

Why You Shouldn’t Compare Adult’s Squat with Child’s Squat

There is no comparison between an adult’s full squat and a young child’s full squat, yet people continue comparing the two when discussing the back squat exercise.
As a former personal trainer, it continues to amaze me at how often other personal trainers and hardcore strength training and weightlifting enthusiasts keep pointing out that if a young child or toddler could get down into a full squat, an adult should be able to do so. Bah!
Any layperson with his eyes half open should be able to see a more-than-subtle difference between a toddler’s, and even grade schooler’s, body proportions, and an adult’s, even a short adult’s.
The distance between a toddler’s hips and head, relative to their legs, is significantly greater than in an adult’s!
View a profile of a toddler in a full squat. The relatively huge head of the child below prevents him from falling backwards and provides a comfortable leverage point.

Shutterstock/Rozochka
The length between the toddler’s hips and head acts as a fabulous leveraging device that easily keeps the baby (or young child) from falling backwards, while allowing the toddler to keep his back fairly upright.
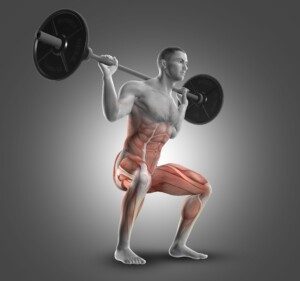
To keep from falling backwards, a person in a deep squat needs to have the shoulders vertically aligned with the midfoot.
The less length between the hips and the shoulders, the more that the person needs to lean their torso forward, to get the shoulders smack over the midfoot.
This fact of physics is SO obvious, I don’t know why it escapes so many fitness professionals and gym enthusiasts.
A young child squats to retrieve something on the floor or work with something on the ground.
Instinctively a toddler knows that if he bends over like an adult, he’ll fall flat on his head.
Toddlers and babies are top-heavy enough to tip headfirst into a bucket of water and drown; they can’t lift themselves out because there’s not enough “length” under their center of gravity to straighten back up.
A report from the U.S. Consumer Product Safety Commission states: “…the stability of these buckets, makes it nearly impossible for top-heavy infants and toddlers to free themselves when they fall into the bucket headfirst.”
I’ve read the strength training and muscle building forums, and time and time again, someone points out that if toddlers can full squat, adults can, once they stop making excuses.
Now, I’m not endorsing any excuses here. My criticism is the comparison of adult full squats to children’s full squats (also known as the Third World squat).
I might also mention that the full squat of a toddler is entirely different from the classic Third World squat, which is more of a crouch, though in some nations, an adult version of the toddler full squat is commonly used as a resting position.
Another reason the child’s squat to adult’s is an unfair comparison is because toddlers have ridiculously short femurs relative to their shins.
This is SO evident in early toddler-hood, when babies are walking across a room just in their diapers, and all you see are these shins coming out of the diaper; where are their thighs (femurs)?
The femur gets longer, relative to the rest of the body, as the child grows, but for quite a while, that femur is this short stumpy thing that provides superb leverage in a full squat, keeping the shoulders easily aligned over the midfoot because the minimal hip displacement by the super short femur minimizes the forward torso lean.
An adult’s head is one-eighth their height, on average. An infant’s is one-fourth their body length!
Though a toddler has grown quite a bit since being born, his head is nowhere near one-eighth his body length!
That big bobbing head of a toddler serves as an excellent counterforce to the mild hip displacement in a full squat!
Older children, too, have this advantage, but not as pronounced, but enough to make a comparison between even an older child’s full squat and an adult’s full squat outright ridiculous.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com
Sources:
cpsc.gov/cpscpub/prerel/prhtml02/02169.html
www.dace.co.uk/proportion_child_2.htm

