

Why You Should Never Ignore a Transient Ischemic Attack!

A TIA should never be ignored; this can lead to your death, even if the mini stroke lasts only seconds.
A transient ischemic attack (TIA) is also commonly called a mini stroke, but don’t let the terminology of “mini” trick you into thinking that a TIA is nothing to get overly concerned about.
If TIAs were called something like “stroke forerunners,” maybe they’d be taken more seriously by the general population.
Have you ever downplayed the seriousness of a transient ischemic attack because it’s usually called a mini-stroke or TIA? Don’t get snarled in this deceptive web.
“A TIA is a focal CNS disturbance caused by vascular events such as a micro-embolism or occlusion [blockage] leading to ischemia [deprived oxygen supply],” says Dr. David Beatty, MD, a retired general practitioner with 30+ years of experience and an instructor of general medicine for 20+ years.
“They last less than 24 hours, and there is a full recovery.
“Speaking generally, if someone has a TIA it increases their stroke risk x 7 compared to the normal population.
“It shows that they have this increased tendency to form clots of platelet aggregates.
“Five to 10 percent of these arise from the heart. Other medical problems are risk factors for both TIA and stroke.” These include diabetes and high blood pressure.
“If someone has had a TIA there’s a fair chance that one of these other factors is playing a part — and a 30 second TIA needs to be referred and investigated as quickly as a 10 minute TIA.”
Serious Disability from Ignoring a TIA
A study on TIAs says that serious disability can be the outcome. The report is in the journal Stroke and also adds that often, doctors don’t take mini strokes very seriously.
The paper points out that in some cases, a doctor may not give a patient a clot busting drug because the transient ischemic attack was mild.
However, a TIA or mini stroke is a significant risk factor for future disability and needs early assessment and treatment.
Don’tn let “only a few moments” of blurred vision or feeling heavy on one side trick you into thinking “it’s nothing.”
Those who’ve had a TIA should be imaged early on, and treatment should be aggressive, says the paper.
It doesn’t matter how minor the symptoms are in a mini stroke, because if imaging detects a blockage, that is serious business. A treatment called thrombolysis can dissolve blockages.
The Study
Nearly 500 patients who had a TIA took part in the study, and 90 days after experiencing their mini stroke, 15 percent had at least one mild disability.
CAT scans showed narrowed blood vessels in the brains of some patients. Other subjects reported continued or worsening of symptoms.
Amazingly, it wasn’t until 2009 that the American Heart Association and American Stroke Association recommended swift action and complete testing for a transient ischemic attack — exams that can detect a blockage in brain blood vessels.
These blockages are potential gateways to a catastrophic event.
So never mind if mini stroke symptoms pass quickly, because if you have them, this means get to the ER stat to receive the proper scans.
The study warns that ignoring a transient ischemi attack can lead to death, because not getting treatment means a massive stroke may be lurking just around the corner.
A TIA is never benign. Never.
 Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/JL-Pfeifer
Source: sciencedaily.com/releases/2012/09/120913162437.htm

Reduce Stroke Risk After a TIA with Cardiac Rehab

Cardiac rehab will help you reduce your risk of stroke after having a transient ischemic attack.
If you’ve been diagnosed with a transient ischemic attack (TIA), then you know this is a mini stroke which means you’re at significant risk for suffering a major stroke in the near future — unless you take measures to prevent this.
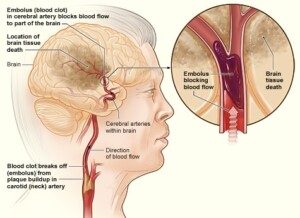
A TIA results when a blood clot in the brain chokes off oxygen to the area that the blood vessel, where the clot is, feeds.
The clot usually dissolves within minutes, so the symptoms are transient or temporary.
A report in Stroke: Journal of the American Heart Association has something to say about transient ischemic attacks.
The senior researcher, Neville Suskin, notes that cardiac rehab addresses the risk factors for a stroke.
The Suskin study was small and looked into mild stroke and TIA rather than major stroke.
Nevertheless, if you suffer a TIA or mild stroke, these are still harbingers of a major stroke in the near future.
For the study, the participatns — all whom had a TIA or mild stroke the prior year — did cardio rehab for over seven months and then were re-evaluated for risk factors.
What was the cardiac rehab?
It involved exercise, nutrition education, medication management, smoking cessation and stress reduction.
Eighty people completed the cardiac rehab. The report says that “overall,” the subjects improved quite a bit in their risk profile.
This includes peak exercise capacity. Other improvements included blood lipids, waist circumference, body mass index and blood pressure.
Eleven additional patients were recategorized to lowest death risk after initially being at moderate or high risk of dying during the following year.
Self-Cardiac Rehab
If you’re afraid of getting a transient ischemic attack or have already had one, do the same things that you’d do to prevent a heart attack.
“There are two main types of risk factors in getting stroke [or TIA] which are modifiable and non-modifiable,” says Sashini Seeni, MD, a family medicine practitioner with DoctorOnCall, an online doctor and pharmacy.
“By knowing your risk factors, you might be able to manage them accordingly to lower your chance of getting stroke.
“Routine blood pressure measurement. The higher the blood pressure, the higher the chances of getting stroke. Check your BP routinely.”
According to the American College of Cardiology and the American Heart Association, it should be under 130/80. Otherwise, consult with your physician.
“Stop smoking,” says Dr. Seeni. “It is one of the major risk factors.
“Get a healthy balanced diet. Lower your cholesterol intake, get more fiber, fruits and veggies in your menu.” Lentils and beans are particularly high in fiber.
Finally, Dr. Seeni urges people to exercise. Housework and walking Fluffy around the block don’t count.
Sign up for group fitness classes or work out at home to videos. Join a gym. Take up yoga or martial arts. Go on hikes. Buy a pair of dumbbells. The list is endless.
 DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Brian A Jackson
Sources:
sciencedaily.com/releases/2011/09/110922164200.htm
stroke/article_em.htm#transient_ischemic_attack_tia_overview
sciencedaily.com/releases/2011/09/110922164200.htm
stroke/article_em.htm#transient_ischemic_attack_tia_overview

