
What Is Provent?

For some people with obstructive sleep apnea who can’t tolerate CPAP machines, Provent may be a godsend.
Just how does Provent work?
Provent is an FDA approved treatment for obstructive sleep apnea.
This nasal device has a valve design that attaches over the user’s nostrils.
It’s secured in place via a hypoallergenic adhesive.
As you breathe, the valve opens and closes. This redirects air through little holes, creating resistance when you exhale. This helps keep the airway open.
Each Provent device is single use and disposable, and must be prescribed by a doctor.
If a sleep study shows that the device lowers your apnea-hypopnea index to (on average) less than five per hour, then the device works.
However, people who faithfully use CPAP may also find that Provent is a convenient alternative treatment while they are camping or traveling somewhere where use of a CPAP would be cumbersome or not possible.
Symptoms of Untreated Sleep Apnea
• Excessive daytime drowsiness or sleepiness.
• The grogginess is not mitigated by napping; person fails to feel refreshed after a nap.
• Easily falling asleep while doing passive activities such as reading, working on a crossword puzzle, using a computer or watching TV.
• Dozing off in a vehicle while stopped at red lights.
• Waking with headaches in the morning that go away, without painkillers, within 30 minutes of being up and about.
• Difficulty concentrating or focusing on tasks; irritability.
• Someone telling you that while you sleep or nap, you stop breathing.
• Snoring or gasping in one’s sleep.
• Frequent trips to the bathroom overnight to urinate — not just the urge, but a good amount of urine coming out with each trip — despite abstaining from fluid intake in the hours before bedtime.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source:proventtherapy.com/provent-faq.php
Is There Really a Best Time to Drink Water ?

Other than when you’re thirsty or have signs of dehydration, does it really matter when you drink water? Or is the scheduling of water intake a bit too obsessive? (more…)

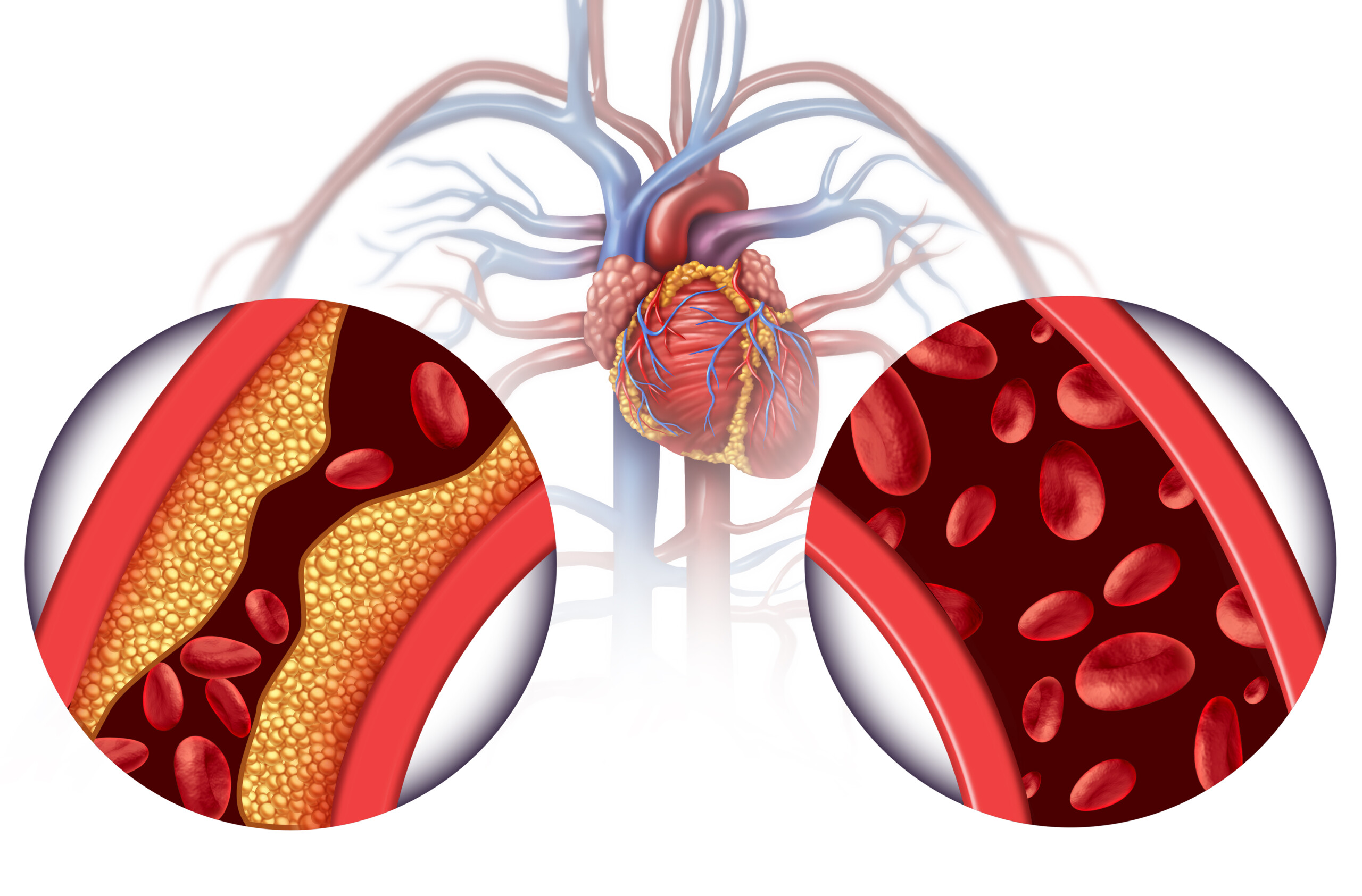
Natural Ways to Unclog Coronary Artery Soft Plaque
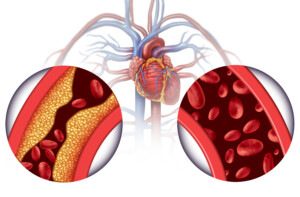
Soft plaque is unstable and can rupture, causing a heart attack; there are natural ways to unclog coronary arteries or kick back the soft plaque. (more…)
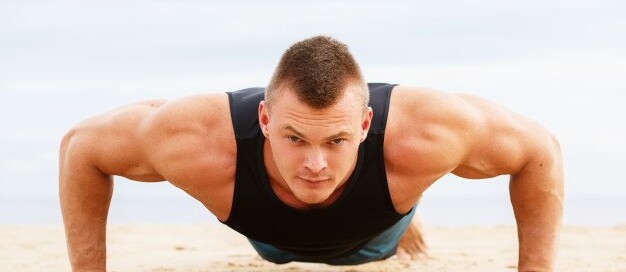
Do Pushups REALLY Work Your Abs?

