

World’s Strongest Toddler, Liam Hoekstra, on TLC: Hype or Hypertrophy
Liam Hoekstra was born in 2005.
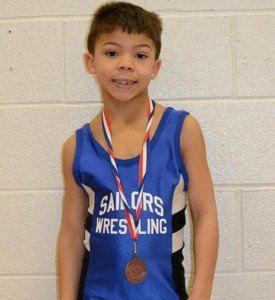
The World’s Strongest Toddler aired in 2014 on TLC about 3-year-old Liam Hoekstra, a pint-size boy from Roosevelt Park who has 40 percent more muscle mass than typical 3-year-olds.
Liam Hoekstra, “the world’s strongest toddler,” has a rare condition called myostatin-related muscle hypertrophy. Hypertrophy means increased muscle mass.
But Liam Hoekstra is small for his age. Liam Hoekstra, “the world’s strongest toddler,” does not have big muscles, but he’s rather buff.
The world’s strongest toddler does not have a soft, “baby” look to his body, and has very little body fat.
His mother Dana says he’s always hungry and eats large quantities of food, but oddly, the show did not report how many calories a day he eats.
The World’s Strongest Toddler talked about several feats of strength that Liam Hoekstra has performed in the past. But again, strangely, there were no videos shown.
The World’s Strongest Toddler said Liam Hoekstra was walking at five months. If YOUR baby was walking at five months, you’d take a video. The show provided no video evidence.
The World’s Strongest Toddler said that Liam Hoekstra was moving furniture around before his second birthday.
Again, why weren’t videos of this shown? Seems to me that if a person sees their 19-month-old baby pushing around furniture, they’d immediately grab the video camera.
If they didn’t own a video camera, this would be a pretty good reason to go out and buy one, and then film the feats of strength.
The World’s Strongest Toddler gave the viewer only a photo of a baby Liam Hoekstra being held up by an adult into a standing position by his hands; he appeared to be about six months old.
The greatest feat of strength that the show gave us, was Liam Hoekstra climbing a gym rope.
Barefoot, he was able to slither up the last several feet, though however, at the bottom, he got a little assistance with his feet.
Nevertheless, even just for several pulls without the assistance at the top, that was impressive.
The video conveniently left out the entire climb; we see only the begining, and only the end.
Liam Hoekstra did 17 sit-ups in one minute, though it was not clear if his feet were anchored; only the first sit-up was shown, and his feet were not anchored, and this first sit-up appeared to be a sample sit-up before the actual test.
The other 3-year-old boy, whom Liam was being compared to, could only do one sit-up.
Liam’s grip strength is the equivalent of a 7-year-old. He’s able to do a pull-up, though not from a pure hanging position with straight legs; his legs were bent and flopping around, which makes the pull-up easier.
However, other kids in his preschool class weren’t even able to do even THAT; they had to put their feet against a wall in order to even attempt a pull-up, and most couldn’t even do the pull-up that way.
So, it’s clear that Liam Hoekstra is definitely stronger than most other 3-year-olds and slightly older kids, but at this point, without video evidence, I can’t believe he was walking at 5 months, moving furniture, and I think the show said he was climbing up stairs at 12 months or something like that.
The World’s Strongest Toddler spent too much time showing Liam Hoekstra doing things that I myself have seen other kids about his age doing, including hanging effortlessly on bars (though not doing pull-ups).
The World’s Strongest Toddler showed the boy running just slightly faster than another 3-year-old, but this wasn’t convincing, because in any random pair of preschool boys, usually one runs ahead of the other.
I would have loved to know what Liam Hoekstra’s time for a 30-meter dash would have been, and then compared to that of 10 other 3-year-old boys.
Liam Hoekstra and the other 3-year-old (who only did one sit-up) were instructed to do pushups.
Neither of the boys understood how to do a pushup, but then Liam, while in a sunken pushup position, casually flipped over and supported himself on one hand, in a side-bridge position, to look at his father, sustaining the bridge position. A 3-year-old normally cannot do this.
The World’s Strongest Toddler said that Liam Hoekstra’s adult-height projection was 5-6.
Later in the show, his father told a highschool football coach that it was 5-6 or 5-8.
This creates a problem, because the father dreams that his son will play pro football.
This short stature eliminates a number of sports; it would be useless to prime Liam Hoekstra for Olympic-caliber swimming, though he takes swimming lessons, and his swim instructor says he has the makings of a great swimmer.
Short stature is an impediment in elite-level swimming, but certainly not diving!
The World’s Strongest Toddler noted that should Liam Hoekstra become serious one day about sports competition, his genetic condition might be seen as an unfair advantage.
Well, we can attribute an “unfair advantage” to many Olympic athletes. Take Michael Phelps.
His height, relatively long torso, relatively short legs (less drag in the water), and relatively huge feet (like fins), can be considered genetic anomalies that give him an “unfair advantage” over other swimmers.
An NBA player who stands 7-2 has an unfair advantage, no? Or how about that super thin marathon runner, or that very short gymnast?
Or that giant-slalom skier with the relatively LONG legs that provide a solid base of support while skiing downhill?
One has to wonder how many Olympic or pro athletes might have the same genetic condition that Liam Hoekstra has, and were simply never tested for it.
It was only by chance that Liam Hoekstra was diagnosed. His grandfather was boasting about the boy’s strength to his friends, one of whom was a doctor.
The doctor became intrigued and recalled reading about cows that had abnormal muscle mass due to a genetic anomaly, and he wondered if perhaps Liam Hoekstra might have the same condition. One thing led to another, and soon, Liam Hoekstra was diagnosed.
Now what if Gramps never boasted to the doctor?
Liam Hoekstra could have gone on to be just an ordinary boy who had a very fast metabolism, ate a lot, had unusual muscle definition for his age, and was a little stronger and faster than other kids his age.
And as he got older and excelled in sports, nobody would be accusing him of having an unfair advantage, because nobody would know about his genetic condition, because it wouldn’t have been diagnosed, because Gramps kept his mouth shut.
The reality is that the whole town knows about Liam Hoekstra, and now, after TLC’s airing ot The World’s Strongest Toddler, the whole nation knows.
The World’s Strongest Toddler showed Liam Hoekstra climbing a refrigerator, but — oddly again, the video footage was shown in TWO segments! Dang !
The first segment showed him grabbing the refrigerator’s handles and hoisting himself upward, feet against the appliance. He then reached for the top of the appliance.
Just when I thought I was going to see Liam Hoekstra amazingly hoist himself higher and hang from the top, the footage switched to another angle, showing him ALREADY hanging at the top! A crucial transition element was left out!
The World’s Strongest Toddler made no mention of the possibility that Liam Hoekstra could grow into his strength, or, to put it another way, his biological age could catch up to his biological strength at some point.
Will he always have 40 percent more muscle mass than kids his age and then the average adult?
Or will his muscle development slow down and eventually match pace with his chronological aging?
Ideal sports for Liam Hoekstra, considering his adult-height projection: Sport climbing (big time!), Gymnastics, Power lifting, Sprinting (some elite sprinters are short), Rugby, Soccer, Cycling.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

