyct#part_nine

How to Extend Lifespan After a Transient Ischemic Attack

There are simple ways that you can lengthen your lifespan after suffering from a transient ischemic attack (TIA).
A TIA is linked to a shorter life span, but specific steps will increase one’s life span.
Research says that a mini stroke (aka TIA or transient ischemic attack) can shorten a person’s life span – by up to 20 percent over a nine-year period.
A TIA in and of itself does not shorten life span.
Rather, it is an indicator or marker of things about the patient that can shorten life span.
You can’t die from a TIA (but you can die from a stroke). However, a TIA means a high risk of stroke and increased risk of future issues that may reduce life expectancy, says the paper which appears in the journal Stroke: Journal of the American Heart Association.
Dr. Melina Gattellari’s study recommends that doctors very closely help TIA patients manage their lifestyle for many years after the mini stroke.
- Quit smoking.
- Lose excess weight.
- Eat fewer processed foods and more fruits, vegetables and nuts.
- Exercise

And therein lies the problem, because only one of these recommendations is straightforward and not open to misinterpretation: that of quitting smoking: You either smoke or you don’t.
But just what does “exercise daily” mean?
Many people, including those who have suffered a transient ischemic attack, believe they “exercise daily” or get “plenty of exercise.”
You do not have a built-in, ready-made exercise program just because you clean the kitchen every day, shop three times a week, vacuum once a week, walk your dog or use your staircase strictly for transportation eight times a day.
You’ve ALREADY been doing these things. Post-TIA, you need to bump things up a notch.

Freepik.com/pressfoto
“After a TIA, and after controlling blood pressure and any other medical risk factors to prevent further TIAs, exercise is definitely important,” says Danielle DonDiego, DO, a family physician and obesity specialist with SteadyMD, an online program where patients can call, text or video chat with their doctor anytime.
“Exercise can keep blood pressure lower and help with circulation.”
Exercise should not be incidental; it should be “dedicated,” says Dr. DonDiego.
“As far as what type, in my opinion it’s whatever the person enjoys doing and will do, and progresses from there. I’m a big fan of resistance training for overall disease prevention and longevity.”
“Regular exercise” is that which does not include the movement of daily living that you were already doing prior to the TIA.
For example, the walking you do while shopping — slow, leisurely, laden with pauses — cannot be equated with a brisk, non-interrupted, arm-pumping walk at a park, track or residential area.
High blood pressure is a risk factor for mini stroke. Aerobic exercise, strength training and yoga will lower resting or baseline blood pressure.

The TIA patient needs to work out hard enough to produce a training effect.
Going through the motions is not enough.
“Regular exercise” means making the effort challenging — outside your comfort zone, yet not straining or painful in any way.

Shutterstock/Liderina
What You Eat
If you’ve had a mini stroke and believe you eat healthy, read the ingredients of your foods.
Avoid anything that says “hydrogenated” in the ingredients, regardless of what the front of the package says!
The FDA allows food companies to get away with labeling the front package with “Zero Trans Fats,” even though the product contains trans fats (disguised by the terms “hydrogenated” or “shortening”).
Learn the names of synthetic food additives, then stop eating products containing them, along with foods containing artificial flavors, dyes and added sugars.
It’s difficult to avoid added sugars (they are ubiquitous), but it’s easier than you think to avoid foods with synthetic chemicals and trans fats.
Healthy eating means focusing mostly on plant-derived foods with minimal processing.
Dismal Study Result
At the conclusion (nine-year mark) of Dr. Gattellari’s study, the survival rate of TIA patients came to 20 percent lower than expected.
The risks faced by one who had a TIA go well beyond the early stroke risk.
So many people who had a transient ischemic attack lose weight, stick to better eating and take up exercise in the few months following the event — only to begin letting their guard down after several months.
And then they’re back to their pre-TIA routine. They are playing Russian roulette.
 Dr. DonDiego focuses on weight management, fitness, nutrition, reproductive health, preventive medicine and managing end stage disease. Learn more about SteadyMD.
Dr. DonDiego focuses on weight management, fitness, nutrition, reproductive health, preventive medicine and managing end stage disease. Learn more about SteadyMD.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Source: sciencedaily.com/releases/2011/11/111110191946.htm

