

Appetite Loss Causes OTHER than Ovarian Cancer

You don’t overeat, you don’t have ovarian cancer, so why have you lost your appetite?
Have you been feeling full “all the time” even though you haven’t been eating more, and even though your doctor said you don’t have ovarian cancer?
Feeling full all the time is a nonspecific symptom, says Michael Blume, MD, a gastroenterologist at MedStar Good Samaritan Hospital, Baltimore.
He explains, “One needs to distinguish whether this is a problem with gastrointestinal structure (i.e., obstructive or inflammatory problems) or gastrointestinal function (this may include metabolic problems, medications, as well as functional gastrointestinal disorders).
“Diagnosing this would likely involve a combination of taking a medical history as well as some diagnostic testing.”
For women who have noticed a persistent full feeling, one of your first stops, if not your very first stop, should be with a gynecologist.
Ask the doctor to see if your ovaries are doing well.
Keep in mind that the absence of ovarian cancer does not mean that some other cancer can’t be causing you to feel disproportionately full relative to the amount of food you eat.
Cancers that can subdue the desire to eat include stomach, colon, pancreatic and lung.
Additional Causes of a Suppressed Appetite
– Addison’s disease
– Anxiety
– Celiac disease
– Chronic heart failure
– Crohn’s disease
– Dementia
– Depression
– Diabetes (though this also often causes intense hunger)
– GERD
– Kidney disease
– Liver disease
– Pancreatitis
– Rheumatoid arthritis
– Side effects of cancer treatment
– Stress
– Tapeworm
– Ulcer
– Ulcerative colitis
This list of causes of appetite loss is not complete.
If you’ve been experiencing a loss of appetite lately, then the more symptoms that occur with this, the more concerning your situation is.
For example, a suppressed appetite that’s also accompanied by vomiting, unexplained fatigue and/or abdominal pain should be immediately checked out by your doctor — regardless of your age — or gender.
 In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/VGstockstudio

Non-Cardiac Causes of Dizziness when Eating

If it’s not your heart, what can be causing dizziness while you eat?
Eating should be an enjoyable experience, not something you dread because it causes you to feel dizzy.
Non-cardiac causes of dizziness while eating are many.
“One needs to remember that just because you are having gastrointestinal symptoms, does not necessarily mean that this is from a gastrointestinal problem,” says Michael Blume, MD, a gastroenterologist at MedStar Good Samaritan Hospital, Baltimore.
He continues, “This is a nonspecific symptom and can be related to metabolic or neurologic issues.”
Getting dizzy when eating can have a number of causes.
Dr. Blume explains, “One can see this from problems involving abnormal gastrointestinal function, such as when one’s autonomic nervous system (the part of your nervous system that works without you thinking about it) — specifically the parasympathetic nervous system — function is abnormal, where one can get dizzy after eating.
“However, one often gets other symptoms along with this, such as feeling clammy, flushed, nauseated or having erratic bowel function.”
If dizziness during eating keeps happening to you, make an appointment with your physician. This is not normal and needs to be evaluated. There is no known food that makes a person feel dizzy or causes vertigo while it’s being eaten.
Occasional dizziness when eating is probably not caused by eating or anything related to the GI tract. Rather, it’s likely a coincidence in that whatever the cause of the symptom is, just happens to act up while you are eating.
Keep a record of these events so that you can potentially identify a pattern, or at least, present to your doctor. Documentation can help you determine if the dizziness does or does not occur at other times unrelated to food intake.
You can make a note if there are other symptoms that may suggest a cardiac problem such as chest pain, feeling faint and/or feeling short of breath.
In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/9nong

