
How Long It Takes Good Diet to Lower Bad Cholesterol
Do you think you’re too old to improve your diet for your cholesterol because it’ll take too long to kick in? Guess what: you’re wrong.
“Any blood work that is obtained on an individual can be viewed as a snapshot in time,” says Richard Kelley, MD, a practicing physician in Texas for 20+ years, and author of “The Fitness Response,” “The Three-Hour Appetite” and the ebook, “The Fitness Response ‘Diet’ for Women.”
He continues, “Consequently, specific lab values, regardless of what they are, can often vary from hour to hour and day to day.
“Though lipid and cholesterol testing is usually done at intervals of several weeks between panels, depending on what a given practitioner is interested in looking at, I have had the opportunity on many occasions to observe repeated studies of LDL and other components of the lipid panel, within days of a patient changing to a cleaner form of diet, and have been able to observe improvement in LDL within a matter of days.”
LDL, the “bad cholesterol,” stands for low density lipoprotein, and you don’t want this number getting above 150.
It’s possible to have a very low triglyceride number (the lower, the better) at the same time that the LDL is on the high side.
Don’t underestimate the power of a better diet in lowering bad cholesterol, regardless of your age.
Dr. Kelley continues, “We know, without a doubt, that in patients who have no predisposition to elevated triglyceride or LDL cholesterol, these values can be elevated or show improvement, sometimes within a matter of two to three days, to varying degree, with simple changes which improve one’s diet.”
As one loses weight from an improved diet, it’s not surprising for medical professionals to observe marked improvements in cholesterol and lipid values, even normalization of these values, adds Dr. Kelley.
If you’re worried about an LDL value that’s increased or is already over 150, the best diet to lower bad cholesterol is one that severely restricts processed foods.
Avoiding buying food in the center of the supermarket right off the bat will go a long way at lowering bad cholesterol; foods that are in the centers of grocery stores tend to be the most processed (with the exception of the bakery department which is typically in the perimeter).
To lower LDL bad cholesterol through diet, avoid the store’s bakery department, increase consumption of raw vegetables, eat more fruit, eliminate beef from grain fed sources (eat only wild game or grass fed beef), eat salmon/tuna/scallops/halibut several times a week, eliminate fast food products, and eat nuts and seeds.
 Richard Kelley, MD, is an author, speaker, fitness expert and transformation coach.
Richard Kelley, MD, is an author, speaker, fitness expert and transformation coach.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can Green Vomit Mean Cancer?

Do you fear that the green in your vomit means cancer?
Perhaps you’ve upchucked lately and couldn’t help notice that the color of your vomit was actually green. Now that can sure be unsettling.
However, this green in your vomit doesn’t mean that anything is seriously wrong with you such as cancer.
In fact, a truly serious sign is when you see red in your vomit — from blood.
But GREEN?
Don’t fret; it’s nothing to worry about. I myself have never seen green in my own throw-up, but I understand that this can frighten people who do happen to notice this odd color.
Gastroenterology is the medical specialty that deals with the gastrointestinal tract (intestines and stomach organ).
“Green color in vomit can occur either because of green food, or more commonly from vomiting bile from the intestine which has a yellow/green appearance,” says Edward Cruz Paredez, MD, a board certified gastroenterologist based in La Jolla, CA.
No cancer.
If you’ve noticed that your vomit is green, ask yourself if you’ve recently eaten broccoli, cucumbers, kale, spinach or other such produce.

Dr. Paredez continues, “Yellow/green bile is made in the liver out of bile salts and pigments/colors.
“These salts aid in digestion and are secreted into the intestine just past the stomach to mix with food contents from the stomach.
“Vomiting green bile can occur in a number of instances and is not specific for ‘how sick’ someone is or what the cause of vomiting is.
“Most people aren’t accustomed at seeing their own vomit and panic when they see the green color, even if they know it is from bile.”
So when you see this hue in the content that you just upchucked, it’s actually the bile that comes from the liver.
“Vomiting green bile often alarms people since they may not have eaten anything green and they do not realize that the body makes bile continuously for us to digest our food,” says Dr. Paredez.
As mentioned before, blood in the vomit warrants a trip to the doctor for evaluation.
However, blood can also manifest as brown, appearing like coffee grounds.
When you throw up, don’t be afraid to take a good look at its contents or color.
If throwing up is accompanied by any other symptoms, see your physician.
So you now know that green vomitus is not a sign of cancer.
However, you should investigate why you’re puking in the first place.

