

Why Does My Heart Flutter After Eating?

“There are many thoughts as to why one can experience palpitations after a meal,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
Sometimes the palpitations are described as a “fluttering” heartbeat.
Dr. Waissbluth continues, “One may ingest caffeine or alcohol during the meal and these often cause palpitations.
“Also, one may have a specific food sensitivity which can be mild and manifest in many different ways – such as MSG or shellfish or gluten – and one of the manifestations is frequently palpitations.
“Also, it is possible that the esophagus or stomach could be irritated – people often have esophagitis or gastritis without really knowing it, and eating may irritate their GI tract further – causing angst and discomfort and then palpitations.”
Causes of a fluttering heart after eating continue…
“Also, it is important to note that after you eat, blood flow is automatically redirected away from the muscles and towards the stomach and intestines,” explains Dr. Waissbluth.
“This change can be quite dramatic after a large meal, and the change can lead to people ‘feeling’ their hearts beating differently.”
The fluttering heart after a meal can be mental in origin.
“Occasionally mealtimes can be anxiety provoking for a variety of reasons, and anxiety is a common cause of palpitations.”
When your heart flutters after eating, does this suggest a serious cardiac problem?
Dr. Waissbluth says, “Palpitations are typically not serious, but they can represent a more serious issue – especially if one experiences other symptoms with them – like chest pain, shortness of breath or dizziness.
“It is always recommended to go see your doctor if you have palpitations just to make sure everything is okay.
“The best way to improve palpitations is to try and remove the cause – which takes some figuring out – and oftentimes there is no cause – they ‘just happen.’”
Reducing that fluttering heartbeat may mean elimination of alcohol or caffeine.
And for others it will require avoidance of stress at mealtime. Put away the smartphone and financial reports.
Tell yourself you won’t think about your bills. Just relax and enjoy your meal.
Avoid if possible eating with the so-called toxic people in your life.
“Assuming there is no worrisome underlying heart disease that needs addressed, there are some medicines people can take to try and diminish the sensations/palpitations,” says Dr. Waissbluth.
“But remember, they have side effects, and sometimes the side effects are worse than the palpitations.”

Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Orawan Pattarawimonchai

How Much Olive Oil a Day Is Too Much?

Here’s what a cardiologist/heart surgeon has to say about how much olive oil is too much in a day.
After discovering a super easy way to get more olive oil in my daily diet without cooking it or tasting it, I wondered just how much olive oil in a day is safe—and is there a point where the quantity becomes more adverse?
“There is no reasonable answer to that question, as it has no context…what else is the person eating, etc.,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
“Navigating the modern food world properly is about understanding what you’re eating. Olive oil contains a lot of fat but it is mostly unsaturated fat.
“The recommendations from various governing bodies are that adults consume approximately 20-30% of their daily calories from fat – of which 2/3 should be unsaturated and 1/3 saturated.
“Fat is a necessary nutrient. If one is eating 2,000 calories a day, then 25% of those from fat would equal 500 calories from fat.
“Fat contains 9 calories/gram so that comes out to about 55 grams of fat allowable per day.
“1/3 of that is about 18.3 grams, so 18.3 grams of saturated fat allowable per day in a 2,000 calorie diet. 2/3 is about 36.6 grams, so 36.6 grams of unsaturated fat per day in the 2,000 calorie diet.
“I personally recommend to my patients that only 20% of their calories come from fat.
“So these numbers would lessen somewhat for my 2,000 calorie a day patient.”
Olive Oil in a Day: How Much?
Dr. Waissbluth continues, “Back to olive oil – 1 tablespoon contains about 14 grams of fat ~ 2 saturated and 12 unsaturated.
“If you ate 9 tablespoons you’d get your 18 grams of saturated fat in for the day but way overshoot your unsaturated.
“And if you ate nine tablespoons you ought not have any other sources of saturated fat in your day.
“If you eat 1 tablespoon you get 2 and 12 respectively and would be lacking in your fat intake for the day – need to make it up elsewhere.
“However, remember, these numbers are not hard and fast rules. They are guidelines.
“If you eat 30 grams of saturated fat one day, that is not the end of the world – you simply curtail your sat fat intake somewhat for the next few days.
“Drinking olive oil is unreasonable – what IS reasonable is to include extra virgin olive oil as part of a diverse predominantly plant based diet and to understand macronutrients way better than the average person currently does.
“It is simply necessary to be able to exist at one’s healthiest, given the food environment/era we were born into.”
The closer food is to nature, the better it is for you. That’s the general rule.
An apple is better than apple sauce is better than apple juice is better than apple pie.
As for easily getting uncooked olive oil into your diet without tasting it, put one tablespoon into your protein drink or fruit smoothie. You will NOT taste it!

Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Is a Resting Pulse of 100-105 Bad?
If your resting heart rate is 100 to 105, you’d better read this article to find out what the bad news is.
The straight question is:
Can a resting heart rate of 100 to 105 beats per minute be harmful to the heart or in some way be tied to a future health ailment?
“Yes – there is emerging evidence that higher resting heart rates correlate with increased cardiovascular risk,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
Dr. Waissbluth continues, “There are many risk factors that influence one’s risk of cardiovascular disease and they all have a cumulative effect.”
If your resting pulse tends to be between 100 and 105, there are things you can do to lower it, but you’ll probably need some patience; don’t expect the lowering to occur overnight.
First off, stop smoking if you smoke. Smoking accelerates resting pulse. This speeding up does NOT strengthen the heart.

Shutterstock/Bogdan Vija
However, the elevated heart rate that comes from structured exercise does improve the heart.
Aerobic exercise three times a week, and strength training on other days, will lower a fast resting pulse.
Cardio exercise, though, is far more effective as long as it’s done consistently and gets your pulse up for extended periods.
Aerobics workouts can be any of the following: dance or step class, “cardio kickboxing,” any kind of cardio machine, brisk walking, hiking, jogging and inline skating.
Tip: If you use a treadmill, do NOT hold on. Pump your arms.

Consistency in your exercise is crucial: three times a week, week after week, month after month — for the rest of your life.
Two of these three cardio workouts should be of the interval training type: alternating brief high exertion with casual recovery periods.
Interval training should be high intensity or medium/high intensity for best results.
Strength training should include many intense routines that get your heart rate up like heavy kettlebell swings, deadlifts and squats, but the interval cardio training will have the much greater impact on lowering a fast resting heart rate.
Another way to knock down that resting pulse of 100 to 105 is to eliminate excessive sitting throughout the day.
On TV commercial breaks, walk around. Always walk about when on the phone.
A resting pulse in the low 100s is nothing to sneeze at.
Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Palpitations During Bowel Movements: Causes, Solutions

Yes, palpitations CAN occur as a result of a bowel movement, and a cardiologist explains why pooping can make you feel as though your heart skipped a beat.
“Anything that causes pain or anxiety can cause palpitations,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
“And if there is a big hard painful poop, this can in turn cause palpitations.”
The pooping itself usually does not cause the palpitations in a direct fashion.
But when having a bowel movement, some people develop anxiety — for a number of reasons.
One of them might be fear of developing a hemorrhoid. Or, it could be fear of colon cancer.
They are driven to inspect their poops with every movement, afraid that the next inspection is going to reveal blood or some other concerning feature.
Another source of anxiety could be that of having a big bowel movement in a public restroom — while someone is in the stall right next to you.
Or maybe you’re in a restaurant bathroom and you’re worried that someone in your party — wondering what’s taking you so long — is going to walk into the john any moment calling out your name. Let the palpitations begin!
Dr. Waissbluth adds, “There are also transient shifts in blood flow during bowel movements which, for people very sensitive to their heartbeats, can lead to ‘feeling’ more heartbeats.
“Also, bearing down too much can alter the return of blood to the heart and cause various changes in heart rate as well, and this too can lead to palpitations.”
Bearing down refers to holding your breath as you push to get a tough poop out.
Try not to hold your breath. Instead, concentrate on exhaling during the push.
Holding your breath during such an action will raise blood pressure.
Is there a way to prevent or reduce palpitations during a bowel movement?
Dr. Waissbluth says, “Eat more fiber, bear down less, enjoy the poop by golly.”
One medium apple = five grams of fiber. One medium banana = three grams.
One tablespoon of chia seeds, which you can sprinkle in salads and rice, contains three grams.
Do Not Worry About Palpitations During Pooping
“There is typically nothing to worry about, as most palpitations are benign,” says Dr. Waissbluth.
“But you never know if there is an underlying heart issue, so always check with your doctor, as some simple noninvasive testing can get to the answer quickly and easily.”
Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, jcomp