What Does “Inflammatory Lung Disease” Really Mean?

Have you or someone you know been told they have “inflammatory lung disease”?
“Inflammatory lung diseases are clinically and histopathologically [under the microscope] a group of acute and chronic conditions,” begins Sashini Seeni, MD, a family medicine practitioner with DoctorOnCall, an online doctor and pharmacy.
“These disorders may affect the pulmonary vasculature, airspaces, pulmonary interstitium or a combination of these three anatomic compartments,” continues Dr. Seeni.
When my mother went to the ER the second time during a bout with pneumonia (she had vomited and complained of faintness and had clammy skin), a CT scan was ordered due to an elevated D-dimer.
The ER doctor said that the CAT scan showed that the pneumonia was gone (though my mother still had a bad cough).
The doctor then informed her, “The scan also shows that you have inflammatory lung disease, and this is not part of the pneumonia, which you no longer have.”
Interestingly, prior to the CT result, my mother had a chest X-ray that the doctor said still showed some pneumonia.
So I asked, “Then what was on the chest X-ray that you said a while ago showed some pneumonia?”
The doctor replied, “That’s scar tissue from the pneumonia. We know now from the CT scan that the pneumonia’s gone.
“Pneumonia tends to show on an image in a lobe of the lung, but the inflammatory lung disease shows as diffuse.
“I recommend a follow-up with your regular doctor or a pulmonologist to have your lung function checked.”
I asked the doctor for a more definitive explanation of this “inflammatory lung disease,” but he said it was difficult to be more descriptive at this point, and that’s why the follow-up was necessary.
I asked if this inflammatory lung disease could be caused by the pneumonia. He said no, pneumonia does not cause inflammatory lung disease.
I left the ER thinking that my mother possibly had some early stage lung disease! What was this inflammatory lung disease?
Inflammatory Lung Disease Could Be MANY Conditions
“Inflammatory lung disease can be divided into two subtypes which are infectious and non-infectious,” says Dr. Seeni.
“Non-infectious inflammatory lung diseases may be idiopathic [no known cause] or may represent a secondary reaction to autoimmune diseases, infections, environmental exposures or drugs.
“Meanwhile, some possible causes of infectious inflammatory lung diseases are tuberculosis, histoplasmosis and blastomycosis.”
COPD
“Chronic obstructive pulmonary disease (COPD), asthma and pulmonary fibrosis are the result of ongoing inflammatory processes,” says Dr. Seeni.
“COPD affects both the airways and lung tissue.
“This can manifest as a combination of emphysema and chronic bronchitis.
“COPD patients are most likely to have a smoking history.”
In addition, “Lung fibrosis is a chronic lung disease where the lung scars and thickens and that can affect oxygen exchange.
“The cause of lung fibrosis is unknown but for some reasons, it is believed to happen due to infection of the lung.”
Ground Glass What?
Next day I contacted my mother’s doctor’s office and spoke to the nurse.
I learned that the preliminary report of the CT scan, sent by the emergency room doctor, stated, “Granulatoma with change and ground glass opacities.”
It took me a while, but I finally recalled that several years ago, a “granuloma” was noted on a chest X-ray of my mother.
A granuloma is a dense collection of scar tissue that indicates previous infection and is harmless.
But what was this “ground glass opacities”?
Pneumonia can cause diffuse-pattern ground glass opacities (GGO) on a CT scan.
GGO can also result from an error in image interpretation, plus unreliable aspects of the imaging technology itself!
GGO can also appear as a result of normal breathing!
In short, GGO is a nonspecific radiologic finding that has a lengthy list of causes.
My mother had the follow-up, and the doctor apparently didn’t even mention the ground glass opacities, and was awaiting the more detailed report from the ER.
A phone appointment with my mother was made for two weeks later to discuss that more detailed report.
Two weeks later my mother’s doctor called and told her everything was normal, and that no further follow-ups were necessary.
The lesson here is: If you’re told you or a family member has “inflammatory lung disease” or “ground glass opacities” as revealed on a CT scan or X-ray, respectively, do not panic or lose sleep.
However, you should be quite discerning and inquisitive about this finding. Do not be reluctant to ask a lot of questions.
 DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Sources:
erj.ersjournals.com/content/24/3/502.full
ehow.com/about_5489647_inflammatory-lung-disease.html
medicalcenter.osu.edu/patientcare/healthcare_services/lung_diseases/lung/interstitiallung/Pages/index.aspx
mayoclinic.com/health/granuloma/AN00830
appliedradiology.com/Issues/1998/12/Articles/Ground-glass-opacity-on-CT-scanning-of-the-chest–What-does-it-mean-.aspx

How Does Feeling Depressed Cause Constipation?