Dr. Paredez has been named a Top Doctor by San Diego Magazine and has also received a 2016 “People Love Us on Yelp” Award.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

What It Costs to Treat Dog Injuries from Exercise

The cost of treating a dog’s injuries–the kind from exercise — is not the least bit cheap.
It’s advised that you have a “dog injury fund” in a second bank account!
When it comes to how much it costs to treat dog injuries, it depends on several factors, says Dr. Jules Benson, BVSc, chief veterinary officer with NationwideDVM, a pet insurer company.
- what diagnostics and treatment your veterinarian considers appropriate for the circumstance
- whether there is any follow-up care, pre- or post-operative rehabilitation or complications
- how large your dog is (larger dogs can cost considerably more for medications and surgical procedures)
- and where you live – veterinary prices vary depending on state/area, and some procedures may only be available if you have a specialty veterinarian in your local area.”
Pet Insurance
Dr. Benson points out that a pet insurance plan will reimburse a percentage of the veterinay bill, “minus a deductible – both of which are selected by the policyholder.”
The costs below reflect an average reimbursement for these conditions as of 2012.
Injuries in Dogs–How Much They Cost
Lameness: $478.80
Cruciate ligament tears: $2,107.31
Luxating patella: $1,262.61
Broken nail: $220.52
Lacerations/cuts: $314.99
Heat stroke: $1,168.43
When your dog is getting exercise, it can be difficult to prevent injuries.
Your dog can be bounding out in a field and step on something that sprains its leg or deeply cuts into a paw. It’s something that just might happen no matter how careful you are.

However, one of the injuries on that list can be prevented: heat stroke.
Unless you and your dog are unexpectedly stranded in a desert, there is no reason for a dog to develop heat stroke.
For any physical activity on a hot day, bring plenty of water, and give it to your dog frequently throughout the activity, especially if it’s strenuous like a hike.
In the event that your dog sustains any of these injuries or some other injury via exercise (or some other origin), you should put aside some money every month for a treatment fund.
Even if it’s just $20, this will cover a broken nail in two years.
 Dr. Benson is regularly consulted by many media outlets including ABC, NBC, FOX, The Wall Street Journal and The New York Times to provide pet health advice to pet parents nationwide.
Dr. Benson is regularly consulted by many media outlets including ABC, NBC, FOX, The Wall Street Journal and The New York Times to provide pet health advice to pet parents nationwide.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Local vs. General Anesthesia for Knee Arthroscopy

Which is better for knee arthroscopy: local anesthesia or general?
We all know that general anesthesia comes with far more risks than local, but there are circumstances that call for general anesthesia over local for a knee arthroscopy.
It’s also understandable if the idea of “going completely under” is frightening.
You probably already know that the level of unconsciousness while under general anesthesia is deep enough that the patient cannot be aroused without drugs.
It’s so deep, in fact, that the patient can’t even breathe on their own; they must be intubated: A tube is placed down their throat and breathes for them.
Local vs. General for Knee Arthroscopy
“Local anesthesia is a reasonable consideration assuming the planned procedure is not expected to be extensive or to last longer than 20 to 30 minutes and does not require the use of a tourniquet,” explains Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
“The tourniquet itself may cause pain that will not be adequately addressed by the use of a local anesthetic.”
Knee Arthroscopy
This very common procedure allows the doctor to view a knee joint despite making only a small incision.
Arthroscopy allows the surgeon to diagnose the specific condition and then treat it.
Viewing is done via a little camera (arthroscope) that’s inserted into the joint.
It shows images on a video monitor that guide the surgeon in using thin, miniature surgical instruments – that allow for very small incisions.
The patient enjoys a much faster and less painful recovery than what would occur with invasive surgery to the knee, especially if it were done with general anesthesia.
Be sure to ask your surgeon adequate questions to make sure you understand the precise nature of your condition and why your surgeon — if this is the case — has opted for general anesthesia over local to perform your knee arthroscopy.

Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Stomach Burning from Exercise Caused by Magnesium Deficiency

Have you experienced a burning sensation in your stomach during or right after exercise?
What can cause a burning feeling in your abdomen when you exercise?
“Sit-ups can aggravate a hiatus hernia and lead to reflux or even vomiting,” says Carolyn Dean, MD, ND – Medical Advisory Board Member of the non-profit Nutritional Magnesium Association at nutritionalmagnesium.org.
Acid reflux can cause a burning or aching feeling in the stomach.
Reflux is when acid in the stomach enters into the esophagus (“food pipe”).
However, the discomfort of reflux can still occur in the stomach, not necessarily only in the chest.
“Also, stomach spasms and vomiting can be aggravated by magnesium deficiency…since magnesium makes muscles work properly, allowing calcium to cause muscle contraction and then pushing calcium out of the muscle cells to allow the relaxation phase,” explains Dr. Dean.
“When there is a lack of magnesium, muscle cells in the bronchial tubes can go into spasm, tighten up and cause wheezing and burning and coughing.”

Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/KDdesignphoto

Pancake Breakfast or Skipping Breakfast: Which Is Healthier?

Mmmm, a stack of steaming pancakes drenched in maple syrup and butter for breakfast: Is this healthier than SKIPPING breakfast?
Plenty of research shows that a nutritious morning meal is the most important meal of the day (or maybe the second-most important, if you rank the post-workout meal in the top spot for later-day workouts).
The Research on Breakfast for Kids
- Eating it is linked to lower risk of type 2 diabetes in children (Donin et al).
- Eating it is linked to higher IQ’s in kids (Liu et al).
- Skipping breakfast increases kids’ obesity and cardio-metabolic risk (Eloranta).
- Skipping is associated with reduced learning and reduced attention span in kids (Bennett et al).
And what about adults?
- Fuster et al found that skipping breakfast is associated with hardening of the arteries.
- It can lead to poor food choices for the rest of the day (Auestad et al).
- It may lead to high blood pressure and coronary artery disease (Cahill et al).
Note that some of these negative outcomes are associations rather than direct results.
We can venture to say that people who always pass on breakfast are less likely to be health conscious or put in grueling gym workouts.
Therefore, due to poor overall diet and lack of exercise, they’re more likely to develop type 2 diabetes or cardiovascular disease.
But the direct results, such as poor concentration, can’t be dismissed.
If the only breakfast available were pancakes, would it be better for your body to eat all this white flour, sugar and butter fat than to skip it?
“As a clinician, I am always one to promote eating something for breakfast,” says Amanda A. Kostro Miller, RD, LDN, whose specialties are nutrition counseling, weight loss and medical nutrition therapy.
“When we skip breakfast, we may get really hungry by lunch and overeat at lunch.
“While a pancake breakfast is not the best choice, there are small changes we can make to improve upon the nutritional profile of a pancake breakfast.
“Here are some ways to make a pancake breakfast better:
- Add fruit and/or nuts.
- Make your pancakes whole grain.
- Minimize the syrup.
- Control the amount of butter used.
- Instead of large pancakes, make yourself small/mini pancakes (control the number).
“Many people who don’t eat breakfast tend to have several obstacles that prevent them from actually eating breakfast (e.g., lack of time, don’t know what to make, want to sleep in, not hungry in the morning).
“However, if a client is already eating a breakfast (even pancakes), we can work on small changes to their breakfast to make it healthier.
“As a clinician, these small changes, rather than getting someone to prioritize their time to eat breakfast, can be easier.”
Certainly, a breakfast laden with white flour and sugar will satisfy hunger and prevent overeating at lunchtime.
Then again, if a pancake breakfast isn’t consumed with discrimination, it can have far more calories than overeating at lunch after a skipped breakfast.
A well-managed breakfast of pancakes should stave off poor concentration and reduced learning or impaired productivity in children at school and adults at work, respectively.
But remember, as much as the body wants and needs fuel shortly after it awakens from an overnight fast, if you put junk in your body, it will still be junk. Junk food is junk food.
Don’t give up pancakes if you love them. But make an effort to limit intake and make most of your breakfasts healthier options such as eggs with fruit and yogurt, or a fruit smoothie with a whole grain English muffin topped with a little butter.
 Amanda Kostro Miller has worked with U.S. veterans, people with eating disorders and those with various acute and chronic diseases.
Amanda Kostro Miller has worked with U.S. veterans, people with eating disorders and those with various acute and chronic diseases.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Surgical Hair Restoration: Can You Run Out of Donor Sites?

