

Can Acid Reflux Cause Left Sided Chest Pain?

Left sided chest pain is associated with a heart attack or cardiac trouble, so when people experience this, they hope to high heaven it’s only acid reflux.
So the million dollar question is: CAN left side chest pain be caused by acid reflux?
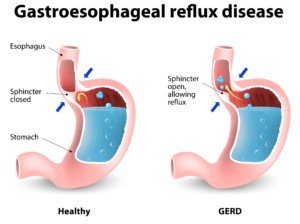
“While occasional acid reflux is normal, chronic acid reflux could be a symptom of a more serious condition known as gastroesophageal disease, or GERD,” explains Lauren Gerson, MD, board certified gastroenterologist formerly with California Pacific Medical Center in San Francisco.
She is a nationally recognized researcher in the field of general gastroenterology including management and treatment of GERD.
“GERD is a chronic disease in which stomach acid flows into the esophagus and irritates the lining,” adds Dr. Gerson.
Shutterstock/Designua
“This acid backup can sometimes cause non-cardiac chest pain, which likely occurs due to the spasm of the esophageal muscles that results from stomach acid refluxing into the swallowing pipe, causing the pain receptors in the area to be activated.”
Though the esophagus is located squarely behind the sternum (chest bone), this doesn’t mean that when it goes into spasm from acid reflux, that the pain must necessarily be felt smack in the center of the chest.
The contractions of the esophageal muscles in spasm could be such that most or even all of the pain is felt on the left side of the chest, or as a left-dominant type of pain.
Unfortunately, the way this actually feels cannot be distinguished from the way a heart related pain can feel – whether it’s from an imminent heart attack, one in progress, or angina (transient shortage of blood flow through the coronary vessels due to plaque buildup).
Having left sided chest pain but have not seen a doctor about acid reflux?
And what if also, you have not seen a cardiologist, and you’re a nervous wreck, struggling to get through each day, hands on chest, terrified the pain might be coming from your heart?
The first doctor you should see is a cardiologist. Get the most serious possibility checked out first.
What You Should Tell the Cardiologist
• Report that you’re having left side chest pain.
• Report any accompanying symptoms of these episodes such as shortness of breath or dizziness.
• Hopefully by the time you see the doctor you will have kept notes on any apparent triggers of this symptom, such as lying down, eating certain foods or anxiety.
• You’ll get a blood pressure check, EKG and stethoscope exam.
• You’ll have blood drawn for a cholesterol test and possibly for other markers that may indicate a potential heart problem.
• A cardiac stress test may be recommended, but if one isn’t, you can always ask for one as a screening procedure.
“In addition to non-cardiac chest pain, it is important for patients to be aware of typical symptoms of GERD including a burning sensation in the chest, regurgitation of food and difficulty swallowing,” says Dr. Gerson.
“If you are experiencing any of these symptoms, as well as non-cardiac chest pain, it is important to talk with your healthcare provider about your symptoms and what treatment options may work best for you.”
If your cardiologist clears you of any heart problem and assures you that your left side chest pain is not cardiac related, then your next step would be to pursue the cause of your anxiety-producing symptom.
• Are you experiencing the symptoms that Dr. Gerson describes?
• Does the left side chest pain occur only when in certain positions or only when lying down?
• Does it occur only in the middle of the night?
• Do certain exercises or movements with your arms bring it on?
• Does it hurt when you press on the area or lie on your chest?
You may not even have GERD or acid reflux; it could be a soft-tissue strain.
At any rate, you should get to the bottom of the cause of your left side chest pain so that your anxiety doesn’t return and cause you to revert back to worrying it’s coming from your heart – even if a cardiologist said that everything is working just fine.
Dr. Gerson passed away in July 2017 after a valiant battle against metastatic melanoma. Dr. Gerson devoted herself to solving her patients’ most difficult and longstanding health challenges.
passed away in July 2017 after a valiant battle against metastatic melanoma. Dr. Gerson devoted herself to solving her patients’ most difficult and longstanding health challenges.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Twinsterphoto

Can Excessive Sitting on the Job Thicken Your Waist ?