Unsuspecting Stroke Risk: Getting Hit in the Head

There’s yet one more reason why you should try not to get hit hard in the head: It may increase your risk of a stroke.
The stroke at issue here is the ischemic type, in which a blood clot in the brain blocks blood from reaching the area that the vessel supplies.
People with traumatic brain injury (TBI), or, to put it more simplistically, a severe hit in the head, are more likely to suffer an ischemic stroke, says a paper in the June 26, 2013 online Neurology.
But there’s a reason you should not let this study scare you into thinking that the clobber in the head by a baseball you suffered in high school will give you a stroke later on.
“While this paper makes some interesting associations between TBI and ischemic stroke, the level of evidence for this study is level 4 out of 5,” says D’Wan Carpenter, DO, a board certified physical medicine and rehabilitation physician with SIMEDHealth in FLA.
The report goes as far as stating that the association between TBI and stroke is just as significant as is the link between high blood pressure and stroke.
Though stroke has some very identifiable risk factors, including smoking, diabetes and obesity, its risk factors remain perplexing to doctors, especially when the victim is under age 65.
How was this study done?
Two groups of patients were investigated: 1) adults who went to the ER or were admitted to a hospital for traumatic brain injury, and 2) those with other trauma but no TBI. Over 1.1 million patients were followed.
Results
1.1 percent of patients with TBI had a stroke over an average of 28 months after their TBIs, and 0.9 percent of patients with trauma but no TBI had a stroke.
Patients who had a TBI were 30 percent more likely to suffer from an ischemic stroke than subjects who had some kind of trauma but NO injury to the brain.
But this study, as interesting as it is, had limitations.
“It raises questions about this connection, given that individuals with TBI tend to be younger and take more risks, which may place them at risk for stroke due to lifestyle factors,” says Dr. Carpenter.
“I believe this study is one that should spark future studies to obtain higher levels of evidence in an effort to decrease another stroke risk factor if it indeed exists.”
 Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Top image: Freepik/benzoix
Source: sciencedaily.com/releases/2013/06/130626162618.htm

Do Minor TIA Symptoms Mean No Treatment Necessary?