Short vs. Long Femurs for Hiking

Does femur length really matter when it comes to hiking efficiency?
“Long femurs” refers to relative length of these bones to one’s overall height or leg length, and in the world of weightlifting, the issue of long femurs becomes relevant when these bones are longer than one’s torso.
A person can stand only 5-5 and have long femurs. A person can be 6-2 and have short femurs, meaning, for their height or leg length, their thighs are pretty short — they have an endless shin bone.
Long femurs are a biomechanical disadvantage in the barbell squat exercise, but an advantage in cycling due to torque (measure of force on a rotational object).
Short femurs are a big advantage for squatting, but a disadvantage in cycling.
So what about hiking?
Hiking includes descents. For hiking, long femurs come out ahead of short thighs, and remember, this is all relative to one’s overall height.
So don’t assume that every tall person has long femurs and every short athlete has stubby thighs.
Geoffrey Mutai is an elite marathon runner who has long femurs relative to his shins and overall height:

I have long femurs and stand 5-8. I finally figured out why I seem to be the only person in a group hike who can effortlessly and quickly ambulate down a talus slope.
I’ve always thought it was related to my years of playing volleyball (lots of “getting low” and “staying low”). I now think that long femurs have something to do with this.
To prevent falling on a talus slope (or any hill while descending), the hiker needs to get their center of gravity as close to the slope as possible.
This is why a dachshund has an easier time ambulating down a steep hill jutting with rocks than does a greyhound.
Long femurs also conserve energy when the hiker ascends, and I’ll explain why in a moment.
Hiking down a steep hill and especially talus slope should be done while in at least a half-squat position.
A hiker with short femurs can drop their center of gravity only so much before unnatural hip flexibility is required to sink even lower.
To understand all this, visualize hikers with wildly exaggerated body proportions.
Let’s say that Polly has one-foot long femurs and three-foot long shins. Sally has the opposite: three-foot long femurs and one-foot long shins. Both women are the same height.
Imagine Polly carefully making her way down a talus slope, sinking her hips down as much as possible. She’s still far above the ground, what with those towering shins.
Her torso/back is upright, which is good. But her center of gravity is not very low. She is prone to being off-kilter, like the greyhound.
Furthermore, it takes more energy to create long strides down the slope, as her foot is extended way out ahead of her knee, and she must then thrust her hip forward to complete the stride, whether it’s a sideways stride or three-quarters frontal (which is how one should descend talus, by the way; never descend facing fully forward).
With long femurs, Sally can sink her center of gravity really low.
This is not the same as a conventional barbell squat, because efficiently descending on talus requires the knees and feet to be wide apart and pointed out for optimal control, thereby shortening the distance between knee and hip, allowing for a more upright torso position.
In fact, for maximal control over talus, the hiker’s legs should be very wide, descending sumo style; the sumo stance allows the hiker with long femurs to be upright.
But even if at times, the feet are closer together, making the hiker with long femurs lean forward, the forward lean is okay because there isn’t a barbell across the back!
Sally’s center of gravity, like a daschund, is close to the talus. If she steps on a loose rock and starts falling, she won’t have as far to fall as will Polly, whose hips, torso, arms and head are further up, even though the hikers are the same height.
Long femurs enable Sally to complete long strides without thrusting her hips towards the stepping foot.
Imagine her descending, hips close to the ground because she is more horizontally displaced due to the long femurs.
I will admit that hip flexibility plays a role here. If a hiker has stiff hips, they’ll be inefficient at descending in a squat, regardless of femur length.
All talus descents should be done in a squat, with feet placed wide, regardless of femur length.
The closer your center of gravity is to the slope, the less likely you’ll fall, and if you do fall, you’ll have less distance to fall.
When ascending, Sally’s long femurs will have an advantage in that she won’t have to execute as much hip flexion as will Polly.
Polly can still get the job done quite well if she’s physically fit, but from a biomechanical standpoint, Sally will use less energy because long femurs will allow her to climb with less range of motion (hip flexion).
Visualize their climbing profiles using exaggerated features again, and you’ll clearly see the biomechanics.
This is easier to visualize if you replace a hill with a staircase. Polly must lift her foot up higher to get it on the next step.
With long femurs, Sally doesn’t need to lift as high (less hip flexion, smaller range of motion, less energy expended). Plus, to push off from the step, Polly must use greater range of motion.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Sources:
(clear photo of Kagwe’s legs) http://forum.bodybuilding.com/showthread.php?t=138030823&page=1
marathonchamps.com/a-JohnKagwe.html