You’re not imagining it: Pushups really do work your abs.
Think about what actually happens when you do pushups:
Your abdominal region is the link between stabilizing your upper body and your lower body as you perform this multi-joint exercise. (more…)

How Bad Is the Sitting Disease for the Brain?

Since the sitting disease is so bad for the heart and blood vessels, it’s no surprise that it’s also bad for the brain.
There is just no escaping the harmful effects of sitting on your can many hours day after day.
It has now been discovered that sitting too much is associated with shrinkage of the part of the brain that involves recent memory formation. (more…)

Can Staying up Late and Sleeping in Make You Die Sooner?

If you go to sleep late and wake up for the day late, this could put you at risk for an earlier death, when compared to going to bed earlier and getting up earlier. (more…)

If Cysts Look Benign on Mammogram Can You Stop Worrying?
Under certain circumstances, a cyst on a mammogram can have a benign appearance, but under other circumstances, it can look very concerning to a doctor. (more…)

Is Slow Growing Breast Cancer Worse Due to Longer Existence?

Some women believe that because the breast cancer tumor has “been in there” longer—despite slow growth—that this means it’s more dangerous than one that’s been present for only a short time but growing faster.

What Is a Subtle Benign Appearing Density on a Mammogram?

You may have come upon the descriptor of “subtle benign appearing density” in reference to mammogram imaging. (more…)

How Soon After Intercourse Can Pregnancy Symptoms Occur?

Symptoms or signs of a pregnancy can begin occurring very soon after having sexual intercourse.
But this doesn’t mean that in every case of conception, the symptoms of a pregnancy will always occur very soon after.
How does this all work?
After you have sexual relations, there is a period of time during which conception can occur: from a few hours to five days.
Yes, that’s right: Up to five days after having sex, you can still get pregnant.
Sperm Hangs Around for Awhile
Sperm can live inside the uterus and fallopian tubes for up to five days, during which an egg (ovum) may be released from an ovary – and permeated by a single sperm to create an embryo.
Ever wonder why two sperm can’t penetrate an egg, even though there may be tons of sperm trying to permeate the egg at seemingly the moment that the “first one” achieves this?
Once a sperm penetrates an egg, a chemical reaction occurs that makes the egg impenetrable to the other sperm.
Symptoms of Pregnancy Occurring Soon After Having Sex
“Missed menstrual cycle would be the earliest pregnancy symptom,” says Mylaine Riobe, MD, founder of Riobe Institute of Integrative Medicine.
Dr. Riobe, who’s board certified in ob/gyn and integrative medicine, is the author of “The Answer to Cancer” and has over 15 years’ experience using integrative techniques to treat diverse patients.
This sign will be particularly blaring if your periods have always been very regular and predictable — and you’re vigilant about keeping track.
“Some women begin to feel breast tenderness, mild nausea as soon as a couple weeks thereafter,” says Dr. Riobe. “Symptoms tend to correlate with HCG (human chorionic gonadotropin) levels.”
If your home pregnancy test is positive, have a doctor confirm this, as these tests are not 100 percent accurate — despite what advertisements might have you believe.
This includes for a negative result as well. If you have a gut feeling that you’re pregnant, get a confirmation from a physician, even if two home pregnancy tests in a row have shown a negative — or positive — result.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}