

How to Strengthen Your Wrists

You can have strong wrists and still sprain them, but stronger wrists are less likely to be severely sprained. Here’s how to make your wrists stronger.
Plus, a strong wrist will recover better from a sprain.
Here’s something you should know: There is no such thing as strengthening only the wrist.
To strengthen this joint area, you must work the forearms.
This can be done in a variety of ways.
Anyone, even “out of shape” people, can benefit from the following exercises.
How to Strengthen the Forearms
Wrist rolls with a dumbbell. Sit at the edge of a bench, light dumbbell in hand, palm facing ceiling.

Shutterstock/Philip Date
Let the dumbbell roll toward your fingertips, then bring it back to the palms. Keep doing this till you can’t any longer.
If this is too difficult, or, another option, is to keep the dumbbell fixed in place, and simply bend your wrist up and down.
How much weight to use will very from one person to the next.
Reverse hand position and bend the wrist up and down while holding the weight.
Another option is wrist rolls with a bar.

Farmer’s walks. Walk around for three minutes holding dumbbells with your arms straight at your sides.
Men can start out with 20 pound dumbbells, while women can start out with 10 pounders. The prolonged hold on the weights will strengthen the forearms and wrists.
If after about three minutes you don’t feel much fatigue in your wrists, then use heavier weight next time. The weights can also be plates or kettlebells.

If you do sprain your wrist, a wrist brace (as shown below) will help it heal.

Shutterstock/belushi
My first sprain (from volleyball) healed quickly. My second one (volleyball), which was worse, was not healing despite icing and immobilization from a brace.
It really hurt at the slightest rotary motion, as in proceeding to turn on the ignition of my car. I had to do that with my left hand.
I went to a doctor and she told me that the problem was that I wasn’t moving it. Yes…that I WASN’T.
It was time to end the complete immobilization and gradually work back into moving the joint.
I moved it to the left several times, then the right several times.
Up several times, then down several times … several sessions like this throughout the day.
Voila, the first day I noticed a marked improvement. Within several days my wrist was practically back to normal.
Additional exercises for strengthening your wrist include the deadlift, any pulling movements such as with weight machines in which you pull the handles towards your chest, and using hand grips.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Orawan Pattarawimonchai

Hip Replacement Surgery: Obesity in Women Hampers Recovery

Not only is there nothing positive about a body that falls prey to hip disease due to obesity, but very plus-size women who undergo hip replacement surgery fare worse than do overweight men.
A very large woman can have normal blood pressure, normal blood sugar and a normal EKG — but this doesn’t change a FACT:
Hip replacement surgery is more common in the obese population, because very heavy women and men are more likely to suffer from hip osteoarthritis (wearing away or degeneration of the cartilage in the hip’s ball and socket structure).
Being body positive and boasting “great blood work” won’t protect you from this common disorder of the hip joint.
Despite what the “health at any size” movement insists, obesity is a major hardship on the body and causes more complications after surgeries than in leaner patients, and hip replacement is no exception to this rule.
However, just how obesity affects the outcome or results of hip replacement surgery in women, is not the same as in men, says research from Geneva University Hospital in Geneva, Switzerland.
The study involved 2,495 hip replacements over a 10-year period, of which 589 were on obese patients.
The following elements were evaluated: dislocation, infection, redoing the surgery, satisfaction with the surgery, quality of life and general health.
Most of the plus-size patients were men, but for the heavy women, obesity was tied to a much greater risk for infection, and it brought on more dislocations than in the men, resulting in surgical revisions.
Obesity in Women vs. Men: What They Reported
- The women reported medium-level lower functional outcomes, but the men didn’t report any.
- The women also reported a little less satisfaction, and most of this came from the higher rate of complications.
In short, the obese women had poorer results from their hip replacements, but strangely, the risk factors for infection that more often strike heavy patients, did not apply to the women in the study.
The researchers aren’t sure what could explain this, but suggest possibly it could be differences in body fat distribution between the genders, and maybe even metabolic response.
As a former personal trainer I speculated that lower levels of muscular strength could explain it, and sure enough, further into the study report, it stated that another theory was “lower peripheral muscle strength” in the women.
Many body positive women claim on Instagram that “fat means strong,” or “fat people are strong,” etc. Even thinner people have been known to state, “Fat people have to be strong in order to move around all their weight.”
But often, when a very plus-size person is moving around for the normal activities of daily living…they are sweating, breathing heavily, and you can hear the effort in their voices. Yes, they’re moving the weight, but it’s not comfortable.
Thus far, nothing is set in stone, and the researchers point out that prior studies of hip replacement, obesity and complications cough up conflicting results, especially since “obesity” can have varying definitions.
For women (and men) who are considering hip replacement surgery, weight loss is crucial.
- Emphasize upper body strength training since a painful hip joint will limit aerobic activity.
- Focus on big compound moves like barbell pressing, dumbbell pressing, and machines that target the chest, shoulders and back.
- Add water aerobic classes for a little extra calorie burn, but these should NOT replace strength training with weights.
The full report is in Arthritis Care & Research (March 2007).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Jazz Guy from New Jersey/commons.wikimedia.org
Source: sciencedaily.com/releases/2007/02/070228064707.htm