Depression can cause constipation. However, if your depression has caused constipation, you may not even know it.
“The range of normal bowel movement frequency is from one BM in three days to three BMs in one day,” begins David D. Clarke, MD, President, Psychophysiologic Disorders Association, Clinical Assistant Professor of Gastroenterology Emeritus, Oregon Health & Science University, Faculty Associate, Arizona State University.
Dr. Clarke continues, “Fewer BMs than this is considered constipation. In depression, though definitive studies are lacking, when constipation occurs it is likely that it results from slowing of the muscle contractions of the large intestine (colon).
“The slower contractions cause the feces to move more slowly. In addition, the resulting greater duration of contact of the feces with the colon results in more water being absorbed — causing the stools to harden.”
The information you’re about to read is based on my mother’s constipation, and how her depression led up to it.
A person with major depression typically abandons their usual eating habits and lessen water intake.
My mother one day complained of constipation. But she had had this several times before during her course of depression. We thought it might be related to side effects of painkillers.
- But this time, we couldn’t blame painkillers because she had quit taking them not long prior.
- And this time, the constipation was not resolvable.
We took her to the ER and the doctor said she had a huge bowel movement that couldn’t make an exit, and he’d have to “dig it out.”
Later the doctor said there’d been about two feet worth of bowel movement, and that there was still more BM in there.
How could this be, if my mother had reported a bowel movement that morning, and if she’d been having bowel movements over the past many days?
The doctor said that a person could have bowel movements and simultaneously develop chronic constipation, in that while bowel movements may occur daily, fecal buildup occurs inside the colon over time: a simultaneous process.
He said that my mother’s bowel movement buildup may have taken place over a few weeks’ time, all while she was actually having bowel movements every day or almost every day.
She had compacted fecal material in the colon, and on that fateful day, it caught up with her and resulted in constipation that did not respond to edemas, suppositories or time.
Coinciding with the past few weeks were erratic eating habits, excessive inertia and low water intake.
These three problems were from depression, even though my mother was on an antidepressant.
The problem was that beginning a few weeks prior, the antidepressant lost steam and had to be increased in dosage.
There were a few days there where depression symptoms returned, thus suppressing my mother’s desire for food and fluids.
After we increased the dose, everything was fine, but then she started showing signs of relapse again.
This time we wondered if the increased dose was causing the extreme lethargy, fatigue and desire to sleep all the time. And once again, her appetite and desire for fluids was suppressed.
Even on better days, my mother didn’t eat so well, and she was never one to drink much water.
Erratic eating habits, going long periods without food, and inadequate water intake (all common results of depression) can very much lead to constipation in the form of built-up fecal material.
Depression also causes inertia and the desire to sleep a lot or just sit around not doing anything.
We noticed that my mother, after responding well to the antidepressant, was gradually beginning to want to spend more and more time sleeping or sitting around.
We wondered if the antidepressant was losing its steam again.
At any rate, all that inactivity contributed to the constipation because inertia suppresses voiding.
My mother was eventually diagnosed with hypothyroidism (several days before the major constipation episode), and it’s possible the clinical depression was secondary to the hypothyroidism, which would explain why she began showing signs of relapse despite being on 90 mg of the antidepressant.
The hypothyroidism perhaps began escalating and apparently was fighting against the antidepressant.
But even after she began taking Synthroid for the hypothyroidism, the extreme fatigue continued getting worse. This didn’t make sense…
…Until the ER doctor informed us that she had all that backed-up fecal material in her, stuck inside three feet worth of colon.
We were given instructions on what to do to get the remainder of bowel movement out over the next few days.
As a bunch of bowel movements began coming, once the home treatment started, my mother’s energy returned.
It’s a vicious cycle: Depression causes inertia. Inertia leads to constipation. Backed-up fecal material that’s been sitting in the colon for days and days will weaken the body and drag it down.
If you know someone who has depression and is getting increasingly tired and fatigued, despite being on an antidepressant, consider the possibility that he or she has impacted fecal material inside their colon, weighing them down and making them feel sick.