A very brief transient ischemic attack is as much a medical emergency as is a full-blown stroke.
Sometimes, people who have experienced a transient ischemic attack (TIA) are not given clot busting drugs because their doctors don’t consider the condition serious enough to treat, says a study.
A TIA is a “mini stroke,” meaning, a blood clot forms in a blood vessel in the brain, blocking blood flow from that vessel to wherever in the brain it feeds. That portion of the brain then suffers.
However, a transient ischemic attack, like its name says, is temporary.
The clot dissolves, sometimes in under a minute, leaving the patient with no lasting effects; the patient may feel perfectly normal just a few minutes after a TIA.
A study at Foothills Hospital in Calgary, Alberta, Canada, shows that TIA patients, as well as those who had a minor stroke, are at a substantiail risk for disability and require early assessment and treatment.
No matter how minor the TIA symptoms are, the report says that early imaging of patients is crucial, and that the administration of clot busting drugs is critical if the imaging reveals a blockage in the brain.
TIA of One Very Brief Symptom vs. Full-Blown Stroke
These are equal to each other as far as degree of emergency: Get to the ER — even if what appears to be a TIA lasted only 20 seconds.
For instance, the inability to form words that lasts 20 seconds is just as much an emergency as the inability to use the right side of one’s body plus mental confusion plus double vision lasting three hours!
Whether it lasts 10 seconds or an hour, the same thing happens: a blood clot forms in the brain.
This is not something to take lightly, regardless of duration! The type of symptom is determined by the location of the stopped blood flow.
The study authors state that clot-busting treatment is not typically given because transient ischemic attacks are often deemed too mild to treat.
“Mild” TIA — is there a such thing?
“TIA is an emergency,” says Atif Zafar, MD, medical director of St. Michaels Hospital in Toronto, Ontario, and former director of the stroke program at University of New Mexico Hospital.
“If you are given a diagnosis of TIA, this means your physician is worried you have risk factors for a clot or plaque that are causing these neurological symptoms you’re complaining of,” continues Dr. Zafar.
“As a stroke neurologist, I take TIAs very, very seriously. However, if you present to the ED and your symptoms are mild and improving, we would consider holding [out] on the clot busting medication.
“Reason being, clot busting medication has a six percent chance of bleeding risks. So with you in the discussion, we have to weigh the risks and benefits of the treatment.
“Obviously, a very minor stroke with mild face numbness would not indicate the clot busting treatment if you were seen by me in the ED.
“Comprehensive TIA workup is needed to make sure we know where the clot or plaque is coming from, and how to ensure it wont act out again.
“TIA’s almost always require some change in treatment regimen. Blood thinner adjustment, cholesterol and blood pressure optimization are critical things your doctor will work with you on after a TIA event.”
A clot busting drug is not the same as a blood thinner such as Warfarin or Eliquis.
So even though you may not receive a clot busting drug, you’ll likely get a prescription for a blood thinner to take daily.
After all, if a TIA can happen once, it can happen again. The condition that causes a TIA is also perfectly capable of causing a massive stroke.
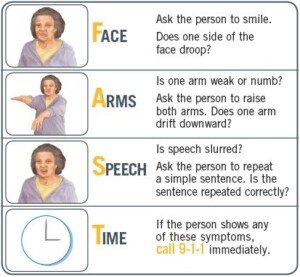
Remember “FAST” if you suspect a TIA or stroke.
More About the Study
The study involved 499 patients. Fifteen percent had at least a minor disability 90 days following their transient ischemic attack.
CAT scans revealed that some of the transient ischemic attack patients’ brains had narrowed blood vessels.
Other patients reported continuing or worsening symptoms.
These individuals were more than twice as likely to suffer disability at the 90 day mark.
For those particular patients, clot busting treatment should be considered.
After all, for every second following a transient ischemic attack, the brain may be losing oxygen.
In 2009, the American Heart Association and the American Stroke Association urged immediate action plus thorough testing for a transient ischemic attack — tests that are very similar to those given after a full-blown stroke.
The report reminds people that even though TIA symptoms “may pass quickly,” you should “immediately go to the hospital” to get the proper scans.

Dr. Zafar is author of the book, “Why Doctors Need to Be Leaders.” His interests include vascular and endovascular neurology, and the neurosciences.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik
Source: sciencedaily.com/releases/2012/09/120913162437.htm

Best Exercise to Lower Stroke Risk in Stressed People

Are you constantly under stress and worried about getting a stroke?
The good news is there’s a certain kind of exercise that will dramatically lower your chance of getting a stroke.
This type of exercise is called “hormonal.”
I’m a former certified personal trainer and I highly recommend this type of exercise that raises levels of anabolic hormones that counteract the stress hormones that thicken the blood.
What a Doctor Says
“The stress response, triggered by fear, stimulates a profound and sudden flooding of stress hormones, adrenaline and cortisol, into our blood stream,” says cardiologist John M. Kennedy in an interview for a previous article of mine.
A report in the August 2012 Journal of Neurology, Neurosurgery and Psychiatry says that chronic stress, fueled by a major life stressor and a Type A personality, is a high risk factor for stroke.
The Type A personality is the hard-driven, aggressive type, quick to show anger or get into arguments, and prone to fuming in stressful situations.
Though one might argue that this type of personality is also at higher risk for engaging in behaviors that increase stroke risk, such as smoking, drinking and eating junk food, the study (Egido et al) showed that stress is an independent risk factor for stroke.
National Heart Lung and Blood Insitute
Exercise will make a difference, but not just any exercise; it must be “hormonal” exercise — the type of exercise that triggers elevated secretion of human growth hormone (HGH) and testosterone.
These hormones oppose cortisol, the “stress hormone,” and adrenalin.
What is hormonal exercise?
Hormonal exercise helps unthicken the blood that stress thickens. When we are under chronic stress, our body prepares for a fight or flight.
The blood thickens and the blood platelets get sticky (making it more clottable) to protect us from bleeding to death from a gash during the fight or flight.
Problem is … with modern man, the fight or flight never happens.
Instead we remain immobilized in a traffic jam, an office cubicle, a business meeting — places where we can’t act out physically.
Stroke in the Making
Our blood stays thickened and sticky. If your blood remains this way chronically, you are at much higher risk of ischemic stroke (blood clot in the brain), since thick blood is more prone to clotting!
“Getting stuck in traffic can lead to increases in stress hormones which over time can wreak havoc on our cardiovascular tissue,” adds Dr. Kennedy, medical director of preventative cardiology and wellness at Marina del Rey Hospital, and author of the book, “THE 15-MINUTE HEART CURE: The Natural Way to Release Stress And Heal Your Heart In Just Minutes A Day.”
This is why blood thinning drugs are recommended to people at risk for stroke. Another way to “unthicken” blood is via hormonal exercise.
The intense physical exertion from a fight or flight releases HGH and testosterone. These cancel out the stress response that thickens the blood.
In a modern society, fight or flight exercise comes in two forms, both of which incite the hormonal response that opposes stress hormones:
High Intensity Interval Training and Heavy Weightlifting
- Jogging for an hour won’t cut it.
- Standing on wobble boards and pressing little dumbbells overhead won’t cut it.
However, dashing up a few flights of stairs as fast as possible while holding a 10 lb. dumbbell in each hand (or faster without a weight) will spark a completely different environment in your body that will immediately start going to work at hacking away at the stress hormones.