Pulled Chest Muscle vs. Heart Problem

A cardiologist addresses whether a pulled chest muscle has different features than a heart problem or angina and vice versa.
A pulled or strained chest muscle is no picnic to have. It can hurt.
And sometimes, the discomfort doesn’t kick in till the day after a chest workout—making it, in a way, seem less likely connected to your bench pressing, pushups or whatever.
(Though any fitness aficionado would be very familiar with delayed onset muscle soreness.)
Differences Between Strained Chest Muscle and Cardiac Pain, Angina
“Musculoskeletal chest pain tends to be quite different from worrisome heart pain,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
Dr. Waissbluth continues, “Musculoskeletal chest pains almost always change with physical movement of the chest wall either from breathing or moving one’s arms or body.
“This causes tension on the actual muscles or tendons or ligaments or joints that are inflamed and makes them hurt.”
This is a hallmark feature of chest muscle soreness.
Like any sore or strained muscle, the pain will fluctuate or be aggravated with movement.
“Also, musculoskeletal chest pains are often fleeting – lasting a few seconds at most –and go away when the movement is over.”
Angina doesn’t last for three seconds.
Pay attention to your movements. What motions did you carry out just before that fleeting “chest pain”?
The offending motion could have even been committed while you were seated—simply twisting in your chair, pressing a hand against the armrest, may be all it takes to buzz the strained chest muscle.
“They are rarely accompanied by other symptoms and typically don’t radiate anywhere else,” says Dr. Waissbluth, referring to musculoskeletal pain.
If you seemingly have persistent chest pain that you suspect is from a gym workout, pay very close attention to your breathing.
You may find that the pain surfaces only at the bottom of an exhalation or at the top of an inhalation, but it seems as though the chest pain is persistent or constant because you’re taking breaths every several seconds.
Take an exaggerated exhalation or inhalation to see if either bring out the discomfort.
Hold your breath to see if the discomfort vanishes!
Holding your breath won’t make angina or other heart pain vanish!
“Chest pain from heart problems, on the other hand, almost never changes with breathing or moving around, is usually in the middle of the chest or left sided, often radiates to the left arm and/or neck and/or jaw and/or shoulder and/or back, is often associated with shortness of breath, nausea and/or sweating, and lasts typically minutes or longer,” explains Dr. Waissbluth.
This isn’t to say, however, that angina can’t ever present as just chest pain only or right-side dominant.
But remember, angina or cardiac pain won’t fluctuate, improve or worsen with changes in breathing and body position.
Dr. Waissbluth continues, “Whereas musculoskeletal pains change with sitting in place and moving one’s torso or arms or taking a deep breath, it is actual physical exertion such as climbing stairs or walking up a hill or carrying something that can precipitate chest pain from a heart problem.”
Gee, how could that sudden “chest pain” while you’re sitting at your computer (when your oxygen demands are thus very low) be from a heart problem when just yesterday you did 50-pound kettlebell swings and 6 RM bench presses (huge oxygen demands) without incident?