Ever see those surgical hair restoration infomercials and wonder if the donor follicles can keep up with the hair loss follicles?
In surgical hair restoration, follicles that are not genetically programmed to eventually stop producing are “grafted” onto the sites that have become bald.
If you’ve seen any hair loss infomercials involving surgical solutions, perhaps you’ve wondered what I’ve wondered.
In male pattern baldness, the first areas to “go bald” are the top and top/back of the head.
When this pattern of baldness progresses enough, the man is left with a horseshoe pattern of hair.
In extreme cases, this remaining hair is a thin band encircling the lower portion of his head, just above his ears, revealing significant amount of scalp.
The infomercials show the donor site as the section of hair that’s below the balding area. But won’t this area eventually thin out too?
As follicles from this area are grafted onto the top portion of the patient’s head, seems that if this is done enough, this donor area will thin out.
And because this donor area will thin out if it’s harvested enough, and as the male pattern baldness progresses over many years, won’t the patient be left with hair pretty much only on the top of his head?
“Realistic short and long term results should be discussed, as the balding process is progressive and final results can be unpredictable,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
“Over time the transplanted area may become ‘isolated’ and therefore multiple procedures may be necessary over one’s lifetime to achieve natural results.”
Dr. Gabriel continues that “small areas of donor sites can be taken for hair transplant without any loss of noticeable hair with newer techniques.”
The back of the head is a common donor site (since male pattern baldness begins more towards the top of the head).
Taking follicles from this site will not result in noticeable hair loss, says Dr. Gabriel.
“Even if a larger graft is taken and divided into mini-grafts (not the preferred way), the skin and scalp can stretch and expand, and loss of hair will not be noticed as long as the hair is long enough to cover (or drape over) the donor scar.
“With newer techniques and technologies (i.e., follicular unit extraction), the surgeon can retrieve grafts three to five times from the same area,” explains Dr. Gabriel.
“It’s like harvesting blades of grass from the lawn. If we disperse the harvesting, it will not be noticeable.”
Will grafts grow if they are transplanted in an area that never grew hair?
For instance, suppose a person always had a receding hairline, or, to put it another way, prominent temples with an innately, naturally receding hairline.
If the skin here is healthy (non-scarred and no prior history of radiation), and especially if the patient is a nonsmoker, then this recipient site will be “welcoming to the graft,” says Dr. Gabriel.
He emphasizes that medical problems such as diabetes, vascular and thyroid disease will interfere with results and should be controlled prior to the procedure. Smoking cessation is also critical for better results.
“One can graft near the temple or graft on the forehead to lower the hairline, even though hair never grew there.”
 Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/wavebreakmedia
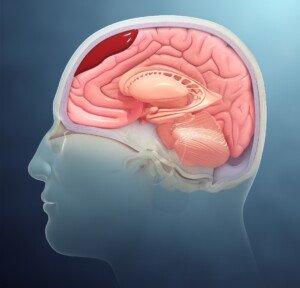
How Many CT Scans Should a Head Trauma Patient Have?
Just how many CT scans are needed if someone has a small brain bleed resulting from a not-so-severe head trauma?
This can be banging their head on the bottom of the bathroom sink after kneeling on the floor and getting up.
Is it possible for a doctor to over-order CT scans in a head trauma patient with a chronic subdural hematoma (slow brain bleed)?
Years ago my mother had seven CT scans in 29 days due to a chronic subdural hematoma.
Certainly, she is not the only person to ever undergo many CT scans of the head in a short period of time.
Concerns of Radiation Exposure of Multiple CT Head Scans over a Short Time Period
What About for Milder Head Trauma?
The January 2013 issue of Neurosurgery has a report that questions the need for repeated CT scans in patients with non-severe brain bleeds.
“The available evidence indicates that it is unnecessary to schedule a repeat CT scan after mild head injury when patients are unchanged or improving neurologically,” says the paper.
In the case of my elderly mother, the diagnosis was chronic subdural hematoma (nowhere near as severe as acute subdural hematoma).
• On 11/28/10 my mother had a CT scan after hitting her head.
• Next day she had another one. Both were normal.
• However, 42 days later (01/09/11) she had another CT scan after awakening with neurological symptoms. That image showed the brain bleed.
• Two days later she had another CT scan following surgical draining of the blood/fluid from her brain.
• About a week later she had another one because she was experiencing new-onset neurological symptoms — that were ultimately attributed to an anti-seizure drug given pre-emptively for the head injury.
On 01/24/11 she had another computerized tomography (scheduled), but this one was based on yet a new set of neurological symptoms (that were soon found to be caused by a recurrence of the brain bleed).
The next day she had yet another CT scan (in the ER) following acute delirium. The ER doctor said the delirium was an adverse reaction to the Medrol Pak (oral steroids) that were prescribed for the injury.
On 01/27/11 she had another imaging following her second surgical draining.
That all seems like a lot of head CT scans, but it’s important to keep ahead of brain bleeds, and to weigh the risk vs. benefits.
It would take many years for radiation exposure to cause adverse effects, if any, and if the patient is already elderly , the concern over radiation becomes smaller.
The standard protocol is to give repeated CT scans after even mild head trauma, since bleeding in the brain can be life threatening or cause permanent neurological damage.