Is it Safe to Exercise After a TIA (Transient Ischemic Attack)?
If you’ve had a TIA and have not been treated for it, it’s actually very UNSAFE to exercise, says John M. Kennedy, MD.
A TIA (transient ischemic attack) is actually a “mini stroke,” or to put it another way, a temporary stroke, and that high blood pressure is a major risk factor for stroke.
Exercise, especially lifting weights, raises blood pressure. Simply adding two plus two spells potential catastrophe if a person who just had a TIA (“just” could mean weeks ago) goes out and exercises.
“I would say exercise (aerobic or strength training) is unsafe for anyone who has experienced symptoms consistent with a TIA before formal evaluation by a health care professional,” says John M. Kennedy, MD, medical director of preventative cardiology and wellness at Marina del Rey Hospital, and author of the book, “THE 15-MINUTE HEART CURE: The Natural Way to Release Stress And Heal Your Heart In Just Minutes A Day.”
Though a TIA, in and of itself, doesn’t cause permanent damage, it is a very serious issue because it signals a possible impending stroke.

Ischemic stroke blood clot. Shutterstock/solar22
A TIA involves a blood clot in the brain that temporarily prevents oxygenated blood from nourishing the part of the brain that the blocked vessel supplies.
Having a transient ischemic attack means that the blood vessels in your brain have a propensity to develop blood clots.
The next blood clot could end up staying there (a stroke) rather than dissolving (a TIA).
It is a health hazard to exercise right after having a TIA.
If you believe you’ve had a TIA, do not exercise, as this will raise blood pressure. Instead, get a full medical evaluation to find out if you had a transient ischemic attack.
Symptoms of a transient ischemic attack are identical to those of a stroke and come on suddenly:
– Tingling, weakness, numbness or heaviness on one side of the body
– Visual impairment: blurriness or darkness; sudden loss of vision in one eye
– Slurred speech or difficulty speaking
– Paralysis on one side of the body
– Alarming headache
– Cognitive impairment; confusion
– Dizziness, loss of balance, difficulty walking
– Suddenly falling with no warning
Symptoms may resolve within minutes to up to 24 hours.
You may feel perfectly fine after symptoms of a transient ischemic attack resolve.
DO NOT LET THIS FOOL YOU ! By definition, a TIA is transient, so of course you’ll feel fine afterwards!
But the next blood clot could be a stroke, which can kill you or leave you permanently crippled.

If you believe you had a TIA, don’t exercise before you find out if you indeed had a transient ischemic attack.
Dr. Kennedy explains: “TIAs are signs of a threatening ‘full blown’ stroke. Two possible causes include hypertension (high blood pressure) and certain arrhythmias such as atrial fibrillation (AF), both of which can be triggered by or exacerbated by exercise.
“After a stroke, data suggests in order to achieve the best quality of life, and greatest functional capacity, walking is the best type of exercise.”
If you suspect you had TIA, don’t delay; head straight to the ER for tests, and do not exercise or perform any challenging physical activity like carrying out heavy garbage before heading out to the ER.
 Double board certified in cardiovascular disease and also internal medicine, Dr. Kennedy’s special interest is stress and how it adversely affects a person’s delicate cardiovascular system.
Double board certified in cardiovascular disease and also internal medicine, Dr. Kennedy’s special interest is stress and how it adversely affects a person’s delicate cardiovascular system.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Does an EMG Test Hurt?