Shutterstock/Jasminko Ibrakovic
“But you don’t need to move at all [trot up stairs, shovel snow, lift heavy box, run on treadmill] to have chest pain from a heart problem – as if a plaque ruptures and causes a heart attack while you’re sleeping or watching TV, you can have typical heart chest pain just lying or sitting there.”
Of course, chest pain from a plaque rupture won’t be fleeting.
People who’ve suffered plaque ruptures will tell you that the pain didn’t get better or subside; it persisted, perhaps became worse, and was (most very likely) accompanied by other frightening symptoms such as shortness of breath and profuse sweating.
Dr. Waissbluth adds, “However there is no absolute rule! These are guidelines. Any chest pain of any quality should be reported to your doctor to figure out.”
To non-invasively find out if you have an abnormal amount of soft plaque in your coronary arteries (the type that can rupture), you’d have to undergo a magnetic resonance angiogram — and this procedure is not given to asymptomatic people as a screening tool for heart disease.
You can kick back soft plaque buildup by cutting back (and a LOT, not a little) on processed foods!
As for chest muscle pain, make a habit of warming up generously prior to chest routines, and keep in mind that back routines can aggravate chest muscles.
Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/staras

Coconut Saturated Fats vs. Meat Sat Fats

A heart specialist addresses whether coconut oil’s saturated fats are as bad as those from meat.
There’s a lot of online content touting the health virtues of coconut oil, even though it’s loaded with saturated fats.
Proponents of coconut oil and shreds say that the sat fats are of a different (and healthier) molecular structure than those that come from beef and other types of meat.
“Coconut oil is not as good as current marketers try to make it out to be and not as awful as once thought,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
Dr. Waissbluth continues, “The ‘bad’ coconut oil from days gone by was typically refined – bleached and partially hydrogenated – and this type has multiple unpleasant health effects – as do most manmade processed foods.”
This means that jar of “refined” coconut oil sitting on your shelf is bad news!
In addition to the trans fats of the partial hydrogenation process, the refined version often has sodium hydroxide added to extend shelf life.
The refining process may also involve chemical solvents.
“The modern ‘good’ coconut oil is virgin coconut oil – untouched by man [unrefined] – and even though it is predominantly saturated fat – over 90% – most of these are medium chain triglycerides which are processed differently [once inside the body] than the long chain ones (which are found in most other vegetable oils and almost all animal products),” explains Dr. Waissbluth.
Buy the unrefined version, even if the solidified oil looks clumpy inside the jar.
“These medium chain TGs have been postulated to have some beneficial effects and have shown very modest benefit in small trials and animal studies,” says Dr. Waissbluth.
“However, there is no definitive data which leads any health professional who is not being paid by a coconut oil seller/reseller to recommend virgin coconut oil be used any more than sparingly in any given diet.
“There is no good long-term data on humans that show cardiovascular benefit. Period.”
This isn’t welcome news for those of you who are hooked on raw chocolate coconut balls sweetened with dates and/or Stevia — seemingly a great replacement for the standard candy bar and especially a more processed item like brownies and cake.
If you’re feeling your way around the saturated fats of coconut oil vs. meats and just don’t know what to do, one thing that will help make things a little clearer is to get your cholesterol profile regularly checked.
Changes in diet can rapidly alter your lipid profile.
Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, Racool_studio
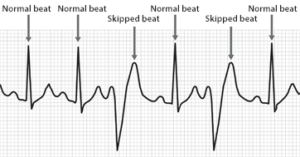
How Does Stress Cause a “Skipped” Heartbeat?
A heart surgeon explains how stress can cause a “skipped” heartbeat.
Keep in mind that what may feel like your heart skipping a beat isn’t necessarily actually that at all, but rather, the next beat occurs so close to the previous one, that this leaves a gap before the next beat after that, creating the illusion that your heart literally skipped a beat.
“Stress causes increased heart rate and blood pressure by increasing the release of adrenalin and adrenalin-like substances in the body,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
Dr. Waissbluth continues, “Adrenalin increases heart rate and blood pressure which can lead to abnormal or fast heart rhythms along with the sensation of skipped beats and palpitations.”
Adrenalin and like-hormones are the so-called “fight or flee” hormones. They prepare your body for an encounter with danger.
The body, however, doesn’t know the difference between the dangers that primitive man had to face (an encounter with a wild boar) and the “dangers” that industrialized people must face (opening the letter that has your mammogram results).
The chemical fear response in the body is the same in either case.
To put it in layman’s terms, these hormones can trip things up, leading to a momentary erratic heart rhythm, what is often called a palpitation, or a thumping or fluttering heartbeat.
There’s a lot of truth to that age-old saying, “My heart skipped a beat when I found out I owed so much in taxes!”
Dr. Waissbluth has been in practice for 25+ years and is board certified in interventional cardiology and cardiovascular diseases. He is founder of Eat Tank, an educational nutrition initiative that provides simple tools and practical knowledge for better understanding food.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Bench Press vs. Weighted Vest Pushups