Can Young People Get Bursitis? Best Treatments

Bursitis doesn’t just strike old people; the young can get it too.
Bursa are the small sacs of fluid that help muscles slide easily over other muscles and bones.
Bursitis is when the bursa become inflamed, as a result of either overuse during sports or workouts, tasks around the house, or from running or jogging.
The pain often comes on within a few days of the offending activity.
The pain of bursitis can feel like the pain of tendonitis. An orthopedic specialist can make the right diagnosis.
Risk Factors for Bursitis
“Any overuse activities might cause tendonitis,” says Michael A. Schwartz, MD, an orthopedic surgeon with White Plains Hospital Physician Associates in NY.
“Also, any excessive leaning on certain body parts: most commonly on the knee or elbow.”
Prolonged leaning motions are commonly seen in gardening (knees), and reading a newspaper (elbows on the table).
Excessive elbow-leaning also occurs in some people who spend a lot of time at a computer. So you can see now how young adults can develop bursitis.
What sports or types of exercises can cause bursitis?
Dr. Schwartz says that many can lead to bursitis, “especially those that involve repetitive motions, such as tennis, golf, throwing sports, etc.”
Is bursitis curable? Or must the sufferer live with it permanently?
It’s curable.
Can supplements help?
Dr. Schwartz says there is “no data on supplements or certain foods that can help this. It is usually treated with activity modification and anti-inflammatory medicine.”
Home Treatment
Avoid the activity that caused the bursitis. The pain may go away in a few days to a few weeks. But don’t assume the problem is gone just because the pain is gone.
Merely resuming activity after staying away from it, is not enough to regain pre-injury status. You must strengthen and stretch the muscles around the injured joint.
You may also need to change the way you perform a strength-training routine that caused the bursitis.
For example, sometimes the entry and exit into a routine with dumbbells can add stress to the joints.

Often, people quickly lower the weights, and their arms just flop down with them, rather than a deliberate, controlled lowering. Sudden, abrupt movements can cause or prevent the healing of bursitis.
Another way of modifying the routine is to switch type of weights. For example, if using a barbell caused the injury, switch to dumbbells.
If flat-bench dumbbell presses caused it, then use an incline bench, and lighten the weights accordingly.