If you want to trim down that thick waist, you’ll need to spend less time sitting on the job.
Not only are desk jobs linked to bigger stomachs, but they’re linked to a bigger risk of heart disease. (more…)

How to Get 15,000 Steps a Day if You Have a Desk Job

You can get in 15,000 steps a day even if your boss won’t allow a treadmill desk.
There are ingenious ways you can make the step count rack up by the end of the evening. (more…)

Why Does Keflex Smell & Taste Like Smoke with Smoky Aftertaste?

Keflex stinks so bad that when I open the bottle to give my father a pill, I hold my breath. Keflex tastes like smoke & leaves a “burnt cigarettes” aftertaste, he says.
Keflex (cephalexin) is an antibiotic that comes in capsule form.
An article at abcnews.go.com points out that doctors may not have ever held the drugs that they prescribe, and hence, don’t know just how “stinky” they can be – and this would certainly apply to Keflex.
The article also points out that if a drug is “foul smelling,” this could be enough to make the patient stop taking it.
My father balks most times I give him the 500 mg Keflex, which is four times a day, prescribed due to a skin infection.
I first began suspecting that the Keflex capsules were more than just bad smelling when my father did not take the pill I set before him and instead continued napping.
If something stinks bad, it probably TASTES bad, even though it’s not chewed but swallowed whole.
Not only does Keflex taste like smoke, but it leaves an aftertaste that he describes as being like burnt cigarettes.
According to a pharmacist who was interviewed for the abcnews article, there are no studies on the effects of patient adherence to taking medications that stink or taste bad.
Thank goodness the prescription is for one week, though four times a day.
My father finally came upon a solution to neutralizing the stink odor and aftertaste of Keflex:
He takes it with his orange-flavored B12 pill.
The article cites patients complaining that their prescribed drugs smell and taste like sour milk, fish or even like skunk.
What does the FDA say?
Shelly Burgess, an FDA spokeswoman, told ABC News that the organization is aware of bad odor complaints.
She explains that the complaints “are not necessarily indicative of drug quality or safety concern,” and that the stinky quality “can occur as a result of the chemical composition of the drug product itself.”
So I guess we can assume that the reason Keflex smells and tastes bad – even if it’s described as smoky – that this is due to the chemical composition of the drug.
Remember, drugs aren’t supposed to smell good, but it would be nice if a safe coating could be applied to neutralize offensive odors and tastes.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ARENA Creative
Source: abcnews.go.com/Health/WellnessNews/doctors-learn-drugs-stinky/story?id=9844575

Elderly Falls: Tell Doctor & Risk Coumadin Prescription Stop?

What a real catch-22:
An elderly person on Coumadin takes a bad fall, but if you take them to the doctor this will result in a prescription cancellation for the blood thinner. (more…)

Can Unilateral Tinnitus of Acoustic Neuroma Seem Bilateral?

Should you exclude acoustic neuroma as the cause of your tinnitus if the “ringing” is in both ears?
Ninety-five percent of acoustic neuroma patients have the tumor in only one ear.
The remaining five percent have a tumor in both ears (bilateral).
The remaining five percent of patients with tumors in both ears have a genetic disorder called neurofibromatosis 2.
If you have NF2, you probably already know it, as most patients begin developing signs by their teens or early 20s.
So let’s talk about AN in a non-NF2 person; the tumor will be unilateral. Often, tinnitus is the first symptom.
When a patient reports unilateral tinnitus to a doctor, the doctor should take special note of this as being suspicious for an acoustic neuroma.
Though very rare (2,000-3,000 diagnoses yearly in the U.S.), an acoustic neuroma needs to be ruled out in cases of unilateral tinnitus.
The vast majority of unilateral tinnitus is NOT caused by an acoustic neuroma – which is benign and slow growing.
A person with tinnitus that seemingly comes from both ears may feel a sense of strong relief due to the following thought process:
“This can’t possibly be an acoustic neuroma because I hear the tinnitus in BOTH ears!
Whew! Here I am, fearing I have some kind of TUMOR that might need radiation treatment or whose surgical removal might cause permanent hearing loss – but thank God, these things affect only one ear.”
I was reading some posts on an AN site by patients; they were describing their initial symptoms related to these noncancerous masses.
What got my attention was a post by a woman who said that her tinnitus, before the surgical removal of her acoustic neuroma, had been in BOTH ears – and she did not have the NF2 genetic disorder.
You may think, How is that possible, both ears?
I posed this question to Brandon Isaacson, MD, F.A.C.S., Department of Otolaryngology – Head and Neck Surgery, UT Southwestern Medical Center, Dallas, TX.
Dr. Isaacson explains, “Tinnitus is most commonly perceived on the same side as the tumor but can occur in both ears.
“The hearing pathways crossing in the brainstem is the likely mechanism why it can be perceived in both ears.”
So there you have it. You are not automatically off the hook from an acoustic neuroma just because the tinnitus is bilateral.
Dr. Isaacson’s research interests include cochlear implants, endoscopic ear surgery and acoustic neuroma. His clinical interests include all aspects of otology and neurotology, with a special focus on skull base surgery.
research interests include cochlear implants, endoscopic ear surgery and acoustic neuroma. His clinical interests include all aspects of otology and neurotology, with a special focus on skull base surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Florida Chuck
Source: cancer.net/cancer-types/neurofibromatosis-type-2/cineurofibromatosis-type-2printer