Whether the patient truly needs routine follow-ups based on a timeline, vs. another scan based on symptoms or what the previous scan showed, is up to the treating physician.
The Neurosurgery study authors favor neurological examination as a stronger determinant in treatment changes.
Symptoms, not timelines, should guide the need for CT scans for small slow brain bleeds, says the study.
These findings do not necessarily apply to victims of severe head trauma.
 Dr. Mendi has published several articles in radiology journals and has expertise in MRI, women’s imaging, musculoskeletal, neurological and body imaging.
Dr. Mendi has published several articles in radiology journals and has expertise in MRI, women’s imaging, musculoskeletal, neurological and body imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Pixel-Shot
Source: sciencedaily.com/releases/2013/01/130103113848.htm
Should I Go to ER After Hitting Head on Bathtub?
Hitting your head on a bathtub after falling can cause bleeding in the brain, but should you rush to the ER simply because you bonked your head on the bathtub?
What if you’re fully conscious and “feel fine” afterwards?
Symptoms of the brain bleed may not begin occurring until weeks after you hit your head on the bathtub!
Bathtubs are hard as hell.
I will never forget that distinctive “THUD!” at about 8:45 that morning. I immediately knew what it was and raced up the stairs and into my parents’ bedroom to get to the bathroom, calling for my mother.
She was lying on the floor, head and shoulders propped up against the side of the bathtub. I knew exactly what had happened.
She had passed out while standing and fell, dead weight, to the floor, hitting her head on the bathtub along the way.
She had very severe orthostatic hypotension and was supposed to alert me whenever she got up from a lying or seated position, so that I could prevent the falls when she passed out.
This time she didn’t alert me; I had been snoozing downstairs on the sofa.
My mother was conscious immediately after hitting her head on the bathtub (I was up there in seconds).
I helped her up and examined her head, finding no bump or blood.
My mother wasn’t 100 percent alert, though, because at first she told me she had not hit her head.
I pressed about this, and then she said she had indeed.
She also told me, after I had asked, that she did not have a headache, was not in pain.
I helped her into bed, and all I could think about was a subdural hematoma (brain bleed).
Ever since my mother developed the mysterious orthostatic hypotension, I had feared subdural hematoma from falling and hitting her head; I couldn’t be with her 24 hours a day.
Based on the sound that her head had made when it hit the bathtub, I wasn’t convinced that there wasn’t a bump somewhere on her head — and a ripe condition to trigger a brain bleed.
Check Victim’s Head; Don’t Take Their Word for It
I told her to point to exactly where she’d hit her head on the bathtub.
I pulled away at her hair and, sure enough, there was a section of matted blood on her hair.
“We’re going to the ER!” I announced. “There’s blood on her head!” I told my father.
If someone in the household hits their head on the bathtub and you find them lying on the floor fully conscious, consider taking them to the ER.
“After sustaining head trauma by hitting someone’s head against a bathtub, an urgent medical evaluation may be in order,” says Natasha Fuksina, MD, an internal and integrative medicine specialist who combines traditional and functional medicine to restore health and function.
Dr. Fuksina continues, “An elderly person on multiple medications, including blood thinners (such as Coumadin, Eliquis, Xarelto), can quickly develop a subdural hematoma (bleeding outside of the brain underneath the skull) or bleeding inside of the brain.
“If a person felt faint and dizzy and that resulted in a fall and hitting the head on the bathtub, with or without loss of consciousness, they have to be evaluated in the ER regardless of their age.”
The victim’s description of what happened or “where it hurts” may not be accurate due to compromised mentation.
The CT scan of my mother’s brain was normal, but she was held overnight for observation and a follow-up scan the next morning, which was normal.
I asked the doctor, “Is there a possibility that a few months from now, there could be bleeding in her brain from this?” He said that there was a very “slim” chance.
Six weeks later, following six weeks of normalcy as far as no neurological symptoms, my mother awakened with a blazing headache and significant lower body weakness.
I took her to the ER and sure enough, the CT scan showed a chronic subdural hematoma!
Scientific Animations, CC/BY-SA/Attribution-ShareAlike 4.0 International
Though the initial ER visit results were negative, don’t let this keep you from going to the ER a second time.
And sometimes the bleeding will be evident 24 hours later on that follow-up CT.
Age of the victim plays into this. A brain bleed is far more likely in an elderly person who hits their head on a hard surface like a bathtub from a fall.
It’s way more likely, in fact, when compared to a young adult or even middle-aged person.
“A young person or middle-aged adult will most likely not sustain any life-threatening head injuries from hitting their head on a bathtub,” says Dr. Fuksina.
“If someone develops dizziness and changes in consciousness, then prompt medical attention is still warranted.”
So regardless of age, if there are neurological symptoms, get to the ER!
If the person is elderly but shows no symptoms (nausea, worsening headache, confusion, amnesia, off-balance), get them to the ER, but don’t panic.
Remember, a bathtub is as good as concrete when hitting your head.
 Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Normal CT Scan After Hitting Head: Brain Bleed Can Still Occur
Can Chronic Subdural Hematoma with Symptoms Go Away on Its Own?
Slip & Fall, Hit Head Hard on Concrete: Brain Bleed Prevention
Hit Head? Bleeding in Brain Symptoms Can Occur Six Weeks Later