Since 1983 Dr. Clarke has successfully cared for over 7,000 patients with stress illness.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Excessive Crying in Adults: Causes & Solutions

Are you an adult who cries too much?
Are you an adult who cries excessively?
Just how abnormal is it for an adult to be prone to excessive crying episodes?
There are different kinds of crying, and different reasons for such, in the adult.
Many times, the crying is a normal reaction to an agonizing event.
Sometimes an adult will cry out of happiness.
I’ve witnessed adults crying after winning something on “The Price Is Right.”
The issue, however, is when the adult cries too often, excessively, out of proportion to life circumstances.
I once read a letter to an advice columnist from a woman who said she cried over everything, including the opening of a new K-Mart.
Why are some adults prone to so much tearfulness?
“Most likely the crying is related to a heightened emotional state which is caused by some stress in the person’s life,” explains Peter Swanljung, MD, chief of psychiatry at the Malvern Institute in Willow Grove, PA.
Someone may cry when the K-Mart opens, but they are not really crying about the K-Mart opening; rather, they are releasing emotions related to other issues going on in their lives.”
Some people begin weeping and sniffling while watching sappy movies or TV shows like “Little House on the Prairie.”
When I was in college, a group of us were in the TV lounge watching the 1939 version of “The Wizard of Oz.”
While Judy Garland was singing “Somewhere Over The Rainbow,” one of the female students began quietly weeping.
I don’t recall if I heard her sniffling, but I clearly recall another girl commenting in a sort of teasing way, “She’s crying!”
The weeping girl loved rainbows and had them all over her room.
Some adults will easily weep over very trite but isolated, specific events such as someone singing; whereas other adults will literally cry “over everything.”
Frequent crying episodes are not uncommon in someone with clinical depression, but this article refers to “otherwise normal” adults who just get too emotional.
Sometimes the tears are in reaction to a pleasant event (or seemingly a reaction to), such as the K-Mart opening or Judy Garland singing.
And sometimes the tears result from something negative, such as being chastised by one’s boss.
How many times have we heard of women running to the bathroom and crying after being chewed out by their boss?
Dr. Swanljung explains, “Meeting with a therapist may help a person understand what issues or stressors may be causing this heightened emotional state, and they may then be able to work on resolving or coping with these issues.”
If excessive crying in your adult life is interfering with social interactions or makes you uncomfortable, consider seeking professional help to discover the underlying cause.
Don’t assume this is something that’s just a part of you that can’t be remedied.