Ice. When there is pain, apply an ice pack for 10 minutes, once and hour for up to three days.
If pain persists, apply the ice for 15-20 minutes, but never more; and three times daily.
Though heat application may feel nice, remember that only ice will relieve inflammation and speed up healing.
It’s unlikely that bursitis pain will ever reach unbearable levels; thus, taking drugs only to numb the pain is not necessary.
In fact, masking the pain this way can lead to a false sense of healing, causing you to over-use the joint while it is still actually inflamed or injured.
Feeling the pain allows you to know where your limits are, as far as range of motion and exertion.
On the other hand, an anti-inflammatory can bring down inflammation, but keep in mind that inflammation can go away via a natural approach: avoiding the offending activity, applying ice, and the following guidelines.
When you’re not in pain, gently move the joint through full range of motion several times daily, to prevent stiffness.
A joint that becomes stiff from under-use, adds more pain to the problem and slows healing. In other words, total rest is a bad idea if you have bursitis.
You can gradually resume the offending activity, but start out with much lower weight — or in the case of a sport such as golf, a gentler approach. If it still hurts, use no weight, and just go through the motions.
For instance, if bench pressing caused the injury, you may need to initially just lie down and do pressing motions against the air, to reintroduce your injured joint to the act of bench pressing.
For golf or baseball, just go through the motions of swinging and throwing.
Make sure you strength-train to prepare your joint for eventual full-participation in your sport, and to help prevent a recurrence of bursitis.
If the problem was caused by excessive leaning on joints, then stop leaning on your joints.
Prevention of Bursitis
Always warm up prior to sports or workouts.
This means stretching the joint to be exercised, and gradually working up to high intensity if this is part of your regimen.
For example, do several sets of light bench presses, and a few medium sets, before piling on the weights. Stretch when you are done.
If you begin to feel any kind of pain starting, even if it’s a dull ache, immediately stop. Do not try to work through bursitis.
 Dr. Schwartz has previously worked as a team physician for high school, college and professional sports, and is the author of numerous scholarly research articles and chapters in orthopedic surgical textbooks.
Dr. Schwartz has previously worked as a team physician for high school, college and professional sports, and is the author of numerous scholarly research articles and chapters in orthopedic surgical textbooks.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/goodluz

Single Best Exercise for Curing Low Back Pain that’s Benign

If there’s only one exercise you could do to cure low back pain, I have it.
There is one exercise for curing low back pain that stands out way beyond the rest.
I had recommended it for my clients during my days as a personal trainer at a health club — and got very positive feedback from them.
It’s a powerhouse of an exercise, superior to other typical exercises that are prescribed for treating low back pain. It is the deadlift.
Maybe you’ve never heard of the deadlift. And if you have, you may still not know what this is, or may have a misguided perception of this exercise. But dang, it cured my low back discomfort.
I’ve been lifting weights since my teen years, but never did deadlifts. I hated them.
But there came a point in my life where I realized that my low back would be aching if I got up from a chair after sitting for awhile. Where the devil was this coming from?
Too much time at the computer? Heaven forbid if the discomfort was because I wasn’t 19 anymore, or perhaps I had inherited a predisposition for this annoying problem from my father.
I had already been doing intense back training routines at the gym, but these primarily targeted the middle and upper back muscles.
I did some low region work, however, and decided to up the ante, adding back extensions and more “camel backs” to my regimen.
But that didn’t make a difference. I still experienced the daily discomfort. So I asked myself, “What’s one exercise for the low back that I haven’t been doing? Deadlifts!”

Setting up to do a deadlift. Freepik.com

Completed deadlift.
I decided to give this compound move a try, no matter how much I hated it, and to stick it out for a fair length of time.
I did deadlifts three times a week: 1) With a barbell, 2) With dumbbells, and 3) Holding weight plates.
Within eight weeks, the pain in my low back, or achiness, what-have-you, was gone. Gone. Entirely gone. Vanished.
This was not something that would have disappeared on its own, because I had had it for quite some time, and had tried other workout routines to combat it, with absolutely no improvement.
And then suddenly, once I begin doing the deadlifts, there is steady improvement, so the logical conclusion is that this compound exercise cured my low back discomfort.
Medical Disclaimer
I never saw a doctor for my problem, and I don’t recommend that you start a deadlift program unless a physician clears you of having any spinal issue that would contraindicate this type of exercise.
In my case, I’d had no injury, no car accident, no fall, no tingling or numbness, no pain radiating to my butt or leg.
I apparently had a soft-tissue deconditioning and stiffness that occurred over time (despite my years of athletics and weightlifting), and the deadlifts restored everything.
I’ve continued to do deadlifts (along with other major core exercises), and my low back is now bullet-proof.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik/yanalya

Can Torn Rotator Cuff Be Remedied With Exercise Therapy Alone?