Intense exercise, aka “hormonal,” is a huge weapon against stroke, especially in stressed people.
In a nutshell, hormonal exercise consists of very brief bouts or bursts of HIGHLY INTENSE exertion, alternating with a few minutes or even five minutes of casual effort.
Imagine, for example, sprinting up a hill, multiple staircases or bleacher steps as fast as you can, boom boom boom — until you just can’t take another step.
You then pace very slowly while you gasp for air, letting your body recover. After several minutes you go all-out again — for only 15 seconds, maybe 30 seconds.
This type of workout is often referred to as either high intensity interval training or burst exercise.
Resistance Training and Stroke
Heavy weightlifting such as an eight repetition max of an all-body exercise such as the deadlift will also help lower the risk of stroke in stressed men and women.

Other great exercises include any kind of pulling, such as pulling resistance down from above yourself while in a seat, or pulling resistance horizontally towards yourself while in a seat; and any pressing motion such as a dumbbell press.
Don’t forget the legs; any type of squat works very well, as well as the leg press and sled push.
Exercises like this will change the hormonal environment in your body and protect against chronically thickened blood that leads to blood clots in the brain: stroke!
 Double board certified in cardiovascular disease and also internal medicine, Dr. Kennedy’s special interest is stress and how it adversely affects a person’s delicate cardiovascular system.
Double board certified in cardiovascular disease and also internal medicine, Dr. Kennedy’s special interest is stress and how it adversely affects a person’s delicate cardiovascular system.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Sources: sciencedaily.com/releases/2012/08/120829195207.htm; http://www.cdc.gov/stroke/facts.htm

Does Stress Change the Brain to Cause a Stroke?

Could it be that chronic stress creates adverse changes in the brain that eventually lead to a stroke?
An ischemic stroke is a blood clot in the brain that shuts off oxygen supply to the area that the blocked vessel feeds.
If you think that mental stress that causes heart disease can then trigger a stroke from the heart, wait till you find out about a Swedish study that implies that stress does something to the brain that makes a brain-originating stroke more likely.
The type of stroke in this study was the blood clot kind: A blood vessel in the brain gets a clot that obstructs blood flow to whatever part of the brain that the vessel feeds (also known as a cerebral infarction).
This is more commonly called an ischemic stroke, and the clot can originate from the heart (usually from diseased arteries; the clot in this case is a coronary plaque fragment that travels “upstream” from the heart and gets into the brain).
Or, the clot can develop in a blood vessel of the brain itself.
The study comes from the Sahlgrenska Academy at the University of Gothenburg and Sahlgrenska University Hospital, Sweden.
Neurologist Katarina Jood says that interpreting the correlation between mental stress and stroke must be done very cautiously, because for the study, patients who’d had a cerebral infarction were questioned (within 10 days of hospital admission) about their stress levels in the five years prior to their cerebral event.
The problem is that a cerebral event can alter one’s perception or memory of their recent past.
Nevertheless, about 600 patients were asked to fill out a questionnaire, to rate their stress levels over the preceding five years.
Their responses were compared to those of a healthy control group who filled out the same questionnaire.
Findings
There was an independent link between self-perceived mental stress and stroke.
However, this correlation wasn’t the same for the three kinds (in terms of origin) of ischemic stroke that were studied.
– Stress and cerebral infarction were linked when the stroke was caused by blood clots that developed in the brain.
-Stress and cerebral infarction were linked when the stroke was caused by blood clots of undetermined origin.
-Intriguingly, this study did not show a correlation between stress and stroke when the clot originated from the heart.
(Tests are used to determine the origin of the blood clot.)
Might this mean that chronic stress has an adverse effect on blood flow in the brain?
The study was not able to determine why stress seems to play a bigger role in particular kinds of stroke.
Nevertheless, stress and stroke are intertwined.
Your Stress Response