What to Tell Cardiologist if You’ve Been Passing Out

A cardiologist explains the details you should give your cardiologist if you’ve been blacking out.
Have you been blacking out and are planning on seeing a cardiologist?
Don’t just tell the doctor, “I’ve been having blackouts; what’s wrong?” Certainly, your doctor will ask questions to get more information, but you should also be prepared to give specific information.
You should tell the doctor “the exact symptoms before and after the blackout,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Dr. Sayeed continues, “Whether they could feel it coming or if it was just like a flip of a switch — awake one minute, found on the ground with facial and head injury the next without warning.
“They should tell their cardiologist if they felt any abnormal heartbeat, palpitations, chest pain, lightheadedness, dizziness before it happened, or if they feel changes in certain positions make them feel like passing out.
“They should tell their doctor if it occurred after urinating, a big bowel movement, meal, extreme activity or taking medication.
“They need to tell the doctor if they are diabetic and taking diabetic drugs or exercising. Whether they feel completely normal or awakening from the blackout and feel funny.”
Though blackouts can have non-cardiac causes, it’s important to rule out any possible heart problem.
Dr. Sayeed says cardiac causes can be a “slow heart rate; pauses in the heart beat; fast and irregular heart beat; severe obstruction of a heart valve; and carotid sinus hypersensitivity causing fainting with changes in position.”
Of course, the sooner you see a cardiologist after a blackout, the less you’ll have to tell your doctor, but some people DO put off seeing a doctor, or, they see a doctor but fail to give as much information as they are capable of.
So every time you have a blackout, it’s vital to document all the details that you experienced just prior to it, after it, and even within 15 minutes of it, to see if a pattern emerges.

Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com jcomp

CT Angiogram for Chest Pain: Cost, Availability & Safety

If studies show the accuracy of CT angiogram for detecting heart disease, why isn’t this tool used more often in chest pain ER cases?
Research have shown the efficacy of the CT angiogram in detecting heart disease in patients presenting to the ER with chest pain, so it makes absolutely no sense to me, the layperson, why this tool isn’t used in a standard way across the board in emergency room settings.
“Coronary computed tomographic angiography (CCTA) has been shown to have a high negative predictive value for the detection of coronary disease,” says Donna P. Denier, MD, of The Cardiology Center with the Appalachian Regional Healthcare System in NC.
“That is, it is very useful in ruling out the presence of coronary disease, even more than ruling it in,” continues Dr. Denier.
“The issues of its usefulness are cost, availability and safety. The majority of patients who present to an emergency department with chest pain can be categorized quickly into one of three groups based on a careful history, physical exam, evaluation of risk factors and review of EKG and troponin results.”
Troponin is an enzyme that leaks from the heart when there is cardiac muscle damage (heart attack).
Thus, as you may now be realizing, a troponin test detects a very recent or current heart attack, not blocked coronary arteries.
My mother’s troponin results were normal after I took her to the ER when she complained of shortness of breath and had vomited.
Three days later (after a second ER visit) she underwent quintuple bypass surgery!
Dr. Denier continues, “High risk patients are admitted and usually undergo cardiac catheterization (such as my mother) which makes a rapid conclusive diagnosis and allows for treatment at the same time.
“Low risk patients (e.g., athlete, under age 50, nonsmoker, healthy body weight/blood sugar/blood pressure) can be sent home and followed as outpatients for further testing.
“For low risk ambulatory patients, a stress test is the best test to rule out coronary disease because it gives functional information as well—how how far a patient can walk without developing symptoms.”
What about the moderate risk patient in the ER with chest pain? “It is the moderate risk patient who requires a test to safely rule out the presence of significant coronary disease,” says Dr. Denier.
“CT angio is clinically useful in this group. As this test is performed while the heart is beating, quality imaging is dependent upon slowing the heart rate enough to image between cycles.
“This limits some patients due to rapid or irregular heartbeats that cannot always be controlled with medication. Some patients cannot tolerate the medication that is used to slow the heart.
“Radiation exposure is another concern and although this has been reduced by newer technology, all centers do not have the latest equipment.
“Cost is definitely a limiting factor, and the test is not universally covered by insurance companies, as it is still considered a screening test.
“As technology evolves, cardiac CT will continue to be one of the techniques considered for the rapid and accurate evaluation of patients with chest pain.”