Dr. Swanljung is the former medical director of the general adult unit at Friends Hospital in Philadelphia and treats a variety of psychiatric conditions.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Does Fasting Glucose Reading of 106 Mean Insulin Resistance?
If your fasting glucose is about 106, do not panic, as this does not automatically mean you have insulin resistance or prediabetes.
A few years ago I visited a general practitioner to find out why I was suddenly having a lot of diarrhea.
I decided to add in a routine physical, which included the standard fasting glucose test.
The result was 106, which netted a “flag” alert in the report, that was e-mailed to me.
The test result came a few days before my visit, and the doctor merely mentioned that it was flagged, but not to worry about it.
Several months later I was reviewing my medical paperwork and saw the printed-out blood glucose result. In the next column it said “impaired glucose metabolism.” WHAT?!
A normal fasting blood sugar reading is 70-100 (mg/dL).
The American Diabetes Association says that 1-2 hours after eating, the fasting glucose (blood sugar) reading should be under 180 mg.
The ADA says that over 125 for fasting glucose means diabetes.
So what does 106 mean?
According to Kaiser Permanente (my HMO at the time of the blood sugar test), a normal fasting glucose result is “less than or equal to 110 milligrams per deciliter.”
Two years ago, however, their normal range was under 100, which was why my result of 106 was flagged.
The Kaiser site for test result information is open only to members, and it states:
“These ranges vary from lab to lab, and your lab may have a different range for what’s normal.
“Your lab report should contain the range your lab uses. Also, your doctor will evaluate your results based on your health and other factors.
“This means that a value that falls outside the normal values listed here may still be normal for you or your lab.”
The site lists factors (other than diabetes) that can cause a high blood sugar reading, and first on the list is “Stress.” This information was not there two years prior to my checking it.

Shutterstock/Gustavo Frazao
If you have a fasting blood sugar reading in the low 100s like mine was, ask yourself how much stress you’ve been under lately.
As a former personal trainer, I am well-versed in blood sugar’s impact on the body, as this is the main fuel source for working muscles and is highly manipulated by exercise and diet.
If you’re under chronic stress, your body is in a perpetual “fight or flight” state.
To prepare for the fight or flight, the liver dumps sugar into the bloodstream as a ready fuel source for muscles.
In chronic stress, however, the fight or flight never comes, and blood sugar remains elevated.
A bout of intense exercise will lower the blood sugar and keep it lowered for awhile, but if the stressor doesn’t go away, the fasting blood sugar may bounce right back up again into the low 100s.
For eight weeks prior to my fasting glucose test, I was under extreme emotional duress – it was really ugly, and I developed microscopic colitis as a result (which caused the diarrhea).
However, disrupted sleep can cause insulin resistance (elevated fasting blood sugar that’s not elevated enough to qualify for diabetes).
David Edelson, MD
For my article titled “Can Poor Sleep Cause Insulin Resistance,” I interviewed Dr. David Edelson, MD, board certified in internal and bariatric medicine, one of the top obesity experts in the U.S., and founder and medical director for HealthBridge.
“There is a strong association between sleep disorders and both obesity and insulin resistance,” explains Dr. Edelson in my article.
“When I refer to sleep disorders, I am speaking of anything that can cause either a lack of sufficient quantity of sleep (insomnia, lifestyle issues) or poor quality (sleep apnea, restless legs, fragmented REM sleep, etc.).”
In fact, insulin resistance (prediabetes) can be caused by just one night of bad sleep, says a report in the Journal of Endocrinology & Metabolism (2010).
“Our data indicate that insulin sensitivity is not fixed in healthy subjects, but depends on the duration of sleep in the preceding night,” says the report.
Not only was I experiencing horrendous anxiety for eight weeks, but throughout that eight weeks, my sleep was disrupted every single night.
After doing my homework about what an elevated fasting glucose might really mean, I was not surprised mine came in at 106.
I was in a fight or flight mode every waking minute, which included lying in bed with a racing heart from the anxiety, unable to sleep soundly.
Two years later I had another fasting glucose test: 85. The stressors of two years ago were well-behind me.
Based on just one blood sugar test of around 106, you should not jump to conclusions and assume you have prediabetes or insulin resistance, especially if you exercise, are not overweight and have a pretty healthy diet.

Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Depression Treatment: T3 Better than Antidepressants