Shutterstock/Charnchai Saeheng
“The stress response stimulates a profound and sudden flooding of stress hormones, adrenaline and cortisol, into our In the modern world, however, the stress response gets triggered much more often – not by saber toothed tigers but by things such as forgetting to pay a major bill, a visit to the dentist or MRI machine, or hearing your boss say in an unpleasant tone, “I need to see you in my office.”
The result, over time, is increased inflammation, high blood pressure and heart rate, and the increased ability of blood to form clots.
“These physiologic changes create the perfect storm for a stroke,” says Dr. Kennedy.
The risk of atherosclerosis goes up. This condition causes plaque formation in blood vessels.
“Eventually, these changes damage the delicate inner lining of blood vessels and lead to a heart attack or stroke.”
Double board certified in cardiovascular disease and also internal medicine, Dr. Kennedy’s special interest is stress and how it adversely affects a person’s delicate cardiovascular system.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik,katemangostar
Source: sciencedaily.com/releases/2009/10/091001101502.htm
What Happens in the ER for a Chronic Subdural Hematoma?

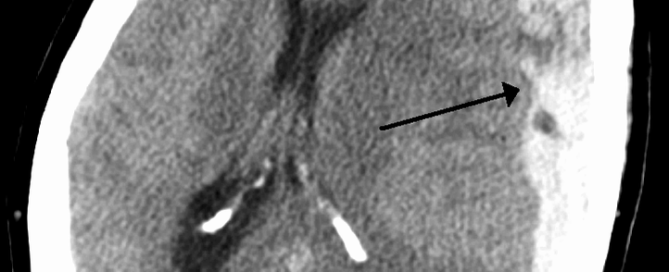
The diagnosis of a chronic subdural hematoma in the emergency room is easy to make: A CT scan easily reveals the collection of blood. But what happens once this diagnosis is made?
My mother went into the ER with alarming symptoms and was ultimately diagnosed with a chronic subdural hematoma.
You may have heard of the words, “subdural hematoma,” and think that this is always an emergency situation that can kill in minutes.
However, there are three kinds of subdural hematoma, says MedlinePlus: acute, subacute and chronic.
Symptoms can occur immediately after a head trauma, or not show up for a few months after the head trauma.
In my mother’s case, the symptoms began appearing six weeks after she fell and hit her head.
In the ER, the doctor suspected a stroke (she had lower body weakness, more so with the left leg, and a bad headache) and didn’t even mention chronic subdural hematoma. A CAT scan with contrast dye was ordered.
Meanwhile the ER doctor gave my mother a neurological exam which included things like asking her to lift her legs against the doctor’s hand resistance.
The CAT scan revealed the chronic subdural hematoma (blood in the brain leaking from torn veins).
In my mother’s case (I am not speaking for ANY or ALL cases of chronic subdural hematoma), she was admitted to the neurology unit of the hospital, and told that she would have surgery the following morning to drain the blood.
I asked why was there a delay; won’t it get really worse overnight? The doctor said that if it were an emergency, they would not wait till next morning to operate.
It was not an emergency and it was not expected that the situation would deteriorate overnight. The doctor believed that my mother’s condition was stable, and told me throughout the night she’d get neurological checks by the nurses.
This was the first time I’d ever learned of the “chronic” type of subdural hematoma.
I’d always believed that if symptoms of a hematoma began weeks after the head trauma, that the situation was just as potentially fatal as when the symptoms occur rapidly right after the head trauma.
The idea of a very gradual, slow leakage of blood had never occurred to me, probably because I first learned of “subdural hematoma” after watching a clip of a boxer receiving the “fatal blow” in a professional match, knocking him out cold.
This had fascinated me because the boxer wasn’t just unconscious, but his body was rigid (“posturing”) as the medics cumbersomely hoisted him (though he was extremely thin) onto the stretcher. This stuck in my mind.
However, when the ER doctor said my mother had a “chronic” subdural hematoma, I instantly realized that this was a less serious form, not to be compared to the one that the boxer had suffered.
A neurosurgeon was contacted and the surgery was tentatively for next morning. The ER doctor was not able to give fine details other than explaining that the procedure involved drilling a hole in the head and draining the fluid.
Though this sounds invasive, the surgery is actually non-invasive and minor. The ER doctor said it was a 10-minute procedure.
My mother was transferred to the neurology wing and set up in her room. Next afternoon she had the surgery which involved general anesthesia, but the neurosurgeon indeed said it would take about 15 minutes and he didn’t seem the least bit worried, as though this was not much more than wrapping a sprained ankle.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: James Heilman, MD/CreativeCommons
Sources:
nlm.nih.gov/medlineplus/ency/article/003300.htm
nlm.nih.gov/medlineplus/ency/article/000781.htm
Chronic Subdural Hematoma: tPA plus Blood Thinners in Stroke Patients
Here’s information concerning risk of chronic subdural hematoma resulting from tPA combined with blood thinners in stroke patients.
Many men and women take blood thinning drugs to help prevent stroke.
Thicker blood is more likely to form dangerous clots, but thinner blood is more likely to cause bleeding in the body, such as a “chronic subdural hematoma.”
This is slow bleeding in the brain; patients over age 65 are at greatest risk compared to other age groups.