Diagnosed with a torn rotator cuff?
Have you been told that the only solution for torn rotator cuff is surgery?
When the rotator cuff is “torn,” this means that some tendon tissue has been separated, or pulled away from, the bone to which it’s supposed to be attached. Tendons join muscles to bone.
“The shoulder is a ball and socket joint,” says Edmond Cleeman, MD, a board certified orthopedic surgeon who specializes in sports medicine and arthroscopic surgery of the shoulder, knee and hip.
“There are four tendons that move the shoulder and they are called the rotator cuff tendons.
“Covering the entire rotator cuff is a bursa, a paper-thin fluid sac that helps gliding occur with less friction between surfaces.”
Does a torn rotator cuff automatically mean surgery?
“Rotator cuff tendon tears do not heal on their own and this has been verified with scientific study.
The tendon is attached to bone and when it tears it is pulled away from the insertion site by the muscle, like a rubber band snapping back.
“The only way for the tendon to heal is to pull it back to the bone insertion site and sew it to the bone.
“This procedure is customarily performed arthroscopically (minimal invasive surgery), with a regional anesthetic (the arm is numbed), and the patient goes home the same day.
“Success rates are high in small tears but success diminishes with increasing tear size.”
Rotator cuff problems are extremely common, and not just in athletes who do a lot of throwing or overhead movements.
People who don’t exercise are also vulnerable to rotator cuff injuries, particularly degeneration.
“Scientific study has demonstrated that rotator cuff tendon tears, if left unfixed, will increase in size,” says Dr. Cleeman, founding member of TRIARQ, a community of orthopedists and physical therapists.
“Eventually the tear will become large or massive and the results for surgical repair will diminish. Some tears will no longer be fixable.
“This is because the muscle attached to the torn tendon atrophies, contracts and essentially melts away.”
If the tear is partial or very small, this might be treatable without surgery; physical therapy would be the cornerstone of healing.
“But in these scenarios vigilant watch over the rotator cuff tendon tear with repeat MRI is a must. If the tear starts expanding then surgical repair is recommended.”
If the rotator cuff tear becomes too big, surgical repair may not be possible.
“The results after surgery for massive tears is significantly lower than small tears.
“The likelihood of being able to repair this tear is low because of the atrophy changes in the muscle and tendon.
“Non-surgical treatment starts by avoiding activities that cause pain and aggravate the rotator cuff tendons. These are mostly strength activities with the arm over shoulder height.”
 Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/KDdesignphoto

Best Exercises for Older Knee Replacement Patients

If you’re 65 years or older and have had total knee replacement surgery, you’ll need to know what the best exercises are for recuperation as well as maintenance.
For older people, as well as younger, having knee replacement surgery, there are exercises they should do for the rest of their life, to maintain optimal functioning of the knee replacement.
There are range of motion exercises, as well as strength-building exercises.
For range of motion exercises, “place a towel under ankle and this allows for a passive stretch” for knee extension,” says Edmond Cleeman, MD, a board certified orthopedic surgeon who specializes in sports medicine and arthroscopic surgery of the shoulder, knee and hip.
This can be done lying down. Place the towel under the foot, holding equal parts of the towel in each hand, and gently pull your straight leg towards you while lying.
It’s okay if the leg is a little bent; not everyone is flexible enough to keep their leg straight.
Another stretching exercise for the knee replacement patient is “Flexion: sit in a chair with foot supported on the floor. Patient actively bends knee,” says Dr. Cleeman.
“You are quickly trained to transfer (i.e., lying to sitting, sitting to standing), then progress to gait training (with assistive device), stair training, and eventually work up to the stationary bike.”
The knee replacement patient will also need to work on quadriceps (front thigh muscles) strength by doing straight leg raises from a standing or lying position, one leg at a time.
On a continued basis, the knee replacement patient should do low impact activities like “walking, swimming and cycling,” says Dr. Cleeman.
Strengthening the quadriceps is especially important for knee replacement patients, particularly older ones, because this muscle group controls knee extension.
Quadriceps strengthening will ease pain, says Dr. Cleeman. Knee replacement surgery takes a while to recover from, especially if you’re older.
Strengthening the quadriceps is invaluable because it will make living so much easier, i.e., exiting chairs and cars, climbing stairs, etc..
Examples of Quadriceps Strengthening Exercises
Squats. These can be done by holding a stable support, such as the knobs on either side of an open door, and simply squatting up and down, or squatting while both hands are placed on a wall.