T3 just may work better on depression than antidepressant drugs.
A large percentage of people suffering from depression actually have low thyroid, says Dr. Kent Holtorf, MD, thyroidologist and founder of Holtorf Medical Group in California.
In other words, many people’s clinical depression is caused by underactive thyroid (hypothyroidism) and they don’t even know it, and hence, are unaware of a highly effective treatment: T3.
Hypothyroidism (underactive thyroid) is associated with weight gain, fatigue and feeling cold, but depression is also a common symptom, and may even be the only symptom.
“The largest study done on the treatment of hypothyroidism with antidepressants found that supplementing with the thyroid hormone T3 worked as well or better than all the antidepressants,” says Dr. Holtorf.
“This is one of the hundreds of studies that demonstrate that a large percentage of patients with depression are actually low thyroid.”
Physicians are missing this cause of depression (low thyroid) left and right, and instead, writing out the prescriptions for antidepressants in droves.
The Star*D report is the largest trial, with over 4,000 patients, comparing antidepressant effectiveness for depression treatment.
Dr. Holtorf says the study found that “Sixty-six percent of patients fail to respond to antidepressants or have side effects severe enough to discontinue use.”
Side effects of antidepressants can actually be disabling, including dizziness, nausea, more depression, and suicidal thoughts in teen and young adult patients.
Of patients who do respond well to antidepressants, says the Star*D study, more than half will relapse within a year.
However, this investigation found that “T3 was effective even when other medications — such as Celexa, Wellbutrin, Zoloft, Effexor, or (behavioral) cognitive therapy — were not,” explains Dr. Holtorf.
T3 was shown to be 50 percent more effective, he continues, “even with the less than optimal dose of 50 mcg, under direct comparison with significantly less side effects than commonly used therapeutic approaches with standard antidepressants.”
A standard thyroid function test, obtained by drawing blood, will not reveal low T3 levels.
Hence, a doctor reviewing a patient’s blood work will not pick up on potentially low T3 levels.
I asked Dr. Holtorf why doctors don’t order a specific T3 test when a patient presents with depression.
He replies, “The simple answer is that the tests check what is in the blood, but what matters is what is in the cells.”
The TSH (thyroid stimulating hormone) is the standard test given to people for their annual physical checkups.
Dr. Holtorf says this test is regarded as the most sensitive marker of the peripheral tissue levels of the thyroid.
However, this view is incorrect, he continues. “Most endocrinologists and other physicians erroneously assume that, except for unique situations, a normal TSH is a clear indication that the person’s tissue thyroid levels are adequate.”
Low thyroid levels are clearly a culprit in many cases of depression.
The importance of T3 levels must not be overlooked. Dr. Holtorf explains, “Not only can low thyroid cause depression, but it can make it much worse in the face of depression, so every person needs to get their thyroid levels tested.
“The problem is that the standard blood tests that are typically used by the overwhelming majority of doctors will miss low thyroid levels in depression.
“Why? What is called a free T3/reverse T3 ratio is currently the best method to detect these low levels in depression.”
For all people with depression and even bipolar disorder, a time-released supplementation with T3 should be considered as possible treatment despite a seemingly “normal” serum thyroid level, continues Dr. Holtorf.
A standard TSH test may be “normal” in a patient exhibiting classic signs of depression, but again, the standard TSH test is not sensitive to measuring T3 levels.
Though supplementation with T3 (the active thyroid hormone) may effectively treat a person’s depression, Dr. Holtorf stresses that “Straight T4 (the inactive thyroid hormone) should be considered inappropriate and suboptimal therapy for replacement in such patients.”
The thyroid supplement is not synthetic; it is bioidentical, meaning it’s the actual hormone that the patient takes every day in the form of a small pill.
Here are three study references that report the strong link of low thyroid (T3) to depression:
Int J Neuropsychopharmacology 2008;11:15-25
Journal of Affective Disord 2009;116:222-226
Am J Psychiatry 2006;163:1519-1530
 Dr. Holtorf has published a number of endocrine reviews on complex topics in peer-reviewed journals on controversial diseases and treatments.
Dr. Holtorf has published a number of endocrine reviews on complex topics in peer-reviewed journals on controversial diseases and treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

How Can Being Diabetic Cause Mood and Anger Problems?