An EMG test can actually hurt.
It depends on how sensitive a person is to pain, and in the case of an EMG test, the pain can come from two sources: an electric shock delivered by the doctor, and needle pricks, which can take the form of an embedded needle that the doctor maneuvers around while it’s beneath the skin.
I sat in on my mother’s EMG test for her suspected pronator teres syndrome.
The doctor had warned her the day before, “It will be unpleasant.” The needles are a little thicker than acupuncture needles, said the doctor.
An electric shock is always an unpleasant experience, and there will be times that the doctor will increase the voltage.
I was watching my mother’s face while he applied the shock with a cell-phone-sized device that he’d press a button on for a split second.
She was lying on her back, eyes closed, while he worked on her arms. Her eyes would mildly flinch, and sometimes flinched more noticeably. Sometimes her face twitched from the discomfort.
However, in my mother’s case, most of the hurt from the EMG came from the needles.
The doctor would place a needle on her skin, then tap the top of it. At one point he embedded a needle about a quarter inch into her skin on the underside of the palm, and moved it around.
The most painful needle prick was when it was applied to my mother’s left palm, even though the doctor had tested her right palm first. She let out a good yalp when this happened.
How much an EMG test will hurt will depend upon where the needles are being applied, and how tolerant an individual is of this kind of pain.
I’d imagine that if they were concentrated on the upper legs, they wouldn’t hurt as bad.
I think what would hurt most during an EMG test is the patient’s anticipation of what the diagnosis might be.
I’d venture to say that the needle pricking of an EMG test doesn’t hurt nearly as much as the “pricking” that occurs during the extractions that come with facials.
Extractions on the nose hurt to high heaven (I’ve had them done). However, these don’t hurt nearly as much as sclerotherapy on the nose, which I have also had.
If you’ve had facial extractions, and especially sclerotherapy (at least on the nose), then the needle pricking of an EMG test certainly won’t hurt too much in comparison.
The bigger issue for some people, as far as pain during an EMG test, will be the electric shocks.
The electric currents last a split second, but EMG literature warns that these are not pretty.
Most people will find that at least some components of an EMG test will hurt, but you must realize that in order to find out what’s wrong with you (or not wrong with you), the EMG test is going to have to hurt.
Despite the pain or discomfort, this neurological testing procedure is perfectly safe, and my mother’s doctor said that a person can have an EMG test “all day long and it won’t harm them.”
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Roman Zaiets

Chronic Subdural Hematoma: How Long to Heal

How long does it take for chronic subdural hematoma to resolve completely?
Chronic subdural hematoma refers to gradual, slow bleeding in the brain that can be caused from getting hit in the head, but how long does it take for this condition to completely resolve?
This varies. My mother experienced chronic subdural hematoma.
Usually, chronic subdural hematoma is born when a person gets hit in the head, or bumps their head, but the risk is much higher in the elderly, especially if they’re on blood thinners.
My mother was on two blood thinners at the time she fell in the bathroom and hit her head on the bathtub.
The first symptom of this accident, other than the visible wound that I saw soon after I helped her to her bed after the fall, was a debilitating headache and lower body weakness … six weeks after she fell.
That day she was diagnosed with chronic subdural hematoma.
Nine and a half weeks later, the neurosurgeon declared my mother completely clear of the chronic subdural hematoma.
The CAT scan of her head was clean, normal, and she was discharged from his care.
This doesn’t mean that it typically takes nine weeks for a chronic subdural hematoma to resolve.
In the case of my mother, there is strong reason to believe that a second fall caused a setback.
One need not strike their head to cause a chronic subdural hematoma, or create a setback in a healing cSDH.
If a fall or sudden motion (such as riding in a car in which the driver slams on the breaks) causes a jarring motion of the head in an elderly person, this can shake things up with the brain’s blood vessels.
And if there’s already a tear in a vein that caused a chronic subdural hematoma, than this jarring can cause more tearing, and hence, more bleeding.
My mother had a recurrence of the cSDH; the symptoms of this began about 10 days after the burr hole draining of the first chronic subdural hematoma.
The neurosurgeon was not able to rule out that her second fall (in which she did not hit her head, but jarred it) didn’t cause the recurrence, even though recurrence happens about 15 percent of the time after drainage.
If a chronic subdual hematoma produces symptoms, it will almost always require surgical draining.
The neurosurgeon will then “follow” the condition with CAT scans.

CT scanner. Liz West, Boxborough, MA, CC Wikimedia Commons
The CAT scan will show how much blood and cerebral spinal fluid is still in the brain, and how old the blood is.
Over time, follow-up CAT scans should show a diminishing amount of blood.
The surgical draining will not get rid of 100 percent of the blood, but is designed to get rid of enough to:
1) relieve symptoms, and 2) promote the healing process, which is the body resorbing the fluid and the veins healing.
While a patient is healing from chronic subdural hematoma, blood thinners will be off limits, and the patient must take vigilant precautions to avoid hitting their head or experiencing any jarring motions.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}