Suppose you’re on blood thinners but you have a stroke anyways. Prompt medical treatment will include tPA: a potent clot-busting drug.
But you already have blood thinners in your system, so won’t the addition of tPA put you at risk for a subdural hematoma: a brain bleed?
A new study from the University of Michigan Stroke Program says that risk of brain bleed, under these circumstances, is low for most patients on blood thinners.
The investigation looked at data from 830 patients who’d received tPA for their stroke.
A little under 50 percent of these patients had been on the blood thinner Plavix, or aspirin, prior to their stroke.
After adjusting for variables, the researchers found no substantial difference in the rate of brain bleeding, based on brain scans. This included low-level bleeding that produced no symptoms.
Patients, plus ER teams, need to be reassured that administering tPA to stroke patients, who already have blood thinners in their system, isn’t dangerous or likely to cause bleeding in the brain. The full report is in the March 2013 Academic Emergency Medicine.
Patients Over Age 81 Had Small Increased Risk
The report mentions, however, that patients over 81 did sustain a small increased risk of brain bleeding, though non-symptomatic.
Which blood thinners?
The study examined patients on aspirin and Plavix, not the stronger blood thinners like heparin, warfarin (Coumadin), Pradaxa or Xarelto.
Unfortunately, the study team says that giving tPA to stroke patients on these stronger drugs needs more investigation.
“In light of the long-term benefit that patients receive from antiplatelet therapy,” says lead author William Meurer, MD, “the small increase in risk of intracranial hemorrhage after tPA treatment should not be a game-changer for emergency physicians.”
Dr. Meurer, assistant professor of emergency medicine at U-M Medical School, adds that this study shows that doctors should not hesitate to give tPA to stroke patients who’ve been taking aspirin or Plavix.
A “chronic” subdural hematoma is when the brain bleed doesn’t happen within several days of the causative agent, and instead, begins showing signs or is detected on scan anywhere from a few weeks to 90 days out.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: James Heilman, MD/CreativeCommons
Sources:
sciencedaily.com/releases/2013/03/130313095301.htm
pmj.bmj.com/content/78/916/71.full
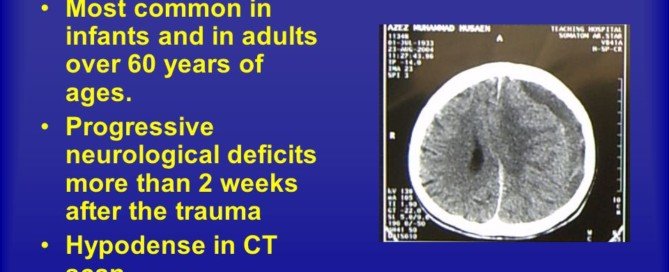
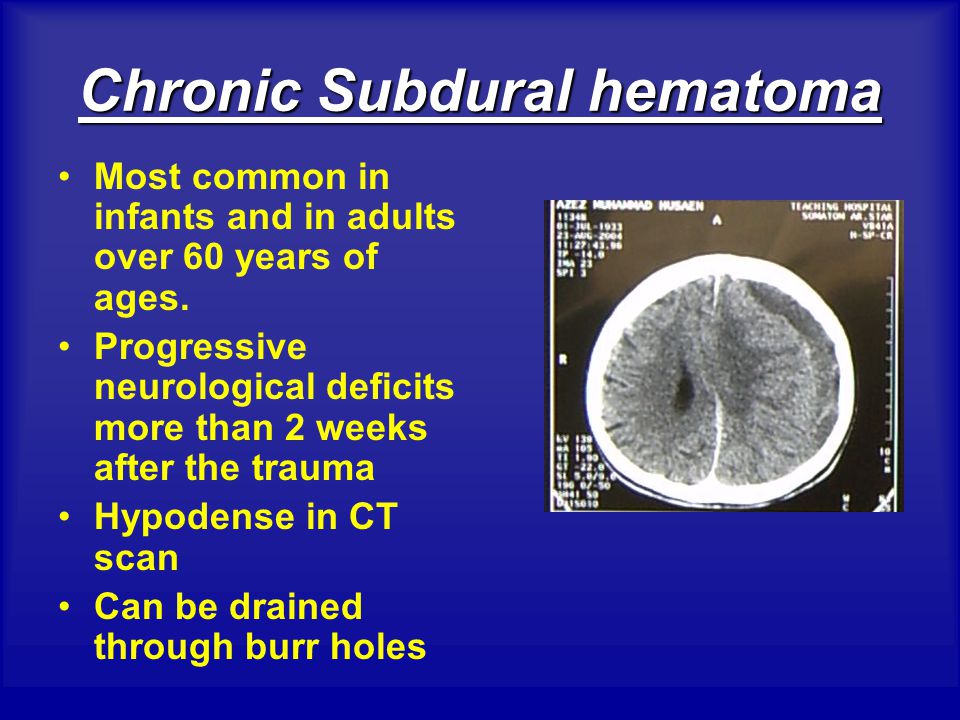
Most Common Symptoms of Chronic Subdural Hematoma in Elderly
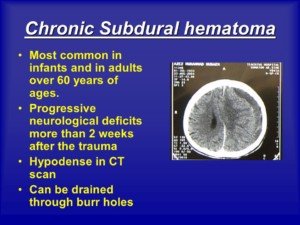
The most common symptoms of a chronic subdural hematoma in the elderly differ from those in younger patients.
“A chronic subdural hematoma is a collection of blood on the brain’s surface, under the outer covering of the brain (dura),” says Sashini Seeni, MD, a family medicine practitioner with DoctorOnCall, an online doctor and pharmacy.
“It is a common neurological condition affecting the elderly,” continues Dr. Seeni.
The chronic nature means this situation begins showing symptoms at least a few weeks after the head trauma (which in elderly people, may be quite trivial such as banging their head on a car door frame when getting into the vehicle).
“Chronic subdural hematoma enlarges from recurrent bleeding in the subdural space which comes from the leakage of blood of a torn vessel into a space below the dura mater,” explains Dr. Seeni.
The Postgrad Medical Journal (2002, Vol. 78) provides an extensive list of symptoms pertaining to chronic subdural hematoma in the elderly.
Altered Mental State
An altered mental state is the most common presentation, says the PMJ paper.
This occurs in 50-70 percent of patients. The alteration in mental status can mimic delirium or dementia, says Dr. Seeni.
“Thus, they should be considered in the differential diagnosis of elderly patients presenting with neurological signs and symptoms.”
My elderly mother had a chronic subdural hematoma twice: the initial one and a recurrence about 10 days later.
Her mental state with the first one seemed normal, though it was odd that she wasn’t alarmed over her severe leg weakness.
Her mental state with the recurrence was altered: a mild level of impaired reasoning.
The PMJ list includes confusion, drowsiness and acute delirium.
As my mother’s recurrence unfolded, she developed acute delirium, but the ER doctor attributed this to an adverse reaction to the Medrol Pak (oral steroid drug to reduce brain inflammation).
Unconsciousness is another possible symptom of chronic subdural hematoma in the elderly.
Focal Neurological Deficit
This is the next category of most common symptoms of chronic subdural hematoma in elderly patients.
One study, as reported in the PMJ, found that 58 percent of elderly patients suffered weakness on one side of the body. My mother had it in both legs.
Focal (confined to a specific part of the body) deficits will usually remain persistent, rather fluctuate, says the PMJ.
My mother’s significant leg weakness never subsided prior to treatment.
However, it’s not known how insidiously it developed because at around 7 a.m. that morning, she reported feeling normal when she arose to use the bathroom.
She returned to bed and around 10:30 a.m. got up, and that’s when a mobility problem was quite obvious.
Headache
“The pressure of hematoma in the subdural space causes the headache in the elderly,” says Dr. Seeni.