Dr. Denier has been practicing medicine for over 20 years and is board certified by the American Board of Internal Medicine – Cardiovascular Disease.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Tests from a Cardiologist to Evaluate Why You’re Fainting

A cardiologist talks about blackouts and what tests you should get to find out if the problem is heart related.
Have you been having blackouts and “all the tests” are normal? Perhaps you haven’t had the right tests.
First of all, the doctor you should initially see is a cardiologist, since blackouts can be caused by serious heart problems that need immediate attention.
So just what are the tests you should insist upon for blackouts?
“One could consider an echocardiogram to make sure there are no problems with the heart valves,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Dr. Sayeed continues, “A holter monitor could check for abnormalities in the heartbeat. A stress test could look for abnormal heartbeat with exercise. A tilt table test could evaluate for blackout with different positions.”
Some people black out soon after rising from a prolonged seated position. Their blood pressure plummets and the brain is starved of oxygen, causing the blackout.
The tilt table test measures blood pressure when the patient is in various positions.
Can a seemingly healthy person, with no previous concerning symptoms, suddenly one day drop from a blackout?
“Yes, this can certainly happen, as the electrical system in the heart can suddenly decompensate, especially in an older person, and this is why they frequently come in with bruised or injured faces or head injury.”
On the other hand, a person can begin experiencing suspicious symptoms, short of an actual blackout, that progress over time, one day culminating in a full fledged loss of consciousness.
Dr. Sayeed, explains that “there can be a transition period, especially if they are just having brief episodes of abnormal heartbeat and if this progresses over time to worsen the heartbeat. The symptoms can get worse and eventually lead to syncope.
“This is usually less common and usually a more drastic sudden blackout is how patients usually present.
“But certainly a gradual onset over time can occur especially if the person can tolerate the symptoms quite well.”
If you have even ONE blackout, do not delay getting tests, because this symptom is never normal.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Image Point Fr

