

Best Ways for Women to Lose that Potbelly

What’s the best ways for women to lose their potbelly?
So you just cannot get rid of that potbelly?
There are truly best ways for women to get rid of their potbelly, even if they have been trying for a long time to trim that gut.
Belly Bigger than It Should Be for the Rest of Your Body
I’m not talking about obese women here, but rather, smaller women who just happen to have a potbelly — a midsection that’s out of proportion to the rest of their body — one that’s just too plump, given the size of the rest of their physique.
A major mistake that some women make is blaming their paunch on pregnancies.
I don’t mean soon after a pregnancy. Obviously, recovery time and “rebound” time are necessary following giving birth.
But I’ve known women who blame pregnancies of well over a decade ago, even several decades ago, on their plump stomachs.
Interestingly, these women’s potbellies have grown in the years following their last pregnancy!
Don’t blame pregnancies.
A woman should review her exercise habits, especially if she’s over 30.
If a woman has not been strength training, then beginning at around age 30, she starts losing muscle mass.
This slows the metabolism, and guess what the result is: increasing amounts of fat in the belly. And often elsewhere, too.
The more muscle a woman has, the faster her resting metabolic rate.
And the faster the resting metabolic rate, the less stored fat there will be in the belly.
Thus, a very important move for ridding the potbelly is strength training — and hard.
Light weights and high reps won’t cut it — though novices should initially do light weights and a rep range of 12 to 15 to acclimate their sedentary body to this new form of exercise.
But eventually the protocol should be eight to 12 reps, with those last few reps very difficult to complete.

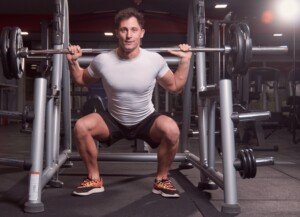
The back squat
Some sets should go to muscle failure: when the muscle being worked, just plain poops out and can’t budge for even one more repetition.
A true eight to 12 rep max means that you’ll feel the effort required from the first few reps.
You should NOT be able to get past 12 reps.
Strength train all the major muscle groups, with emphasis on the upper legs, glutes, back and chest, because the largest muscle groups will burn the most fat — including fat in the belly.

Deep dumbbell squat

Barbell deadlift

Lat pull-down. Freepik.com
This means hard leg workouts will burn fat in the belly; hardworking legs need fuel for recovery from hard exercise.
- Body fat is unused fuel.
- If your belly is loaded with fat, your legs will take from that fat, and hence, you will start losing your potbelly.

Dumbbell deadlift. Shutterstock/Robert Taylor

Bench press. Freepik/master1305
“Won’t lots of crunches trim my stomach?”
Spend minimal time on abdominal exercises. Please, the myth is over: Lots of crunches and sit-ups will NOT get rid of a potbelly.
Potent Fat Burner
In addition to intense strength training, do cardio — high intensity interval type.
This creates an “after burn” that regular long duration cardio doesn’t.
Example: On your favorite cardio machine, instead of setting the controls for a steady duration for 60 minutes, blast out your fastest effort, or use the hardest pedal tension, for one minute.
Then go easy for one minute. Do this back and forth for 20 to 25 minutes straight, two or three times a week on non-strength training days. A woman will start losing her potbelly this way.

What about diet?
“Watch your refined and processed carbohydrate intake if you’re looking to lose that potbelly,” says Sara Artigues, a registered dietician and certified personal trainer out of New Orleans.
“Insulin resistance is a huge health issue that can increase weight, especially around the midsection.
“When you eat too many sugary and processed carbohydrates, they can cause an imbalance in insulin and promote fat storage.
“Cut down on your sodium intake. Sodium causes water retention, so your body holds in excess fluids and can leave you bloated.”
Summary of Best Ways for a Woman to Get Rid of Her Potbelly
Strength train with heavy enough weights to make more than 12 repetitions impossible.
Engage in high intensity interval training.
Try to avoid refined (white flour-based) carbohydrates; fill up on fruits and nuts.
Have a nourishing breakfast.
Don’t go more than three hours without food.
Drink plenty of water throughout the day.
Consider replacing sugary sweets with those sweetened naturally with the herb Stevia — which contains zero calories and can be part of your belly trimming plan.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
 Sara’s training services include fitness/body composition assessments, nutrition planning, customized programs and spin class instruction for a variety of clients.
Sara’s training services include fitness/body composition assessments, nutrition planning, customized programs and spin class instruction for a variety of clients.