Having diabetes is no excuse to blow your top and be angry at your loved-ones all the time, but this disease indeed could lead to factors that can alter mood and even cause ADHD symptoms.
Now on one hand, it seems there’s no connection between being easily aroused to anger, ADHD or being very moody, and having diabetes.
But on the other hand…
Now suppose an adult or child in your life has anger issues, or frequently has mood disturbances or signs of ADHD.
Diabetes As a Cause
This person can very well have diabetes, and the diabetes can very well be causing or significantly contributing to anger outbursts, moodiness and/or ADHD symptoms.
I asked whether or not diabetes can be connected to anger and mood to Dr. Georgianna Donadio, DC, a nutritionist, health educator and Program Director of the National Institute of Whole Health in the Boston area.
Diabetes Can Cause Angry Mood Problems and ADHD
“The answer is a resounding yes,” she replies. In the brain is a neurotransmitter called dopamine, and excess amounts of dopamine are associated with mood and behavioral changes.
Dr. Donadio explains, “Vanderbilt University Medical Center identified that insulin levels affect the brain’s dopamine system, which is involved in many neuropsychiatric conditions, including drug addiction, Parkinson’s disease, ALS, and so forth.”
Two Types of Diabetes
They are type I and type II. Type I is also known as insulin-dependent diabetes. The patient’s pancreas does not produce any insulin. Ten percent of diabetics have type I.
In type II, the patient’s pancreas produces insulin, but the body does not know what to do with it.
Though about 80 percent of type II diabetics are overweight, and this type of diabetes is strongly correlated with being overweight, lack of exercise and poor eating habits, a thin person can still develop type II if other lifestyle risk factors are present.
Genetics also play a role, but not in terms of destiny, but rather, in terms of predisposition.
If a person has anger problems or ADHD symptoms before developing diabetes, then if the diabetes isn’t managed properly, the condition can have a definite impact on that person’s temper and mood.
Dr. Donadio continues, “In addition, theirs (Vanderbilt University Medical Center) and other studies have provoked questions regarding how controlling insulin levels (such as in diabetes) can have an impact on and for ADD, ADHD, and this suggests that the effects of kids/adults having high carbohydrate/sugar diets may be a critical factor in the development of ADD, ADHD and other neurological/brain conditions.”
She adds: “The brain needs glucose to function properly and without proper insulin regulation, sugar levels can become erratic and seriously impact cognitive and neurological functioning.
“People with hypoglycemia often have severe glucose swings and personality issues as a result.”
Hypoglycemia is low blood sugar.
If you, or and adult or child in your life seems to have anger management issues, throws temper tantrums, has temper outbursts, rouses easily to a hostile mood, or shows ADHD signs, consider the possibility that diabetes is at least partially the cause.
 For 35+ years Dr. Donadio has educated the healthcare community, her patients, students and the public about how the physical, emotional, nutritional and environmental aspects of our lives can produce illness or wellness.
For 35+ years Dr. Donadio has educated the healthcare community, her patients, students and the public about how the physical, emotional, nutritional and environmental aspects of our lives can produce illness or wellness.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can Carnivora Cure Cancer or Are Radio Ads All Hype?

The ads for Carnivora on the “Coast to Coast” radio show are incessant and strongly hint it can cure cancer.
If you’re a faithful listener to “Coast to Coast,” then you already know that this popular program frequently runs ads for Carnivora.
What really got my attention was that the ad (in the past, voiced-over by “Coast to Coast” host George Noory, and as of 2019, by Carnivora International founder Richard Ostrow), claims that Carnivora can eradicate abnormal cells while sparing normal cells.
Carnivora is the name of a product that, according to its site is an extract of a species of Venus flytrap known as Dionaea muscipula, and comes in capsule and liquid form.
The description of what Carnivora does is actually the cure for cancer!
It would be illegal for Carnivora International to outright state, “Carnivora can cure cancer.”
Instead the company cleverly masks this bold statement with their claim — but anyone familiar with what malignancy actually is can see right through their cryptic message.
Any company that makes a thinly veiled claim like that had better be able to back it up.
“I have never heard of this specific product, but it is my opinion that these miracle cures touted on media are pure hype and not true (think ‘snake oil salesman’),” explains Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“Consumers should always take these ads with skepticism and speak with their PCP.
“Also, one should be careful about mixing these OTC treatments with whatever prescription medications they are taking; these ‘drugs’ could interfere/interact with prescription medications.”
The product’s site makes it appear as though there’s been a lot of valid, replicated research showing that the product kills cancer cells.
There are things, however, that the company doesn’t tell you, but the American Cancer Society certainly does.
According to the ACS site, there is no scientific evidence that Carnivora is effective at treating any kind of cancer.
One of Carnivora’s claims is that it can reverse skin and other types of cancer.
The ACS site explains that a German physician patented Carnivora after taking liquids from the Venus flytrap and testing to see if they could digest abnormal proteins in cancer cells.
The ACS further says that in 1985, this physician claimed that 56 percent of 210 people with cancer experienced remission or stabilization after taking the extract.
These findings were published in a “little-known German medical journal,” continues the ACS. The findings were never confirmed, either.
The active ingredient in the Venus flytrap is thought to be plumbagin.
The ACS says that claims for what the Venus flytrap can do for malignancy cannot be supported with science.
One of the radio ads on “Coast to Coast” points out that former President Ronald Reagan used Carnivora successfully, but interestingly, the ad doesn’t say for what — apparently wanting listeners to connect the dots and assume he used it for his much-publicized colon cancer.
Yes, Reagan recovered from colon cancer, but he also received conventional medical treatment including surgery!
Another point of interest: The ACS says that most of the studies involving the Venus flytrap extract were done by the doctor who patented Carnivora.
He had a huge financial stake in the clinic that administered the product, as well as in the manufacturer of this product!
The ACS states on its site regarding plumbagin:
“Although animal and laboratory studies show promise, further studies are necessary to determine whether the results apply to humans. It is important to remember that purified compounds such as plumbagin are not the same as the fresh plant extract, and study results would not be likely to show the same effects.”
- So, can Carnivora cure cancer?
- You be the judge.
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Sources:
Cancer.org/Treatment/TreatmentsandSideEffects/ComplementaryandAlternativeMedicine/HerbsVitaminsandMinerals/venus-flytrap?sitearea=ETO
Carnivora.com