Here’s the comparison between the bench press and weighted vest pushups.
One of my personal-training clients some years ago asked me which was better: bench press or weighted vest pushups.
What are your goals? Do you want to tone your arms, shoulders and chest? Weighted vest pushups will do the trick, but so will bench pressing.
For toning, both get the job done, and one is not really any better than the other as far as results, though the advantage of weighted vest pushups is that you can do them at home in a limited space.
If you want to build impressive chest muscle, I recommend the bench press. It’s straightforward and allows you to work towards significant weight loads.
One argument against the weighted vest pushup is that it limits the progressive component.
However, weighted vests are now sold that can hold up to 200 pounds.
Furthermore, for beginners, it will be quite some time before they get up in weight load anyways.
Nevertheless, fussing around with loading up a vest could be a turn-off to many people, whereas loading a bar for the bench press is fast and easy.

If you want to gain a lot of strength in your upper body, again, the bench press is the better choice.
Ultimately, for those gunning for getting as strong as possible, the bench press offers no limits in how much you can load up the barbell.
You might be thinking that pushups can be progressed by doing them one-handed, by propping the feet on a stool, by clapping in between, etc.
But the moment you begin doing things like this, you change the dynamics of the movement.
For instance, a one-handed pushup is no longer primarily a force production movement.
It’s now more of a balance and core movement mixed into the force component (though a textbook military pushup indeed involves core recruitment, but not as much as the one-handed version).
Clapping in between adds a jarring element to the shoulder tendons that many people may not take well to, whereas the bench press does not involve this kind of jarring impact to the shoulder tendons.
Elevating the feet makes a pushup more difficult, but that’s because elevating the feet diverts more of the recruitment to the shoulder muscles (meaning less of it to the stronger chest muscles), hence making the movement harder.
But while you’ve just made it harder, you’ve subtracted workload from your chest. Is that what you want if you want a bigger and/or stronger chest?
By the way, don’t think for a moment that performing pushups with a heavy weighted vest will help you a lot with your bench press. It will do squat (no pun intended). And vice versa.
Though the pushup appears to be an inverted bench press, it does not carry over to the bench press. And again, vice versa.
One more element that can’t be overlooked: The bench press allows you to work with a spotter.
On the other hand, you don’t have to worry about getting pinned by a too-heavy barbell when doing pushups.
So why not have both exercises in your program? Who says you must choose?
Start with the bench press, then maybe do the weighted vest pushups as your second chest routine of the session.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