Best Strength Training Routines for Elderly: Top 5 Exercises

The best strength training exercises for the elderly are the same for both men and women.
If you’re elderly or of “senior” age, you should strength train — no excuses. This means lift weights.
Elderly women, especially, should lift weights, to help fight off brittle bone disease which they are more at risk for than are men.
If you’re over 65 ask yourself:
- Do I want to dance at the next wedding of a grandchild?
- Or would I rather be pushed in a wheelchair into the reception hall?
Top 5 Strength Training Exercises for Elderly Men and Women
A “top 5” list will vary from one personal trainer or fitness expert to the next.
But usually, there is overlap with at least two types of exercises.
A “top 5” list will also depend on the physical condition of people over 65.
Some are already active (golf, swimming, yoga, hiking), while others are very sedentary and get winded just walking quickly in a parking lot.
Any five of the following strength training exercises are great for the elderly population.
#1) “Bodyweight squats are an excellent strength training routine for seniors because they help increase your lower-body strength allowing you to preserve the vital muscle tissue that decreases with age and inactivity,” says Monica Charlton, a senior exercise specialist and certified Silver Sneakers/personal trainer out of New Orleans.

Bodyweight squat Shutterstock/Dmytro Zinkevych
#2) Standing up from a chair and sitting down for repetitions. Don’t plop down; lower into the chair with control every time. This is sometimes referred to as chair squatting.

BrusBlaus
“The easiest way to ease into bodyweight squats is by doing chair squats,” says Charlton. “This helps you get the correct form while also giving you a chair to help with balance.
“Before going into full-blown squats, you can even start in a seated position and push up, holding the tension for a few seconds, and then go back down. This works your muscles and prepares you for regular squats.”
#3) Pushups, modified to your level, such as knees on floor, or standing pushup in which you’re pushing off a countertop.
“Pushups are still some of the best arm and chest exercises you can do, even as you age,” says Charlton.

You’ll need to first start out with your hands on a countertop, then progress to your knees on the floor, and hopefully, you’ll eventually be able to do a standard pushup. Shutterstock/Straight 8 Photography
“Pushups work the same muscles as the chest press, but it also stretches them and works to stabilize your core muscles to protect your lower back,” says Charlton.
#4) Leg press. “An important way to continue strengthening your muscles is to work them constantly in a sitting up and down motion,” says Charlton.
“A leg press can work for this when done on a lower weight. This motion can help improve strength in the quads, buttocks and hamstrings.”

Leg press. Shutterstock/Wendy M. Simmons
#5) Deadlift. “Deadlifts work wonders for your lower body,” says Charlton. “However, they can be very dangerous when done incorrectly.
“To get the best benefits and avoid injury, a personal trainer should be there to assist and make sure you have the correct form.
“The deadlift motion is used in everyday activities — from picking up grandchildren to moving laundry baskets.
“To be precise with your deadlift, it’s best to start out practicing at home, using your own body weight,” and building up to, say, holding with straight arms in front of you a tray with a few books on it for weight, “and then build up with a professional’s help at the gym.”

Deadlift
#5. Row. “Resistance bands can be very helpful for this when tied to a banister or pole,” says Charlton.
“With your feet planted firmly on the floor, pull the band straight back until your hands reach your sides, and squeeze your shoulder blades.
“For even more resistance, you can increase the distance between you and the pole.”

Row. Shutterstock/Aaron Amat
Loss of muscle, beginning at around age 30, starts occurring in people who don’t do strength training – structured weight-bearing workouts. This muscle loss equates to about five pounds per decade.
So even though an elderly woman may still be able to “fit” into her wedding dress of decades past, her body composition has radically changed if she’s been losing five pounds of muscle every decade!
“Our analyses of current research show that the most important factor in somebody’s function is their strength capacity,” states Mark Peterson, PhD, in a University of Michigan Health System study report.
Older people should strength train at least twice a week.
The best exercises that I just named are all compound strength training moves. At the gym, the bench press can replace pushups, or you can do both.
Squat and Pushup Alternatives
An elderly person who’s strong doing body-weight-only squats, can progress to weighted squats on a Smith machine, or with holding dumbbells or weight plates.
A squat with a barbell across one’s back is certainly not out of reach for the fitter 65+ person whose doctor has cleared them for this.
 Monica Charlton’s personal training services include fitness/body composition assessments, nutrition planning, running programs and customized programs for clients with disabilities or injuries, as well as older and mainstream clients.
Monica Charlton’s personal training services include fitness/body composition assessments, nutrition planning, running programs and customized programs for clients with disabilities or injuries, as well as older and mainstream clients.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2011/03/110331163539.htm



Can You Build Muscle with 20 Repetition Bench Press Workouts?