Shortness of Breath from Heart Problem vs. Narcotic Drugs

Is there a way to distinguish between breathing difficulty from angina and from narcotic painkiller side effects?
Narcotic painkillers can cause trouble breathing as a side effect, yet angina as well can result in this scary symptom; is there a way to tell one type of labored breathing from the other?
“Narcotic side effects would make them drowsy or unconscious, and breathing would become dangerously slow or even stop, and the person may not even realize it,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“Angina is usually reproducible with the breathing difficulty happening each time they do a certain amount of activity, walking, etc., and once it is severe would even occur at rest, and the person would be very uncomfortable and definitely would realize it.”
So if you’re on narcotic painkillers, and you feel fine all along, and suddenly develop difficulty breathing, chances are very high that this is NOT a side effect from the narcotic drugs.
It’s not necessarily angina, either, but you can pretty much rule out narcotic side effects if this is your only symptom, and especially if it came on during mild exertion that’s too light to justify the shortness of breath.
My mother had been on narcotic painkillers, and on and off complained of “labored breathing.”
We all thought it was from the narcotics because the inserts listed this symptom as a possible side effect (along with a huge host of other potential side effects).
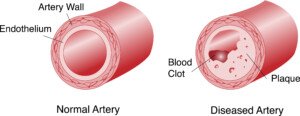
It’s much more likely that all along this symptom had been caused by severe coronary artery blockage, because eventually she was diagnosed with very severely blocked arteries (after being diagnosed with unstable angina), and had to undergo coronary bypass surgery.
If you’re worried about your heart health, see a cardiologist and also have your coronary calcium score taken.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/PrinceOfLove
Why a Stress Test Can Miss Severe Artery Blockage
Find out how often and why cardiologists miss severe heart disease when examining a patient.
It’s possible for a cardiologist to miss severe heart disease when giving a patient a heart exam, and actually go as far as telling the patient, “You’re the last person I’d ever expect to have a heart attack.”
This happened to my mother. Ten months later she had emergency quintuple bypass surgery.
“This can happen if the stress test is normal but the patient has severe triple vessel coronary disease,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“Some nuclear stress tests can be normal in the setting of triple vessel disease due to a phenomenon called balance ischemia where the blood flow discrepancy cancels each other out and the test appears normal.”
In other words, relative blood flow is detected, rather than absolute blood flow.
Thus, if only one or two of the three major vessels is/are severely blocked, this will cause a disparity in blood flow that will be easily detected.
How common is balance ischemia as a camouflage in a stress test?
Dr. Sayeed says, “This probably happens in a relatively small percentage of people, 5% or less. A cardiologist with a high suspicion of disease based on symptoms and exam and history would not trust the falsely normal stress test and probably perform a coronary angiogram.”
But what if the patient reports no symptoms?
My mother did not have symptoms 10 months before three doctors said that a massive heart attack was imminent.
She saw a cardiologist because an EKG, taken in the ER as part of a complete workup to find out why she was sleeping so much, revealed a “left bundle block.” The ER doctor told her to follow up with a cardiologist.
The cardiologist did not order a stress test or any other imaging procedure.
She gathered subjective information from my mother, then examined her with a stethoscope, noted the pulse and blood pressure, and declared her heart healthy.
If the patient has no symptoms, has normal blood pressure, normal pulse, is not diabetic, does not smoke or drink, is not obese and reports no family history of heart disease, what SHOULD the cardiologist do?
When the cardiologist asks the patient, “Do you exercise?” and the patient says, “Well, I maintain a large house that has a staircase, and I’m up and down those stairs a hundred times a day,” the cardiologist should see a blaring red flag.
When people say things like this, assume they are sedentary!
A staircase in the house does not mean the resident has a built-in cardiovascular exercise program!
My mother had three blaring risk factors for severe heart disease that the cardiologist should NOT have missed:
1) elderly age
2) lack of structured aerobic exercise
3) excess fat in the midsection (though she was not obese).
The cardiologist should have probed further with the exercise — for example:
“Do you do any brisk walking for at least 30 minutes most days of the week — and whatever walking you do while shopping does not count.”
And, “Do you take any fitness classes? Do you use any cardio machines like a bike, treadmill or elliptical? Do you jog?”
Sedentary people have a way of convincing themselves they get “plenty of exercise” by believing that housework and shopping count as sustained, rhythmic cardiovascular exercise!

Freepik.com
Though probing the exercise habits often will not turn up useful information when so many people believe that walking 3 mph on a treadmill while holding on counts as meaningful cardiovascular exercise, the probing can definitely yield insight to the cardiologist screening for severe heart disease.
The cardiologist asked my mother about her diet.
My mother replied, “I eat a balanced diet. I hardly eat fast-food. I watch my portions. I don’t eat much sweets.” The cardiologist did NOT probe further.
The problem isn’t so much the type of food; it’s the BRAND.
Popular, commercial brands of processed goods (potato mixes, pasta mixes, seasoning packets, salad dressings, bread crumbs, frozen dinners, frozen side dishes, processed frozen meats) are full of trans fats, which damage coronary arteries!
My mother’s diet was rich in heavily processed foods: trans fats! Trans fats are also “hidden” in foods whose packaging says “Zero trans fats!”
As for no family history of heart disease, my mother confidently declared this, even though at the time, her son had been diagnosed with heart disease years before, and she had siblings whose health histories she was not aware of (one eventually had a heart attack!).
Do you now see how easy it is for a cardiologist to miss severe coronary heart disease?
Shutterstock/OSweetNature
If you’re worried about your heart, be sure you know the FACTS to what seem to be simple questions that the cardiologist will ask about your lifestyle and family history.
And get your coronary calcium score taken; discuss this with your cardiologist, as this can be extremely telling of the presence of severe coronary heart disease.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Zero Calcium Score: How Soon Can a Bad Diet Raise It?