3 Exercises that’ll Improve the Back Squat for Long Femurs
Here are three simple and fun exercises to improve back squats if you have the unfortunate levers of relatively long femurs.
Bad levers do not mean that you can’t override long femurs by “strengthening your ancillaries.”
Three Exercises for Improving the Back Squat if You Have Long Femurs
Wall squat. Stand facing a wall and figure out the closest you can be to it before your knees would be touching when in a parallel squat.
You’ll need to hold onto something to get into a parallel squat to figure out the distance you need to be from the wall. Mark that distance (e.g., place yardstick parallel to wall).
Face wall and begin squatting, making sure that there’s something nearby you can hold onto.
The objective is not to let your head or face pitch into the wall, though it’s fine if your face (or side of) grazes it as you lower. You just don’t want to lose control and pitch forward.
You will notice several things:
1) This really forces your lower back to maintain an arch
2) It stretches the back of the lower leg/Achilles tendon, and
3) As you keep doing this, you’ll find you can eventually eliminate holding onto something with your hands, and instead just allow your palms to graze the wall.
With that third point, the arms can be straight but somewhere between horizontal and vertical, palms against wall.
The goal then would be to eliminate the grazing and not touch at all. Another goal is to sink as deep as possible.
You’ll notice that as you near the bottom, you’ll lose the lower back arch. This will happen to even a person with short femurs.
I don’t recommend going this far, because you want to teach your body to always have a low back arch.
Wall squats will force your body to get good at maintaining a low back arch past a parallel position.
As you improve with wall squats, stand a little closer to the wall. This will encourage less forward positioning of the knees, but realize that your proportions will have the final say-so.
The second exercise for improving the back squat if you have long femurs is what I call staircase squats.
Ideally, there’s a solid wall on either side of you. Even more ideally, you can sit on the steps where at least one of the walls ends and you can use that for support by curving your palm and fingers around it.
- Sit on a step.
- Position feet on the next step, as you would in a back squat.
- Place heels against the back of the step.
- Arch lower back and shift forward to get knees past the feet (maximize dorsiflexion in ankles).
Every time you begin this exercise, note if your shoulder is right over your midfoot.
This is key, because once you achieve this, you’re ready to remove your butt from the step — while keeping heels on it.
The beauty of this exercise is that you never have to worry about falling backwards. The wall allows you to use something for balance without gripping it.
The objective is to eliminate using the wall as you maintain the squat position, butt just a tiny bit off the step.
Hold the squat till you fatigue, then sit and rest. Repeat several times. Concentrate on maintaining the lower back arch.
Make sure feet don’t drift outward any more than you desire, as this can happen without you realizing it.
Working off the next step can be taxing, so alternate between that and the step after the next step.
In fact, beginners may want to use only the second step down, rather than the next step.
This exercise will increase dorsiflexion and train the lower back to keep the arch in those with the longest femurs.
The third exercise for improving the back squat if you have long femurs involves the stability ball, BUT it’s not what you think. There is NO wall involved.

Use a ball that when you sit on it, your femurs are either parallel or below parallel.
If femurs are above parallel, use a smaller ball.
- Position feet as you would in a back squat.
- Arch lower back.
- Align shoulders vertically with midfoot.
- Make sure you’re dorsiflexed as much as possible (never force dorsiflexion; just achieve your natural limit).
You are now in position for a back squat; because the shoulder and midfoot are aligned, you should be able to push the ball aside and hold this position.
Do that and hold until fatigue sets in. Rest and repeat several more times.
Those with long femurs will find that these exercises will enhance your ancillaries: the assistive parts of your body in a back squat. They are the 1) lower back, 2) ankles, 3) hips and 4) shins.
Long femurs + ancillary training + wide stance and you have it made!
When doing these exercises, always wear athletic footwear, and do not force anything or over-train because the tissue around the ankle joint can easily be overstretched.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Long Femur, Short Shin: Advantage in Leg Extension, Ham Curl

Though a long femur relative to shin is a disadvantage in squats, it’s a biomechanical plus in the leg extension and hamstring curl.
The long femur to short shin proportion has been vilified as bad levers for the squat and deadlift.
But it’s vital to point out that these “bad levers” are actually a biomechanical advantage for the leg extension and hamstring curl.
Let’s Look First at the Leg Extension