Cough After Pneumonia Can Last a Few Weeks After Recovering

A doctor says that after recovering from pneumonia, the cough can persist for a few weeks.
“Yes, it is true,” says Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“It is because the damage to the lung tissue (inflammation) can take several weeks to completely heal.”
Years ago a doctor had told my mother that “I think it’s completely normal for a cough to drag on for a couple weeks even after the pneumonia is gone.”
A CT scan showed that my mother no longer had pneumonia.
She had the CT scan because a D-dimer test result was elevated, and when this result is elevated, it can indicate the presence of a pulmonary embolus (blood clot).
This was while she was in the midst of recovering from pneumonia, which of course, was characterized by plenty of coughing and hacking.
The ER doctor said that a CT scan is far more definitive than X ray, and since it showed no pneumonia, she was declared free of the infection, even though she was continuing to cough.
A few days later my mother then had a follow-up with her primary care physician.
I was present in the office and asked just how long a cough is supposed to last after one recovers from pneumonia. This came up a few times during the course of the visit.
In addition to the first verbatim quote mentioned at the beginning of this article, the doctor also stated:
“It’s absolutely normal that you still have a cough. That cough can drag on for another few weeks.
“It caused damage to the airways. Your body still has to clean everything out.
“It can be two or three months before you feel completely normal.”
This was all after I had initially asked, “Can a person still be coughing sputum after the pneumonia is cleared?”
The physician responded, “Yes. It can take a couple of weeks for all that to clear up.”
Never be “afraid” to ask a doctor many questions!
You are not expected to know what a doctor knows, and hence, doctors welcome questions.
So there you have it, stated several times by a doctor seeing my mother who, two days prior, was told that she no longer had pneumonia, but was still having occasional bouts of productive coughing-phlegm or sputum coming up.
The doctor also said that it’s good that all that phlegm is coming up, and that the patient should never swallow it.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Ruslan Huzau

Zanaflex Withdrawal: How to Get off this Drug Smoothly

Here’s best way to get off zanaflex, says a doctor.
Zanaflex withdrawal can be a very troublesome experience, but there’s a way to get off Zanaflex smoothly and safely.
Zanaflex is a drug for muscle spasms.
“The literature and common practice both dictate that Zanaflex (tizanidine) be discontinued by tapering off the drug gradually over a period of one to two weeks,” says Frederick Arthur Ehlert, MD, Cardiac Electrophysiology and Pacing division at ColumbiaDoctors Eastside, NY, NY.
“While there may be some rebound effect if it has been taken on a regular basis for a considerable period of time, gradual reduction of the dose will usually prevent any significant rebound effect.
“There is no replacement or step-down drug, just tapering, which is often easier with the tablet form rather than capsules.
“But if capsule dosage is relatively high it can be halved, and then, if necessary, one’s doctor can prescribe a lower dose to continue the tapering at a lower dose.”

Zanaflex
What are the common withdrawal effects of Zanaflex?
Dr. Ehlert: With the abrupt cessation of Zanaflex (tizanidine), there is a risk of rebound hypertension, which means a high blood pressure, which results from the sudden discontinuation, tachycardia (which means a rapid heart beat, usually a normal heartbeat going faster than normal), and hypertonia (which means muscle spasms).
Can a person just outright quit Zanaflex, and why not?
Dr. Ehlert: Why is that dangerous? The high blood pressure in this rebound effect can conceivably go very high and cause strokes or other organ damage.
Can you recommend some ways a person can go about weaning off Zanaflex, or things they can do (maybe with diet or supplements) that can ease the transition off the drug?
Dr. Ehlert: The recommended initial dose of the drug is 4 mg/day with gradual increases (in 2-4 mg increments over 2-4 weeks to a maintenance dose of 8 mg every 6-8 hrs.
Withdrawal of the medication to eliminate side effects should replicate these increases. Diet or supplements are not really helpful in this.
Remember, to get off Zanaflex with minimal problems, gradually reduce your dose with your doctor’s supervision.
 Dr. Ehlert’s
Dr. Ehlert’s

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}