Really Dry Skin Around Eyes: Causes & Solutions

Dry skin around the eyes is a common problem.
It is not always corrected by simply dabbing on skin lotion or moisturizers.
“Dry skin of the eyelids is frequently referred to as blepharitis (which just means inflammation of the eyelid),” says Dr. Dendy Engelman, a board certified dermatologic surgeon with Manhattan Dermatology & Cosmetic Surgery.
Causes of Dry Skin Around the Eyes
Dr. Engelman explains, “The potential causes of blepharitis are many: allergic contact dermatitis, seborrheic dermatitis, irritant dermatitis, so treatment needs to be catered according to the cause.”
Dermatitis (contact and irritant)
• Keep track of anything that can possibly come in contact with the skin under your eyes throughout the day.
• You’d be surprised at what can end up there that you’d never think of.
• This includes household cleaning agents that are on your fingers — that get transferred to the skin beneath your eyes.
• Other possible culprits are pet dander, cosmetics, hair care products, fragrances and chemicals from the workplace.
• Once you’ve figured out what comes in contact with that area, eliminate them as best you can and see what happens.
Seborrheic Dermatitis
- This common problem involves the sebaceous glands. Not only is dry skin a symptom, but often, the skin flakes, itches and appears as a pinkish patch (sometimes with a tinge of dull orange).
- Do not scratch or rub the affected area no matter how badly it itches.
- Your doctor can prescribe an ointment to rid the problem.
Dr. Engelman continues, “Eye irritation can also be a symptom of ocular rosacea, a subtype of the disorder [rosacea] that can potentially be very serious if allowed to become severe.
“Once a medical cause has been ruled out, a nice OTC option to try to mitigate dryness around the eyes are Ocusoft lid scrubs.
“I recommend patients use these twice daily to help cleanse the delicate eye area.”
 Versed in the latest techniques and technologies, Dr. Engelman provides a wide range of services including fat removal, mole excision, Mohs surgery and skin cancer treatment.
Versed in the latest techniques and technologies, Dr. Engelman provides a wide range of services including fat removal, mole excision, Mohs surgery and skin cancer treatment.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}