If you’re struggling with gains it’s time for the 20 reps bench press!
Bench pressing for 20 reps will help bust through ruts in progress.
The bench press is often used as a staple of upper body conditioning. (more…)



What Is a Rack Pull & the Benefits?

What exactly is the rack pull and its benefits?
Rack pulls can do several great things for your body — male or female.
One of its biggest benefits is that it will help you get past plateaus.
What is a Rack Pull?
It’s a variation of the deadlift. Instead of the bottom portion of the movement being on the floor (barbell on floor or touch-and-go to the floor), the bottom is on the bars of a squat rack that are set between knee height (or sometimes even a bit lower) and about mid-thigh height.
This allows one to pull a lot more weight than with the standard floor deadlift.
This style is not to be confused with shoulder shrugging, even though when the bars are set at mid-thigh level, the movement may initially appear to be a form of shoulder shrugging.
The shoulders do not shrug in the rack pull. In fact, if one is able to shrug the shoulders during this exercise, the weight is not heavy enough if you want to create a bullet-proof back and improve your regular deadlift.
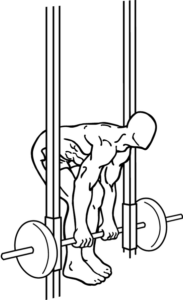
Starting position for a rack pull. Feet should have athletic wear and should be apart. How apart depends on personal preference. Some people space them as they would for a deadlift. Everkinetic, Creative Commons
The primary purpose of the rack pull is to move as much weight as possible, and the limited range of motion — in combination with many major muscle groups getting involved — allows this to happen.
Lifting as much weight as possible is accomplished only when one applies nothing more than the pure deadlift motion — with the adjustment of the bottom portion of the exercise being higher than the floor.

What muscles does the rack pull work?
The rack pull works the same muscle groups as the conventional deadlift, though there is less force absorbed by the legs, since the exerciser doesn’t lower their body as much.
Nevertheless, the legs still get worked with this movement. And I’m talking here about the bent-leg version, which allows you to move more weight than if you were to keep your legs straight.
Rack Pull Benefits
This style of training will contribute to building muscle because it permits one to lift so much more weight.
The higher that the catch bars are set, the more weight that a person can strain and lift with, providing a unique stimulation to the muscle fibers.
The back muscles really get involved, and the fibers will respond accordingly.
The arms, too, take a good beating during a 6-10 rep max of rack pulls. Nobody with scrawny arms is going to rack pull enormous loads.
However, one must have a pretty good grip to get through a blasting set of rack pulls; it would be a shame if one has to quit the set because the wrists and forearms fatigue before the major muscles do.
Some people will perform rack pulls with the bars set literally only several inches from the floor.
This still seems to be more of a pure deadlift than a rack pull, but nevertheless, it allows a person to move more weight.
The exercise can also be done simply as an exercise in and of itself, regardless whether or not one is stuck at any kind of plateau.
It truly is a great exercise and gets the body used to moving tremendous amounts of weight, relative to what it can move with other exercises.
Any person who wants to get huge should include rack pulls–and work towards pulling the most beastly weight possible.
In fact, anybody who can perform rack pulls with insane amounts of weight is always huge. It goes with the territory.
To achieve this goal with the rack pull, one needs to perform it properly.
How to Do Rack Pulls
• One’s standard deadlift form should be mastered first.
• Set the catch bars of a squat rack station to some point between the knees and mid-thigh, maybe even a little bit below the knees, depending on a person’s preference for range of motion.
• Load the barbell with more weight than what one normally does reps with for a standard deadlift.
This will require some experimentation because often, a person who is new to rack pulls won’t put on enough weight, or, the opposite will happen:
They will load the barbell with too much weight, overestimating how much they can lift.
• It won’t be long before a person figures out the appropriate load for a given height off the floor.
• Position the body in a way that makes you feel that you can lift safely and progress with heavier weights. Often this positioning is similar to a person’s usual deadlift.
• Range of motion at the top of the lift is supposed to be as complete as in a regular deadlift.
• Because most people want to move as much weight as possible with the rack pull, the load is usually too heavy for the touch-and-go style at the bottom of the movement.
In the touch-and-go style of the regular deadlift, the barbell plates very briefly tap the floor before the trainee pulls the weight back up.
When the load is enormous (relative to the person, of course) in the rack pull, the individual is forced to solidly set the barbell on the catch bars before lifting it back up again.
In fact, the load may be so heavy that the trainee must readjust their hands between each lift.
Sometimes there is a two-second rest in between repetitions. The idea behind the rack pull, as already pointed out, is to move as much of a load as possible.
In other words, there’s really no point in doing this with weight light enough to just bounce through the repetitions.
Form for the rack pull must be perfect to prevent injuries. Even if the bottom movement stops at mid-thigh, injury can still result if not careful.
One must not let the limited range of motion fool them into thinking that injury is not possible.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com
Two Mistakes with Walking that Prevent Weight Loss