If your calcium score is zero and you go bust with your diet, how long before the score rises?
Your calcium score is zero because you’ve been having a healthful diet and exercising, and maybe there’s some good genetics and/or youth tossed into the equation.
But let’s suppose that lately you’ve been gorging on sugary foods with trans fats, and eating very little of the vegetables and fruits you used to eat a lot of.
Maybe you’ve been stressed. Stress can lead to junk food consumption as a form of emotional relief or comfort.
The body’s stress response triggers cravings for high-fat, high-sugar foods, which can temporarily boost mood.
How long do you have to keep up this bad diet before it raises that calcium score of zero?
“Usually a calcium score or stress test gives an average person about a three to five year warranty in that if it is normal, the risk will probably be low for that period of time,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“If someone is abusing their diet, it is possible that plaque could build up in three to five years’ time to the point where it could be detected on calcium score,” adds Dr. Sayeed.
“This is about how often stress tests, but not necessarily calcium scores, are repeated to monitor for new flow-limiting plaques.”
If your calcium score is zero, indicating no significant calcified plaque in your coronary arteries, it’s important not to use this as an excuse to abandon healthy eating habits.

The closer a food is to its natural state, the healthier it is for the human body, especially the heart.
Consuming a menu high in processed foods and added sugars can still pose risks to the person with a zero calcium score, because sugars contribute to coronary artery plaque buildup over time.
While a zero calcium score is a positive sign, maintaining a plant based diet rich in whole foods and low in processed sugars is the magic bullet for long-term heart health and preventing future cardiovascular issues.
You should read ingredient lists of your favorite foods.
You’ll be surprised over the amount of “hidden” sugars. Any ingredient that ends in “ose” is a sugar.
Trans fats can appear under various names on ingredient lists. Common names include:
1. Partially Hydrogenated Oils: The primary source of industrial trans fats.
2. Hydrogenated Oils: May also contain trans fats, though less than partially hydrogenated oils.
3. Vegetable Shortening: Often contains trans fats unless specified as trans fat-free.
4. Margarin: Some margarine products contain trans fats, though many have been reformulated.
5. Fully Hydrogenated Oils: These are typically low in trans fats but can still be present in some products.
Also avoid anything with “interesterified” fat in it.
Always check labels carefully and choose products that list “no trans fats” or “0 grams of trans fats” to avoid these harmful fats.
Calcium score is very predictive of the presence of coronary heart disease.
Calcium score is calculated using a CT scanner without contrast dye.
The test takes about 15 minutes and shows only the amount of calcified or hard plaque.
It does not show the soft or unstable plaque deposits.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

4 Jaw Exercises for TMJ Relief by a Facial Pain Expert

A facial pain and TMJ disorder expert describes four jaw exercises for facial pain that are comfortable to perform.
TMJ disorder (aka TMD) causes quite a few symptoms, but among the most common is pain, including that in the face.
Before beginning these exercises, you should have a diagnosis of TMJ disorder rather than just assuming you have this common problem.
“The following exercises are often helpful to patients with facial pain,” says Donald R. Tanenbaum, DDS, MPH, a board certified TMJ and orofacial pain specialist, and author of “Doctor, Why Does My Face Still Ache.”
These jaw exercises for facial pain do not represent the full scope of jaw exercises available, adds Dr. Tanenbaum, but these are a great start if you’ve been suffering from facial pain.
Very important: Don’t hold your breath; breathe normally as you perform these movements. There should not be any pain while doing them.
Jaw Exercise 1
Goal: Release tension in jaw-closing muscles
Place your thumb directly under your chin. Place your tongue on the roof of your mouth, halfway back.
Attempt to open your mouth against gentle thumb resistance, as your tongue is kept in contact with the roof of your mouth.
Resist for 3-4 seconds without letting your jaw reach the maximum open position. Repeat 6 times.
Jaw Exercise 2
Goal: Help coordination of muscles that move jaw from side to side
Take a tongue depressor and gently rest it between your upper and lower teeth.
Swing your jaw to the right, gliding on the tongue blade, and feel the resistance. Hold it for 3-4 seconds. Repeat on the opposite side. Do 10 repetitions of both.
Jaw Exercise 3
Goal: Stretch jaw-closing muscles
While sitting down, place your left elbow on a table and lean your forehead into the palm of your hand.
With the index and middle fingers of your right hand, pull down on the lower front teeth to open the jaw until you feel a stretch in your facial muscles. Hold for 3-4 seconds, release, and repeat 10 times.
Jaw Exercise 4
Goal: Limit forward movement of jaw on mouth opening
Place your tongue on the roof of your mouth, halfway back. Open your mouth in front of a mirror.
Try to open in a straight line. Hold in a limited open position for 5 seconds. Release. Repeat 5-10 times.
Be consistent with these exercises, and the pain situation from your TMJ disorder should improve.