Shins appear LONG relative to femurs. Shutterstock/lunamarina
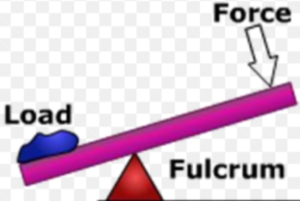
Many bodybuilders swear by this exercise for bringing out more sculpting in the quads. The fulcrum is the pivot point (in this case, the knee).
The resistance arm is the length between the knee and the foot where the foot is against the pad (weight application).
The force arm is the length between the knee and the hip.
The leg extension motion is similar to the classic example of a fulcrum and levers that we all learn in physics 101: the teeter totter, in which the fulcrum is represented as a triangle beneath the teeter totter.
On one end of the totter is a weight (the resistance). At the other end is the force (person pushing down on the board).
The closer the triangle (fulcrum) is to the weight, the easier it is to push down on the other end and lift the weight. Imagine the triangle very close to the weight.
That’s a very short resistance arm. Let’s say that the fulcrum is two feet from the weight, and the person at the other end is 15 feet from the fulcrum. He has an easy job.
Now move the triangle (fulcrum) so that it’s only two feet from the person and 15 feet from the weight.
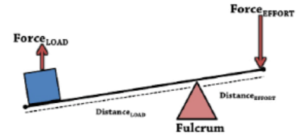
The force arm is now only two feet, and the resistance arm is 15 feet. It will be extremely difficult to push the board down and move the weight.
Apply these concepts to a person with a long femur and short shin, seated on a leg extension machine.
If the distance between knee (fulcrum) and hip is longer than the distance between knee and foot, this is akin to that triangle being closer to the weight.
In other words, think of the knee (fulcrum) as that triangle. Because the shin is short, the knee (triangle) is closer to the foot (weight application) than it is to the hip!
This becomes clearer when you imagine the athlete’s legs in full extension.
The knee is the fulcrum (triangle). If it’s closer to the weight application (foot) than it is to the hip (guy pushing down on teeter totter), it will be easier to move the weight!
Conversely, if the knee is closer to the hip (short femur, long shin), this is akin to the fulcrum (triangle) being closer to the guy pushing down on the board — making the work more difficult.
Imagine the profile of someone with a one foot femur and three foot shin sitting on the leg extension machine.
They begin extending their legs. That’s a LOT of shin bone that they must raise up, with that weight at the bottom (foot), and such a short force arm (short femur) to apply the effort.
Imagine a profile of someone with a super long femur and stumpy short shin. Gee, it’s pretty easy to get that shin parallel!
This same concept applies to the hamstring curl.

Shutterstock/Microgen
It will be harder for someone with short femurs and long shins to crank the weight towards their butt (short force arm) than it will for someone with a stretchy long femur and stubby short shin (short resistance arm).
So if you have long femurs and short shins, don’t despair over squat difficulties.
Do the best you can with the squat, but always include leg extensions and hamstring curls and see how much easier it is to move heavy loads than those with perfect squatting levers.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Flamingo Images

Being Tall Is No Excuse for Parallel Squat Problems!

Even a super tall NBA star could do an ass to grass squat if he has the right proportions!
Do not blame squat problems on being tall. Being tall, in and of itself, is not a disadvantage in performing a parallel or even deep back squat. The issue is not your overall height.
The issue is relative length of body segments!
It’s not an issue of getting long legs to bend under the body–UNLESS the torso is shorter than the femurs.
With “normal” proportions, those long legs will be under a proportionately long torso.
The proportionately long torso of the athlete will balance things out.
If you stand a 6-8 athlete next to a 5-8 athlete, who will have the longer legs? Obviously, the 6-8 person.
Now, who will have the longer torso? On average, the very tall athlete will have a much longer torso than the short guy.
Athletes do come in different proportions (anthropometrics), and these proportions influence efficacy of a particular weightlifting movement.
Ever see a champion in the deadlift who has T-rex arms?
Or how about a champion in the bench press with gorilla arms?
So what about the parallel squat? A tall individual can easily sink to parallel with an “upright” form as long as their femurs are shorter than their torso, and their shins are at least the length of their femurs.
Take notice of tall people’s femur to torso ratios. If you observe enough tall people, you’re bound to eventually spot some with “stubby” femurs.
They’ll have an easy time squatting (assuming they don’t have a history of back pain).
If distance from hip to knee is shorter than distance from clavicle to waist, they’ll have no problem back squatting.
Short stature is not necessarily an advantage in squatting.
It absolutely is not if one’s femurs are longer than their torso.
Remember, while a tall person has the long legs in the absolute sense, you must look at these legs within the context of the rest of their physique.
I’ve seen 6-4 men with gorilla builds and short people who were “all legs” and had the torsos of a person half a foot shorter.
Being very tall, in and of itself, “ain’t no excuse” for having trouble squatting.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik/freepic.diller