If you’ve been walking up a storm yet have not lost weight, there’s a few reasons why.
Don’t give up yet. Learn how to make walking melt off the fat.
(more…)




Do Body Proportions Affect a Women’s Squat with a Barbell?
Why is it that some women find back squats easy while others struggle?
Some women take to this exercise fairly quickly and are just a natural at it.
Then there are those—perhaps you yourself—who just can’t seem to “get it…” even though you have solid knees, no back pain issues, etc.
This article pertains to the back squat—barbell across the back. If you’d like to do this, see first how you do with a bodyweight squat.
Many women will easily be able to drop to past parallel and feel comfortable, while others will struggle, feeling as though they will fall backwards even before they hit parallel (thighs parallel to floor).
This latter group will also find that their back has a tendency to round, while the “naturals” will be able to keep a small arch in their lower back (the correct form).
The key difference between these two groups is body proportions.
To prevent falling backwards your shoulder needs to be directly overhead the midfoot, forming a vertical line from shoulder to midfoot.
The Chair Test for Squat Body Proportions
• Sit on edge of chair that permits thighs to be parallel to floor.
• Keep feet flat on floor, wider than shoulder width, side by side.
• Move feet towards chair, keeping them flat on chair, as far as possible before you feel that you must elevate your heels.
• Keeping your back straight, arch in the lumbar area, lean forward so as to align shoulders smack overhead of the midfoot. No back rounding!
• How far must you lean forward to achieve the vertical alignment? This is how far you’d have to lean forward if doing a back squat with a barbell.
You may not have to lean that much forward (lucky) while others will have to pitch way forward (lousy proportions or “levers”).
Many women’s torsos are short, relative to femur (thigh bone), making them high waisted. What jumps out at me, in the image below of the woman on a treadmill, is how short her torso is, relative to hip-to-feet length and overall body height.

She’d probably have to lean way forward to get her shoulder above the midfoot in a back squat, though this can be somewhat offset by a relatively long shin bone.
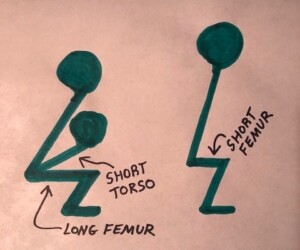
But generally, short torso + long femur bone (regardless of overall body height) = poor proportions for back squats.
If the torso is shorter than femur length, you can see why a big forward lean is required to get the shoulders over that midfoot.
If shoulder falls short of vertical line in an actual back squat, you’ll fall backwards. It’s Physics 101, no way around it.
But a torso longer than the femurs?
You won’t need to lean so far forward to align the shoulder over the midfoot, allowing you to sink straight down into a deep squat without folding in half.
These various body proportions are independent of overall body height. A very tall woman can have short femurs and a long torso.
A very short woman can be quite high waisted. I’ve seen tall women with crazy long SHINS, which helps offset a relatively short waist, allowing them to comfortably do squats with good form.
If you have bad squat proportions, you can still work around these by developing lower back flexibility, ankle flexability and adopting a wider stance with feet slightly pointing out.