Can Cymbalta Cure Irritable Bowel Syndrome ?

Cymbalta is sometimes prescribed off-label for patients who suffer from IBS.
And some patients swear that Cymbalta has cured them of their irritable bowel syndrome.
But what’s really going on here?
“Unfortunately, IBS is a chronic disorder for many patients,” begins Dr. Brian Lacy, MD, of Dartmouth Hitchcock Med Center, who specializes in functional disorders of the gastrointestinal tract and author of “Making Sense of IBS.”
Cymbalta Cannot Cure IBS Despite what Happy Patients Claim
“There is no medication currently available that can cure IBS,” says Dr. Lacy. “Cymbalta is approved by the FDA for the treatment of depression.
“Although no medical studies have evaluated Cymbalta (duloxetine) for the treatment of IBS, some health care providers use this medication off-label to improve symptoms of abdominal pain.
“Other medications are FDA approved for the treatment of IBS symptoms, and two in particular may help abdominal pain.”
Relief of symptoms, or symptom management, is not the same as a cure.
Dr. Lacy recommends for those suffering with constipation due to IBS a medication called LINZESS.
LINZESS may dramatically improve both constipation and abdominal pain,” he says.
Other patients suffer from diarrhea rather than constipation, and for those individuals, Dr. Lacy recommends Viberzi (eluxadoline).
“It may improve both symptoms. Both of these medications require a prescription, so please make sure that you discuss these with your health care provider to determine if one of these might improve your IBS symptoms.”
 Dr. Lacy combines his love of science, medicine and people to uncover the causes of symptoms like stomach pain, gas, bloating, diarrhea, constipation and regurgitation.
Dr. Lacy combines his love of science, medicine and people to uncover the causes of symptoms like stomach pain, gas, bloating, diarrhea, constipation and regurgitation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Twinsterphoto

Can a Digestive Problem Cause a Metal Taste in the Mouth ?

A metal taste in your mouth can be caused by a serious medical condition including cancer, but it can also be triggered by a disorder in your digestive tract.
“In the occasional patient, acid reflux (GERD) can cause the production of frothy secretions in the mouth; this is called waterbrash,” explains Dr. Brian Lacy, MD, of Dartmouth Hitchcock Med Center, who specializes in functional disorders of the gastrointestinal tract, and author of “Healing Heartburn.”
A metal taste in the mouth from a digestive issue?
Dr. Lacy says that this waterbrash “results from acid refluxing into the mouth and stimulating the salivary glands to make a bicarbonate-rich fluid.
“In some patients this may taste a little metallic. Otherwise, patients with IBS or chronic constipation are not more likely to report a metallic taste than others.”
So if you have irritable bowel syndrome or a benign chronic constipation, and you then begin experiencing this phantom taste sensation, you’d be wise to report it to your doctor.
What about cancer?
Cancer as a cause is actually not likely, but not impossible: More causes of a metal taste in your mouth.
Dr. Lacy combines his love of science, medicine and people to uncover the causes of symptoms like stomach pain, gas, bloating, diarrhea, constipation and regurgitation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can a Long IBS Flare Mean Something Serious; Should You Worry?

Panic often sets in when a person’s IBS flare seems to be going on and on without any let-up. (more…)

Double Hip Replacement Guidelines for Walking on a Treadmill



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}