Can Femur to Shin Length Ratio Affect the Back Squat?

It isn’t just femur to torso ratio that can create problems with the back squat; shin length relative to upper leg can also mess things up.
You’re aware that if the femurs are longer than the torso, this will make the back squat difficult, sometimes very difficult, for an individual.
Let’s not dismiss the impact that shin length (tibia bone) can have on the squat, especially the back version.
Though I used to be a personal trainer and was keenly aware of body segment proportions of my clients, one need not be an exercise instructor to see some obvious points.
How does shin or tibia length influence the ability to sink to parallel in the back squat without excessive torso lean?
Certainly you know that to keep balance, one must keep the barbell over the ankle: a vertical point-to-point alignment.
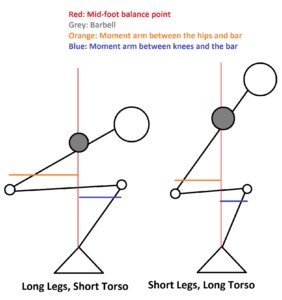
The longer one’s femurs are without the length of the torso changing, the farther their butt is from their knees, and the more bent their torso is (a smaller angle formed by femurs and torso).
To make it easy to understand how tibia or shin length can play a role, look at the illustration below.
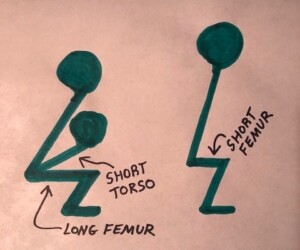
It’s hard to imagine the stick figure on the right falling backwards with all that tibia supporting him like a pedestal. Now, shrink the tibia to a centimeter. What happens?
Look at the figure on the left. That short (relatively) tibia has a lot of body to support.
The longer one’s shin bone, the easier it is to get the foot vertically aligned with the shoulder without having to pitch the torso way forward.
This isn’t only about ankle flexibility.
An extra inch of tibia in a person, for whom nothing else changes, will place their ankles back by about an inch, and allow that person to subtract an inch off their forward lean.
An extra inch of tibia sets the foot back about one inch, assuming that all other proportions remain the same.
The following is an excerpt from the book, “Scrawny to Brawny; The Complete Guide to Building Muscle the Natural Way,” by Michael Mejia and John Berardi, PhD.:
A femur that’s longer than your torso can compromise your ability to squat and deadlift efficiently because it will cause you to lean forward excessively to reach the desired depth.
Of course, a femur and torso of near equal length combined with a shorter lower leg can sometimes pose similar problems, although this can often be effectively managed by improving flexibility around the ankle joint.
The “lower leg” of course refers to the tibia or shin. Improving ankle flexibility allows a person to shift the knees more forward, thereby shifting the barbell more overhead of the ankle.
If you’ve been struggling with the back squat, it may not be so much that you have “long femurs,” but rather, short shins.
Everything else looks in proportion, and then you get to your short tibias.
Moving the kneecaps up a few inches would make your body look more proportionate.
Long femurs do get a bad rap, but sometimes the tibia should get some of the blame.
Often, though, a person’s tibia is the same length as their femur, but their torso is shorter than their femur, making them struggle with the back squat.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/UfaBizPhoto
Source: enotalone.com/health/4855.html