Shutterstock/Prostock-studio
Headache incidence varies from 14-80 percent depending on the study, says the PMJ.
My mother’s initial occurrence included a “crown of thorns” headache, as she had described it at the time.
Though headache is the third category of likelihood of symptoms reported in the PMJ, a headache is a less common symptom in the elderly than in younger people with chronic subdural hematoma.
This is because there’s less space in the bigger brain of a younger person for the fluid buildup to occur.
Falls
A study of 43 elderly patients found that falls occurred in 74 percent, notes the PMJ report.
Ironically, falling as a symptom of cSDH can make the cSDH worse.
Falls as a symptom may result from neurological deficits, altered mental state or postural disturbances.
Seizures
Seizures are a rare symptom of chronic subdural hematoma, though patients with pre-existing epilepsy may have increased seizure activity with a cSDH.
A chronic subdural hematoma can produce a simple partial seizure as its only symptom. This can mimic a transient ischemic attack.
Transient Neurological Deficits
The PMJ says the incidence of TNDs is 1-12 percent. In the elderly the most common TND symptom from chronic subdural hematoma is one-sided paralysis or numbness.
There’s been at least one case reported of on-and-off partial paralysis of the lower limbs due to a cSDH on both sides of the brain.
Rare Symptoms of Chronic Subdural Hematoma in Elderly Men and Women
Vertigo; fast, uncontrollable eye movements; tremoring (Parkinson’s-like); right-left disorientation; unawareness of one’s fingers; inability to write; inability to do simple math; and slowly tilting towards a fall without making postural adjustments due to unawareness of this.
My mother’s recurrence of chronic subdural hematoma produced a most intriguing symptom: left side neglect.
A person with severe left side neglect may refuse to believe that their left leg and arm are theirs.
My mother would make right turns when told to go walk left, and would try to pick things up with her left hand and miss the object, yet think she had it in her hand!
My mother eventually fully recovered from both her chronic subdural hematomas.
DoctorOnCall is the largest digital healthcare platform for citizens of Malaysia, allowing patients to consult doctors for advice, book appointments and place orders with local pharmacies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: pmj.bmj.com/content/78/916/71.full