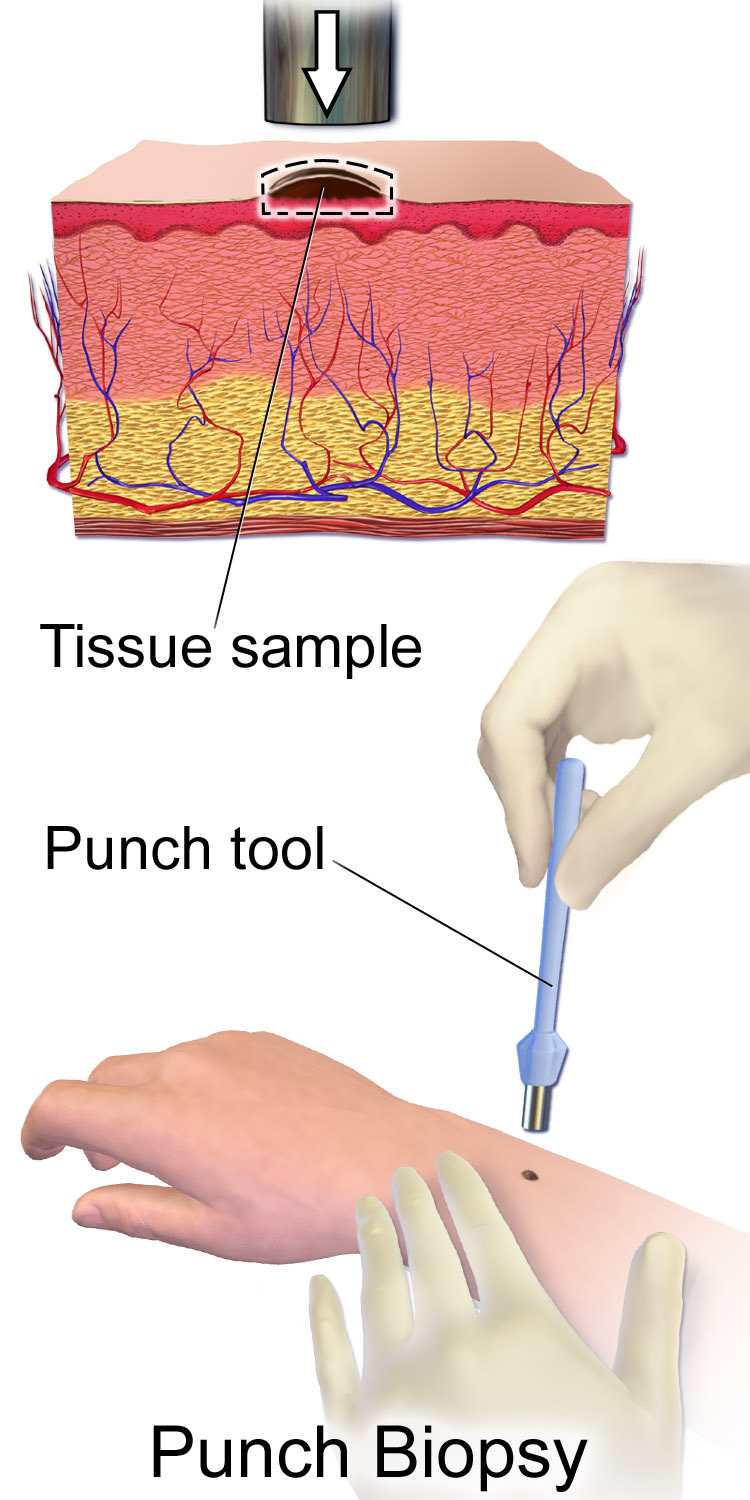
Does a Punch Biopsy for Mole Removal Hurt?

Here’s why a punch biopsy for a mole removal does NOT hurt.
You don’t need a doctor to tell you that having a mole removed via punch biopsy does not hurt. I’ve had two of these.
Actually, one of the punch biopsies was done on a harmless skin barnacle (I had requested the procedure just to play safe, because the dermatologist didn’t sound 100 percent sure that the lesion was a skin barnacle).
Anyways, the actual punch technique itself does not hurt. Prior to performing the punch biopsy, the dermatologist will anesthetize the area, which of course requires a needle to inject the anesthetic.
But in both cases, I did not perceive true pain, like the kind of pain you feel when you accidentally get pricked by a needle.
If you sew or otherwise handle needles and have accidentally gotten pricked, trust me, the anesthetizing injection feels nothing like that.
Once the area is numbed, you will not feel the “punch.” A punch biopsy is when a margin of surrounding tissue which includes below the surface of the mole is removed. As a result, stitches are necessary.
There is no pain, or at least, in my two cases there wasn’t, after the numbing drug wears off.
It doesn’t even sting or burn. In fact, the only problem I had was irritation from the adhesive of the Band-Aid.
Do not fear having a punch biopsy performed for mole removal. It does not hurt.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: BruceBlaus

Breast Density Cancer Danger: Truth or Hype?