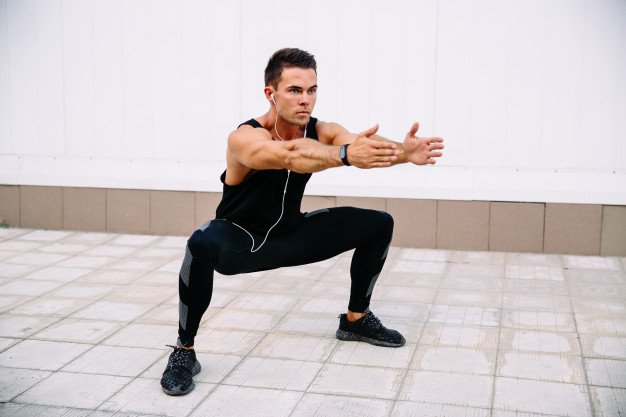
Why Elevated Heels Make Squatting to Parallel Easier

Anyone who’s struggled to get parallel in the squat (femur torso ratio) knows that elevating the heels makes this possible, and here’s why.
For those with long femurs and short torso who can’t achieve a parallel squat without leaning over like in a “good morning” position, elevating the heels (even a little bit) makes getting parallel possible.
If you’ve elevated your heels to get into a parallel squat (due to torso shorter than femur), perhaps you’ve also noticed that it seems as though more tension is on the knees and middle muscle of the thigh. You are not imagining this.
Why does elevating the heels make it possible to parallel squat in those with long femurs and short torsos?
In order to keep balance and prevent falling backwards while descending towards parallel, you must keep the shoulder aligned vertically with the midfoot.
One way to get the shoulder over the midfoot is to lean the torso forward.
Long femurs force the hips out further when lowering into a parallel squat, which means that the torso has more distance to lean forward to get the shoulders over the midfoot.

Those with long torsos don’t have as far to go as those with short torsos, assuming that relative femur length is identical for both people.
Sometimes the femurs are the bigger culprits, in that they are much longer than the shin bones.
The other way to get the shoulder aligned with the midfoot is to shift the knees forward while keeping the feet flat on the floor.
Shifting the knees forward will, in turn, shift the shoulders forward, while the feet stay fixed in one spot on the ground.
Your knees will shift forward (keeping heels on floor) only as far as the flexibility in your heel/foot will allow (a joint action called dorsiflexion).
If you go up on the balls of your feet, which elevates your heel, you can squat parallel and even all the way down while keeping a straight back.
- The elevated heel rotates the position of the feet forward, or “tips” them forward.
- This tipping automatically pushes the knees out more.
- Your shoulder is now easily aligned over your midfoot without having to lean the torso forward.
HOWEVER, you’ll also notice that when squatting on the balls of your feet, which produces a considerable ankle elevation, the knees may feel strained.
Squat all the way down (like a baseball catcher), then stand all the way up — on the balls of your feet. Feel that in the knees? And do you feel it in the middle quad muscle?
This is because the knees were way ahead of the feet, which is a poor way to perform a barbell or even goblet squat.
Now, imagine placing the heels on a one-inch-high board, a few small weight plates to elevate them, or elevating the heels by wearing a heeled shoe.
You can now more comfortably squat parallel despite the long femurs and short torso.
Again, the elevation “tips” the foot forward, which automatically drives the knees out further in front.
This forward shift causes the shoulders to forward shift, bringing them in alignment with the midfoot.
Unfortunately, as just pointed out, this forward shift puts more tension on the knees and subtracts tension from the glutes and hamstrings.
Nevertheless, the slight heel elevation is a sensible option for those with long femurs and a short torso who struggle to parallel squat.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/coka

Does Sitting, Rising from Chair Mean You Can Parallel Squat?