Or, says Dr. Cleeman, “Practice rising from a chair start with several cushions, then remove one at a time.” Work up to 20 repetitions.
Leg presses. This requires gym equipment. Keep feet flat on the pushing platform and don’t let legs bend more than 90 degrees. Work up to 20 repetitions.

Shutterstock/wavebreakmedia
Knee replacement patients, especially older ones, will benefit from a personal trainer once they are finished with all of the post-surgical rehabilitation exercises that were prescribed for them.
Sometimes the surgeon will prescribe specific exercises, and other exercises will be performed through special physical therapy.
Once these programs are concluded, the patient can then upgrade by hiring a personal trainer.
If money is tight, consider this format for just a few sessions. Recreation centers provide personal training at reasonable costs.
Whatever you decide, having knee replacement surgery means a lifelong commitment to home exercises to keep the knee functioning optimally.
Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasirin pamai
Sources: triarq.com

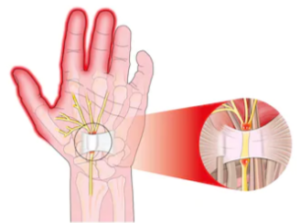
10 Minute Carpal Tunnel Release: No Stitches, Fast Recovery

Traditional carpal tunnel release requires up to three months of recovery, leaves scars and requires restrictive bandages up to two weeks following surgery.
However, there is a shorter, less invasive carpal tunnel release surgery that takes only 10 minutes, called stitchless endoscopic carpal tunnel release.
The incision is 1 centimeter and results in minimal scarring. A local anesthetic is used and there are no bandages necessary.
Stitchless endoscopic carpal tunnel release offers no restrictions after 48 hours and a recovery time of just one week. Stitchless endoscopic carpal tunnel release results in much less pain than the traditional “open” surgery.
Dr. John T. Knight, MD, an L.A.-based hand and wrist orthopedic surgeon and director of the Hand and Wrist Institute at the D.I.S.C. Sports and Spine Center, performs the stitchless endoscopic carpal tunnel release. I asked him some questions.
Why isn’t the stitchless endoscopic carpal tunnel release more well-known?
This technique has been around since the ’90’s but has become much more sophisticated.
When I first went into practice in the early ’90’s I treated quite a few patients with complications from other doctors that took a weekend course and were not hand specialists.
Once the equipment has become much more refined I began doing the procedure in the recent past. I have had excellent results and a much quicker recovery than the older open procedure.
There at two common techniques: one vs. two incisions. I use the single incision which minimizes scarring.
Can you comment on infection risk with stitchless endoscopic carpal tunnel release, vs. the traditional open carpal tunnel release?
I have never had an infection with either procedure, but usually the less invasive, the less infection, as the larger wounds are exposed to the air longer.
With any procedure, no matter how minor, there is always a risk of infection.
Outpatient surgery centers, like the one at D.I.S.C. Sports and Spine Center, have lower incidences of infection than a hospital, even if done in an outpatient setting.
We take extra precautions to ensure against infection, and is vitally important that any facility adhere to strict guidelines of hygiene and cleanliness to reduce the risk whenever possible.
Why don’t more surgeons utilize the stitchless endoscopy method for carpal tunnel release?
Most surgeons are creatures of habit and if they have had pretty good results with the open procedure, then they are unlikely to want to try a new technique.
Many surgeons find it difficult to learn endoscopic procedures, as it requires an ability to work with longer and smaller instruments at a distance from the structure to be repaired, or released in this case.
Are there any contraindications to the stitchless endoscopic carpal tunnel release, that would require the patient to undergo the open method?
If a patient has had a previous open release with recurrence, significant inflammatory disease such as rheumatoid arthritis, a tumor, or incomplete visualization doing it endoscopically.
Is the “local” anesthetic literally local to the hand/forearm, or is it actually a nerve block for the entire arm?
Usually we give a local injection in the palm and wrist along with intravenous sedation.
This allows for a quicker recovery for the patient, who can then begin mobilization of the hand and wrist within an hour or two of the procedure.
It is not uncommon for the patient to be able to hold a glass of liquid within a relatively short time span.
When they are discharged a few hours after the procedure, the only real restriction is to avoid any lifting or intense movement for a few days, but light activities are fine within a few days.
While pain medication is prescribed upon discharge usually very little is taken, as many patients manage their pain with over-the-counter medication like Advil during the initial healing process.
If you have been diagnosed with carpal tunnel syndrome, it would be very wise to consider the stitchless carpal tunnel release when conservative methods of treatment have failed.
 Dr. Knight is widely regarded as one of the most prominent hand and wrist specialists in the U.S., specializing in minimally invasive techniques for hand, wrist and upper extremity injuries and disorders.
Dr. Knight is widely regarded as one of the most prominent hand and wrist specialists in the U.S., specializing in minimally invasive techniques for hand, wrist and upper extremity injuries and disorders.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/jcomp