Dr. Tanenbaum’s practice focuses on facial pain, TMJ disorder and sleep-related breathing disorders. He is the past president of the American Academy of Orofacial Pain and takes a multidisciplinary approach to his patients’ care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/michaelheim

Is Dizziness from Exercise Different than from Anxiety?

Anxiety can cause you to feel dizzy, and so can exercise.
There are different kinds of dizziness, and each has different causes.
Anxiety is a common cause of dizziness.
However, if you feel dizzy after or during exercise, this can be caused by 1) Lack of nourishment; low blood sugar, or 2) The actual exercise itself, such as pivoting ‘round and ‘round on a stepper.
After all, the dizziness from anxiety is triggered by the rapid breathing that anxiety causes.
However, exercise, too, causes rapid breathing, but normally, a person will not get dizzy from exercise.
I’m a former certified personal trainer and rarely did my clients report feeling dizzy during or after exercise.
The few times this has happened involved clients who hardly ate anything the entire day prior to their exercise session with me.
Why would rapid breathing from anxiety leads to dizziness, and why would rapid breathing from exercise not lead to it?
“When people exercise they breathe rapidly because their muscles require more oxygen, and they also need to breathe out the excess carbon dioxide that is produced during exercise,” explains Peter Swanljung, MD, chief of psychiatry at the Malvern Institute in Willow Grove, PA.
“So the increased breathing is a result of the body functioning appropriately in response to exercise.
“When someone is anxious, they are breathing more rapidly than the body needs them to, and thereby are releasing too much carbon dioxide, which can cause the pH of the blood to rise and cause a constriction of the blood vessels in the brain, leading to a dizzy sensation.”
There are many other causes, such as premenstrual syndrome, and quickly rising to a standing position after being seated for a while.
A very pervasive cause is prescription medications, such as statins and antidepressants.
And of course, pregnancy can cause the sensation as well. Sometimes, unknown causes are at play.
In general, for the most part, if you feel dizzy, this is no cause for alarm.
Often, you know what the cause is right then and there: Are you premenstrual?
Did you just quickly stand up from a seated position? Have you not eaten anything all day?
Did you just try a new dance move that required some spinning?
Are you ill from a “bug” or the flu? Did you recently bang your head?
Are you on a new medication?
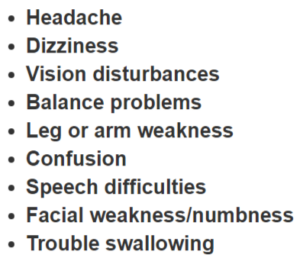
Rarely, dizziness is a sign of serious trouble, such as a transient ischemic attack.
A TIA is recognized by the medical establishment as an emergency situation that signals the possibility of a full-blown stroke in the near future.
However, the dizziness of a TIA is usually accompanied by any of the symptoms listed below.
 Dr. Swanljung is the former medical director of the general adult unit at Friends Hospital in Philadelphia and treats a variety of psychiatric conditions.
Dr. Swanljung is the former medical director of the general adult unit at Friends Hospital in Philadelphia and treats a variety of psychiatric conditions.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}