I could not believe it when a strength training enthusiast chastised another about the parallel squat, in that the one trainee insisted he was not able to squat due to a short torso (and long femurs).
The critical person said, “If you can get up and down from a chair and toilet, you can do a parallel squat, so stop making excuses!”
People with short torsos and long femurs can get into a parallel squat. Few people will deny this.
However, the position your body takes, when sitting onto a toilet and then rising, is not the recommended or same position that one should perform a barbell squat with!
Using a toilet involves crouching forward, supporting oneself with the forearms on the thighs! Who sits upright, arms off thighs, with a lower back arch while on a toilet?
And what fitness expert or even experienced trainee would recommend barbell squatting with a crouched forward torso?
The crouched forward torso makes it easy as pie to rise from a toilet!
As for lowering and rising from a chair, this comparison to the parallel squat is deeply flawed because the chair prevents a person from falling backwards onto the floor!
Who squats parallel with a barbell or even bodyweight only, with their legs, feet and back positioned as they are when getting into and out of a standard chair?
Last time I checked, not a single human being on this planet. It is physically impossible.
Getting into and out of a chair does not require the ankle dorsiflexion that a parallel squat does.
The chair provides external support, too. In a parallel squat for exercise, nothing supports the trainee!
Of Short Torsos and Long Femurs…
Though a chair is an excellent training tool for developing a parallel squat for those with short torsos and long femurs, getting into and out of a chair in daily life is an extremely poor analogy to the parallel squat!
Those with short torsos and long femurs can hover over a chair and practice the lower back arch and minimizing the forward torso lean, and experiment with dorsiflexion while viewing their profile in a mirror.
To say that getting into and out of a chair or onto and off a toilet means that you can parallel squat, means that your 87-year-old Grandma can parallel squat because she can lower and rise from a dining room chair and get onto and off a toilet without assistance!
Can you picture Grandma squatting to parallel without holding onto anything, let alone with a barbell across her back?
The muscular forces and leverages that a parallel squat requires are NOT required to lower into a chair and then stand up from it.
This is why when a person lowers into a chair and a sneaky person pulls the chair out from under them, they fall flat on their can instead of remaining suspended in the air in a parallel squat position, even when they know what just happened!
I said earlier that those with short torsos and long femurs can get into a parallel squat.
BUT — the problem is, if their femur, shin bone and torso ratios are disadvantaged enough, they will need to execute a severe forward torso lean, making the lower back arch impossible.
Their back is rounded, chest smack on top of their thighs (think of a closed clam shell or a speed skater cruising in a distance race).
Often, to hold even THIS position, those with short torsos and long femurs must have their arms straight out in front of them.
So how is it possible for these trainees to execute a parallel squat with their back erect enough to support a barbell without rounding their back?
Those with short torsos and long femurs can have all the ankle, hip and low back flexibility in the world, and still find it impossible to avoid the rounded, slumped-over back while going parallel.
Their only recourse is to Sumo their stance or elevate their heels, best done with shoe lifts, which are significantly cheaper than weightlifting shoes.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: brusblaus/CC
Yes, TALL People CAN Have Short Femurs

Super tall men with relatively short femurs have a squat advantage over shorties with relatively long femurs ANY DAY.
Many believe that being tall interferes with doing a parallel squat because, allegedly, it’s troublesome to get long legs bent under one’s upper body.
But with long legs comes a longer trunk (because in tall people, everything is longer) to help offset the tendency to “fall backwards” while doing a squat.
A typical 6-4 man has a longer torso than a typical 5-4 man.
If someone stands 5-10 and has legs as long as the average 6-4 person, there will be a big problem with squatting parallel, because the torso for this person is too short to offset femur length.
Likewise, take those same legs; put them on someone with a torso long enough to put them at 6-8, and we now have a nice combination for the parallel squat … unless the femurs are super-crazy long in relation to the shin length.
Tall people can have short femurs.
How is it that in strongman competitions these very tall guys are squatting thunderous amounts of weight?
Look at their femurs! Their thigh bones are NOT relatively long (compared to shin length). Many appear rather “stubby.”
Another venue where short femurs on tall people are evident is in the world of runway modeling and in the models in glamour magazines.
Models are tall, many being 5-10 and 5-11. Google leg images for your favorite tall movie star and look at her femurs; some will be relatively short.
Tall People and the Parallel Squat
So when I hear tall people announcing, “I can’t squat parallel because I’m tall,” I really wonder.
The proportions in this illustration can be seen in tall men. Look around at your gym. I’ve seen tall men with femur lengths almost half their torso. Freepik.com/kjpargeter
The parallel squat can be very difficult for a SHORT person with relatively long femurs to shin ratio (or to torso length).
The body build that is often not built for squatting is that of the elite marathon runner.
They rarely have relatively short femurs and often have high waists (short torsos), which helps reduce drag when running.
The long femur and short torso duo is a wicked combination for parallel back squats. A 5-2 person can have this anthropometry.
A very tall person can have short femurs (relative to shin length and/or torso length), making them well-built for the parallel squat.
An important point is that many competitive Olympic-style weightlifters, who do well in competition, are tall.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/SeaRick1

Do Long Femurs and a Bad Squat Mean You’re Weak?