If you’re struggling with squats, widen your stance to double shoulder width and see how it goes. Freepik.com
You can also do other forms of squats (kettlebells held at the shoulders or at the sides, plate held to your chest, etc.).
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.




Why You Shouldn’t Use the Squat Rack for Barbell Curls
Are you a schmuck who uses the squat rack for barbell curls?
This isn’t very considerate for those who wish to do squats and rack pulls.
Why do people tie up the squatting rack or cage with biceps curls? Usually they use an Olympic bar, but this doesn’t justify tying up the cage.
You can curl an Olympic bar anyplace in the gym; there’s always plenty of room, including before a mirror.
You can also use pre-weighted barbells; usually the amount I see being curled is within the range of those pre-fixed, shorter barbells.
Hogging the squat rack for biceps curls deprives someone from using this equipment for safety reasons.
Biceps curls allow you to be mobile in the gym, while the back squat does not. People need the cage for the stoppers in the event they can’t stand back up with the weight
That’s why it’s called a squat rack.
It’s designed for safety. Squat racks come in two basic styles.
One of them involves bars that you insert at different heights between the posts, making this design inviting for rack pulls.
Shutterstock/HD92
It’s not possible to do the rack pull (top deadlift) anyplace else in the gym unless you’re using relatively light weight; you need the stopper bars.
What benefit is there to doing biceps curls in the squat rack?
There’s none. None whatsoever. Now, it’s fair to point out that I’ve seen men doing this as a superset to a bent-over barbell row, using two Olympic bars.
But what about the lone soldier who’s doing ONLY biceps curls?
Well, maybe they want the squatting cage because the design enables them to set the bar back down at only hip level instead of onto the floor, saving them some energy expenditure.
But even when you consider this, it’s still not considerate.
I’m the type of person who will ask such a trainee if I can “work in” using the rack for squats.
But many people don’t have the nerve to do this. And for others, it’s not an issue of nerve; it’s an issue of distraction.
The squat rack is also often used for overhead presses, allowing the trainee to set the bar back down at shoulder level rather than to the floor. This is crucial for very heavy lifts.
Where else in the gym can one do this? Once again, it’s clear that the squat rack serves specific purposes—and one of those is NOT the biceps curl.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
How to Increase the Intensity of Inverted Rows

The inverted row is a fabulous compound exercise for which there’s many ways to increase intensity.
It seems as though the inverted row is the exercise that, when someone finally decides to include it in their program, nobody wants to be progressive with it. (more…)



Best Cardio Exercise for Love Handle Destruction
You can get rid of love handles with the right type of cardio exercise.
The wrong kind of cardio exercise, if you want to get rid of love handles, is the so-called long slow aerobics, a.k.a. steady state aerobics.
This is why you’ll often see people with love handles that never disappear, even though these folks spend a lot of time jogging, walking, pedaling, taking all sorts of classes like belly dancing, Zumba, low impact aerobics, step aerobics, etc.
The fat in love handles is fuel that’s not being used. Steady state cardio is not intense enough to force the body to significantly pull from these stubborn fat depots.
Get Rid of Ugly Love Handles

Another form of cardio will do the trick: HIIT: high intensity interval training. HIIT changes body chemistry and causes a metabolic ripple effect that results in substantially more fat burned.
This is because HIIT raises the body’s recovery needs so much, that the body starts pulling from the fat depots in the waist: the love handles.
Love handles will start shrinking with HIIT. High intensity interval training yields fantastic results in a fraction of the time that long steady state cardio would have to generate for the same results.
If you’re wondering, “Wow, this sounds too good to be true; there must be a catch!”
I’ll be honest: There is a catch. It’s hard work. Hard Work.
HIIT is not pretty. It gets you madly out of breath, like a cheetah panting like mad after failing to catch an impala.
Ever see what a cheetah looks like when the impala gets away? The animal is so winded it must stop completely and collect itself.
That’s pretty much the exertion level of genuine HIIT if you want to experience its fat burning effect to the max.
The good news is that each intensity interval lasts 30 seconds or less, and you need to do only seven or eight to create a huge bang for your buck. Kiss your unsightly love handles goodbye!
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: ©Lorra Garrick



How to Safely Descend Talus and Scree Slopes










































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}