Dense breast tissue is a risk factor for breast cancer, but there’s another big problem with dense breasts: Mammograms are harder to read.
So though there may be inconsistent research findings regarding just how much of a risk factor for breast cancer that dense tissue creates, we can’t exactly sweep under the rug the fact that dense tissue in breasts can hide a malignant tumor.
“Mammographic density is referring to the ratio of breast tissue to fat on a mammogram image,” says Jennifer Hartman, a clinical nurse practitioner specializing in breast health, women’s health and cancer genetics.
“When looking at a mammogram image, fat appears dark and breast tissue is white.
“When you have dense breast tissue your mammogram image will appear with more white patchy areas than dark areas.
“Increased breast density on mammography is a problem for two reasons.
“First, breast cancer can often appear as white masses on mammograms, so if your image already has dense white patches, it makes it more difficult to find a white breast cancer nodule.
“The more dense you are, the greater the chance a small breast cancer could be missed.
“3D mammography (tomosynthesis) is definitely much better at cutting through those dense areas to find cancer than traditional 2D mammography, but it is still not perfect.
“Second, increased breast density has been associated with an increased risk of breast cancer.
“These concerns have led to 38 states currently [as of 2023] requiring that we notify patients of their breast density so they can be aware of these risks.
“Any woman with dense breast tissue should talk to their healthcare provider about their options which may include education, risk assessment and additional imaging.”
Striking Points to Consider Regarding Dense Breasts
• Body weight does not determine level of breast density or fattiness.
• Neither exercise, dietary habits, weight loss or weight gain will affect how fatty or how dense a woman’s breasts are. Breast composition is luck or un-luck of the genetic draw.
• Size, shape, feel or “perkiness” of breasts is not predictive of how fatty or dense they are.
• Only a mammogram can reveal whether breasts are mostly fatty; have scattered density; are heterogenously dense; or are extremely dense.
What should you do if you learn your breasts are dense?
It’s strongly advised to trade the 2D mammograms for the 3D (tomosynthesis).
If your health plan doesn’t provide 3D technology, then don’t let that stop you; find an independent imaging clinic and get the tomosynthesis.
Yes, you’ll pay out of pocket, but your breast health is worth every penny. So is your peace of mind.
You may also want to consider annual whole-breast screening ultrasounds.
If you must get these from an independent clinic and pay out of pocket, then DO SO.
You may need authorization from your doctor, though.
Simply inform your doctor that you have dense breasts and want to be extra vigilant.
Do not be “afraid” to request your doctor’s authorization — which should be in writing and faxed over to the clinic.
What does a “tomo” screening feel like?
I’ve had many. They feel the same as the 2D version.
Think of tomosynthesis this way: A 2D mammogram is like standing in one spot at the edge of a forest and, from that position, looking inside the woods to find a bird perched in a tree.
But tomosynthesis has you flying above the forest to look for the bird!
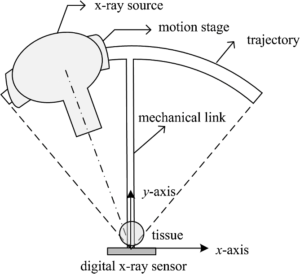
Tomosynthesis
As for the ultrasound as an additional surveillance, the whole-breast screening ultrasound is very simple from the patient’s perspective: Just lie there while the technician places the device over your breasts.
A negative 3D mammogram and breast ultrasound in the same year will be extremely reassuring!



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}