What Exercises Relieve Carpal Tunnel Surgery Pain?

After carpel tunnel syndrome surgery, it’s possible to experience lingering or residual pain that might shoot up the entire arm and affect the shoulder.
Remember, the carpal tunnel compression has caused irritation to the median nerve, which runs the length of the arm (beginning from hand) all the way up to the shoulder and neck where it comes out from the spinal cord.
Pain from carpal tunnel syndrome doesn’t always disappear 100 percent immediately after surgery.
The median nerve may still be irritated, and this can cause pain or discomfort even several days after carpal tunnel surgery, including pain in the shoulder. My mother had carpal tunnel surgery on both hands at the same time.
She was experiencing pain from carpal tunnel in the shoulder before surgery, and post-surgery for several days, and sometimes it ran down the length of the arm.
Based on my experience working with my mother; plus my experience as a certified personal trainer working with clients who had various body tweaks; and my own experience with sports injuries over the years, I had my mother do some specific exercises to relieve the post-surgical carpal tunnel pain.
The surgeon told her that this post-surgical carpal tunnel shoulder pain was “par for the course” and that it would eventually disappear.
However, in the meantime, it’s not pretty. A person with this problem will typically intuitively remain immobile and ride the pain out, perhaps taking “pain pills,” namely, whatever their surgeon prescribed for them for post-surgical carpal tunnel pain.
The combo of narcotics and inertia didn’t work for my mother, and quite frankly, I don’t see how they can work for anybody’s post-surgical carpal tunnel pain.
The drugs caused other undesirable side effects, and inertia “unteaches” the body to be efficient at movement.
Stand with feet shoulder width apart.
Raise both arms straight up, as though to shake someone’s hand. Keep them nearly straight. Raise them parallel to floor.
If this hurts, raise to just below the threshold of pain. If you can go past parallel, do so. Lower. Repeat for total of 12 times.
Continuing to stand, keep both arms straight at sides, palms facing body.
Rotate palms outward so that they’re facing forward, then rotate them so that they’re facing behind you.
This action will open and close the shoulder joint as well as rotate entire arm. Repeat both directions 12 times.
Bend over, one hand resting on countertop or table for support.
Let other arm dangle. Rotate shoulder in circles, forward 12 times, then backwards 12 times, letting arm hang relaxed. Don’t bend arm. Repeat other side.
Place two coins on kitchen countertop about a foot apart.
Place hands before either coin. Now, cross forearms over each other so that opposite hands are now aligned with each coin. Return to start position. Repeat 12 times.
Standing, move arms as they would as if running in slow motion.
Exaggerate the arm movement so that shoulders get a good rotary and vertical workout. Do this for 30-60 seconds.
By this point, the shoulder pain should be mostly dissipated. If it isn’t, then perhaps you can design some different exercises.
I also recommend follow-up visits with the doctor who performed the carpal tunnel surgery.
Inertia in absence of structured exercise isn’t the answer; it will only further stiffen up the joint and reduce blood circulation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Shutterstock/WSW1985