Doctor Didn’t Warn of Future Brain Bleed when CT Scan Was Normal

My elderly mother’s doctor didn’t warn her that she could get a chronic subdural hematoma even though her head CT scan was normal.
Elderly age plus head trauma = fair chance of developing a chronic subdural hematoma, and this chance jumps when the elderly individual is on the blood thinner Coumadin at the time of their fall.
It has long been recognized that elderly individuals are more likely to develop a subdural hematoma (brain bleed), particularly from minor trauma.
“As we age our vessels age with us,” says Reena Patel, MD, a board certified family medicine physician who treats patients at Garnet Health Urgent Care in NY.
“Our capillaries, arteries and veins harden — some more than others, depending on history of hypertension, hyperlipidemia and overall health/genetics.
“Some may even experience decrease in overall brain size. This makes it easier for vascular injury.
“A small vessel in the brain can have a break, leak or tear that over time can cause a deep impact.”
Shrunken Brain
When aging causes the brain to shrink, this increases the amount of space between it and the skull from 6% to 11% of the total intracranial space. The bridging veins then stretch.
The brain can move more due to the increased space, and this makes these veins more vulnerable to tearing from getting hit in the head or hitting the head from a fall.
Every elderly patient who has a normal CT scan following a fall or other hit to the head should be warned to be on the lookout for future symptoms.
“Symptoms of a slow brain bleed can include: headache (most common), neurological deficits such as weakness in a limb, balance issues or paresthesias, slurring of speech and confusion, to mention a few,” says Dr. Patel.
Normal Head Scan but Brain Bleed Weeks Later
My elderly mother had a normal CT scan, and then another one 24 hours after that, following a fall and visible injury to her head.
I asked the ER doctor, “What about the chance that a few months down the road, there’s bleeding in her brain?”
The doctor said, “There’s a very slim chance of that.”
Six weeks later my mother awakened with a searing headache and significant lower body weakness, out of the blue.
A CT scan later in the day showed a chronic subdural hematoma.
At the time of her fall, she still had Coumadin in her system (she’d gone off it the day prior).
The original ER doctor had actually known she was on Coumadin.
This doctor never told my elderly mother about the blaring risk factors for a chronic subdural hematoma: hit on head (it’d even been bloodied), elderly age and Coumadin!
Several years later my father had an apparent blackout while standing and fell face down.
He was on Coumadin. The fall resulted in a “goose egg” purple and red swelling on his forehead.
Nobody at the ER informed him that there’s a fair chance that a few weeks or months down the road, he may develop symptoms from a chronic subdural hematoma.
Of course, I then knew this already, and was vigilently on the lookout for neurological symptoms in the ensuing weeks.
“The CT scan is normal,” was all my parents got.
Because elderly patients may not get a warning about chronic subdural hematoma, they and their family often don’t have a clue what’s going on weeks or up to three months later when the neurological symptoms start developing.
The symptoms of these brain bleeds can mimic dementia, stroke and mini-stroke.
If you’re elderly (or know someone who is) and have recently hit your head, and the CT scan was normal, even one 24 hours later — consider the next few months as an incubation or grace period for the development of a chronic subdural hematoma.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}