If you’re biomechanically disadvantaged due to femurs that are longer than your torso, find out if this means you’re weak.
When a person with long femurs (meaning, femurs longer than their torso, regardless of overall body height) tries the back squat for the first time, even with just body weight, they immediately realize there’s a problem.
If you clicked on this article, then you already know what the issue is with long femurs and the squat.
You also certainly have come across the term “biomechanical disadvantage,” and perhaps have read quite a bit of content in fitness forums saying that those with long femurs and a short torso can injure themselves doing heavy back squats, and even that they should avoid this exercise altogether.
In short (no pun intended), it’s almost as though having long femurs and a short torso is a disability that makes people weak.
In the truest sense of the meaning of “weak,” a person with this anthropometry is NOT weak. They can be very strong.
The issue isn’t strength per se. It’s body position.
Let’s take a really strong beast of a person as an example, say, an Olympic heavyweight weightlifter. Now, let’s lie him on his back.
Though this is an extreme example, its extremeness will clearly illustrate why the person with the long femurs and short torso is not weak, but instead, it’s an issue of body position — a body position that he or she cannot access.
So we have this very strong person lying on the ground on his back. Beside him on the ground is a 50 pound kettlebell that he can reach only by straightening his arm.
His job is to lift the weight off the ground — while maintaining his position of back lying on the ground.
This means he must grab the weight with a straight arm, and because his back must stay on the ground, he cannot bend his arm.
Though he has brute strength (remember, he’s on the Olympic weightlifting team), he will not be able to lift the kettlebell.
Does this mean he’s weak?
Or does it mean he’s at a biomechanical disadvantage due to body positioning?
Because he’s not able to get into an efficient lifting position, he is not able to move the weight. It’s a matter of body position, not lack of muscle strength.
Again, this example is extreme, but you can apply a scaled-down version of this principle to the individual with the long femurs and short torso.
They are simply not able to get into an upright squat position, and thus, are not able to utilize the strongest muscles of their body to squat heavy weight.
Instead, their lower back muscles (which are not force production muscles by nature) are made to take some of the weight.
The deeper this person gets into the squat, the more he must lean forward to keep from falling backwards.
Somehow, someway, famed powerlifter Lane Norton pulls this off with a ton of weight, despite having “bad levers” — femurs long relative to torso length:

If this forward lean is severe enough, it becomes impossible for most people to maintain an arch in the lower back, and the back rounds, creating the potential for disaster.
The person ends up “lifting with their back” instead of “lifting with their legs.”
This is a very inefficient way to lift heavy weight, but it occurs due to the long femur short torso person being unable to get into the position of upright back while squatting (they are leaned way over). Literally, their long femurs get in the way of the lift.
Now take a look at the femur to torso ratio of the man below. His squat is almost as deep as Norton’s, but check out his ridiculously upright back!

The biomechanical rather than strength issue isn’t just present when trying to squat with a barbell across the upper back.
The long femurs get in the way when picking something heavy off the ground as well (you name it: big potted plant, crate of books, file cabinet, big sick dog).
The individual with this anthropometry has two choices: 1) Squat half-way but lean far over (risking low back injury) to get their hands between the object and the ground, or
2) Squat nearly all the way to keep their back upright while holding onto the object to prevent falling backwards, and while in this position, lifting the object.
The problem with #2, even though the back is upright, is that the heavy lift begins from a deep squat, which is harder than a heavy lift from a half-way squat.
A person whose femurs are shorter than their torso can maintain an upright back as they descend into the squat, and thus can begin lifting the heavy object when they’ve reached half-squat depth — less range of motion to do the lift!
So you see, long femurs and a short torso do not make a person weak; they just prevent that person from getting into the most efficient body position to perform a lift.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}