Carpal Tunnel Syndrome: Why Post-Surgical Bandages Are So Thick

If you have carpal tunnel syndrome and planning on having the traditional, “open” surgical technique, you’ll be required to wear thick bandages that cover the carpal area of your hand for up to a few weeks following surgery.
The carpal area of the hand encompasses the wrist all the way up to the knuckles.
Your fingers will be free to move and bend, but the palmar and back of your hand will be bound in a thick wrapping of bandages.
My mother had carpal tunnel syndrome release surgery, the open technique, on both hands at the same time, and wearing the heavy bandages was no picnic.
She wondered why the wrappings had to be so constricting for such a seemingly small incision.
The purpose of the thick bandages following carpal tunnel surgery was to provide immobilization to the wrist.
Post-surgical swelling is another reason for the layers of bandages, since carpal tunnel release involves the cutting of a band of tissue that goes across the median nerve.
After 10 days, my mother had the bandages removed. They were cut away with a pair of shears by the surgeon’s nurse, and revealed incisions, with stitches, that appeared to be about an inch and a fourth in length.
The nurse then removed the stitches; a painless procedure. At that point, my mother was good to go, with no restrictions with the use of her hands as far as getting them wet.
When the bandages were on, she was instructed not to get any water on the wrappings.
Symptoms of carpal tunnel syndrome:
- tingling, numbness and/or weakness in all the fingers except the pink
- reduced grip strength of the hand
- reduced pincer strength of the fingers
- inability to make a complete fist
- aches or pains in the hand; pain upon flexing the wrist (bending the palm so that it’s closer to the underside of the forearm)
- and pain upon tapping the area of the palm just above the wrist.
Symptoms of carpal tunnel syndrome can also include pain in the forearms and even shoulder, even though the compression site of the median nerve is at the wrist.
This nerve goes all the way up the arm, into the shoulder and runs into the spinal cord at the neck, and the entire nerve can become irritated.
If you decide to have carpal tunnel “open” surgery, expect to wear thick bandages for 10-14 days afterwards.
There is another type of surgery for this nerve entrapment disorder that eliminates the need for bandages afterwards: stitchless endoscopic carpal tunnel release.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Angkana Sae-Yang

Hand Exercises After Carpal Tunnel Surgery to Regain Strength in Senior Citizens
After my mother had carpal tunnel syndrome surgery on both hands, she was left with weakness in both hands; weak fingers and a weak grip.
This is because the carpal tunnel syndrome progressed from mild to severe in only a matter of several weeks.
As a result of carpal tunnel syndrome’s effect on the median nerve, she lost some use of her hands and fingers.
This meant that some muscles weren’t getting used for several weeks. When muscles don’t get used, they shrink or atrophy (become atrophied).
An atrophied muscle is a weakened muscle, and often very stiff due to dis-use.
The fingers have muscles, and just because they are naturally small, doesn’t mean they can’t atrophy and weaken when not used, and carpal tunnel syndrome at its worst will definitely cause muscle weakness in the fingers.
My mother’s EMG test did not detect muscle weakness (EMGs measure nerve conductivity), and the doctor said there was no sign of muscle atrophy.
However, the weakness was there for sure, and remained there even after the carpal tunnel surgery.
To combat this lingering weakness, I designed some exercises for my mother.
Post-surgical exercise for carpal tunnel release #1
The first obvious exercise for strengthening the fingers and grip following carpal tunnel surgery is to simply open and close the fist well past the point of fatigue. Each close should be as tight as possible.

Post-surgical exercise for carpal tunnel release #2
Roll out a section of toilet paper about 5-7 feet long. With just the carpal tunnel hand, hold one end of the paper, then start scrunching it up within the confines of your palm, without using the other hand for help.
See if you can bunch up all the paper into your palm without using the other hand to help.

Post-surgical exercise for carpal tunnel release #3
Next, lean forward in a seated position, forearm on thigh, palm up.
Place a weighted ball in palm and lift the wrist upward, so that your palm — still holding the ball — is facing towards you. Then relax.
Repeat past point of fatigue.
If this doesn’t fatigue you within about 40 repetitions, use a heavier weight.
Small weighted balls can be found in sporting goods stores or online.
Post-surgical exercise for carpal tunnel release #4
Pretend there’s ink on the tip of your middle finger.
Keep fingers together and straight, and move just the wrist, and “draw” each letter of the alphabet in the air, pretending that the ink on your middle finger is creating the letter on a vertical sheet of paper hanging in the air.
Each exercise should be done 2-3 times each, and then each session three times per day.
These exercises are not replacements for the normal hand/finger activity that you’d do as part of your daily routine.
These carpal tunnel post-surgical exercises are supplements to your routine daily hand motions.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}