

Addison’s Disease: Do You Have Unexplained Serious Symptoms?

Addison’s disease can be fatal and also go misdiagnosed for many months. The symptoms are quite varied and can mimic other conditions.
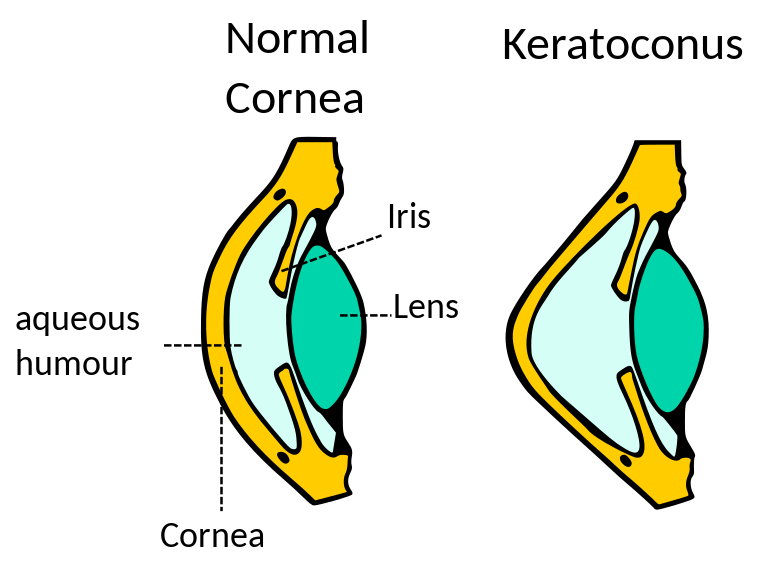
One Woman’s Life with Keratoconus: a Cornea Disease
![]()
The most striking thing about keratoconus and the apparently other congenital eye diseases that greeted me upon, or relatively shortly thereafter, my birth (i.e., amblyopia, alternating vision), is that I’ve never known what it is like to have “normal vision.”
Shortly after I was born, I underwent surgery to correct my “crossed eyes.”
My first memory of what passed for vision screening nearly seven decades ago was of having each eye covered while I tilted my hand in the direction of the letter “E” as I read it, first with one eye covered, then the other, on a screen.
Right-side up, upside down, flipped left, then right — that was my introduction to the fifth letter of the alphabet, thanks to the ophthalmologist who felt it necessary to examine me at a time when most everyone else I knew could get by with an optometrist’s appointment (though, at that age I was probably only familiar with the generic term “eye doctor”).
I was fitted with my first pair of glasses at age three. As a toddler I developed amblyopia, leaving me with vivid memories of the pirate patch I wore in order to correct my “lazy eye.”
There must have been some other kids who wore glasses, but I don’t remember any.
All I remember was being teased and being treated like an outcast at a time I wanted to fit in.
Growing up in Minnesota within walking distance of two elementary schools, as I walked to and from Fern Hill (and later Park Hill) school, during a Gopher state winter, I always looked forward to spring when my glasses would no longer fog up.
I also had to endure the memorable indignity of a bully breaking my glasses.
As my vision worsened, my annual eye care appointments became semiannual, but hope was on the horizon when I became a teenager. It was then that I first became aware of the term kerataconus.
Keratoconus is a thinning of the cornea. Vision is sometimes blurry, and nighttime driving distorts the way headlights and taillights appear.
Keratoconus develops slowly but, in my case, definitively during my early teens to the point where, following associated eye surgery, little-by-little I was able to reduce the time I wore glasses and wear the then-fashionably trendy hard contact lenses for increasing periods of time!
Though there was (and over a half-century later remains) no cure for keratoconus, contact lenses not only have a stabilizing effect, they improve the quality of vision of glasses alone.
Though keratoconus prevented me from wearing soft contact lenses, as the technology improved, I was able to graduate to gas permeable contact lenses.
But, as my keratoconus eventually progressed, even gas permeable lenses failed me, as the shape of my corneas — never fully round like most people’s — became so pointed that contact lenses would no longer fit on my eyes.
This was not good news for me, not only emotionally, but financially. Inflation had caught up with the prescription lenses I required by that point with a new pair of eyeglasses costing me about $300.
Even at those prices, my insurance wouldn’t cover the more costly, thinner lenses and more attractive frames, so I found myself weighed down by “Coke bottle” glasses that gave me headaches!
Relief came when my vision difficulties progressed to the point where I needed cornea transplantation.
Because of the risk inherent in any (vision-related) surgery, eye surgeons will only operate on one eye at a time.
By the time I was ready for my other eye to receive a cornea transplant, the FDA approved (and my insurance covered) the less expensive (but more effective) intraocular lens.
By this time I had reached an age where I needed reading glasses. I tried them but didn’t like them, so to this day I use a magnifying glass, if need be, or simply increase the font size when I’m using my computer.
A side effect of the prescription eye drops used prior to, and following, some eye surgeries, including mine, was the premature development of cataracts.
The silver lining was that at a time when I would normally have developed the cataracts of aging eyes, I’d already had the surgeries a couple of decades before.
And while my vanity still keeps me from investing in glasses, I now not only appear to the uninitiated to have “perfect vision,” my eyes have formed a natural bifocal so that should I decide to cast my pride aside and buy a pair of eyeglasses, I won’t need bifocals.
While I might hope that keratoconus would lessen the odds of my developing macular degeneration and/or glaucoma, the fact is keratoconus has no impact on the odds of developing the diseases of aging.
At least keratoconus doesn’t increase those odds, though it still prevents me from being a candidate for LASIK surgery.
Given how far I’ve come, I think I can live with that.
The publisher/executive editor of Stacy’s Music Row Report, Stacy Harris is an internationally known author, digital content creator, pop culture expert and community activist. Stacy has covered the Nashville entertainment scene as a Nashville-based stringer for Newsweek and as a domestic stringer for the ABC Radio Network and its affiliates. More on keratoconus.
Top image: Madhero88, CC BY-SA 3.0/creativecommons.org/licenses/by-sa/3.0>, Wikimedia Commons

A Caregiver’s Four Lessons on Rare Disease

According to the National Institutes for Health, 25-30 million people in the U.S. are affected by an estimated 7,000 rare diseases. Many of those diseases are serious or life-threatening.
That’s nearly the same number of people with heart disease. And I would hope that each one of those people with a rare disease has a caregiver helping them navigate the often exhausting, lonely and frustrating experience of finding the right care.
Those patients plus caregivers add up to 15% or more of the U.S. population.
Although they are separated by their differing diagnoses, individuals with rare diseases often struggle through a similar set of problems related to health care, family life, employment, mental health and other aspects of living with a serious and often chronic condition.
I saw this firsthand. For several years starting in 2000, I was the caregiver for two family members with the rare disease of hereditary coproporphyria.
Here are four things to expect as an individual with a rare disease or as their caregiver.
Walking a Long Road to Diagnosis
Rare diseases are almost by definition hard to diagnose. It’s not uncommon for patients to struggle for 2-15 years to get a diagnosis.
For me and my then-new wife Connye, it was nearly six months between the onset of illness and an accurate diagnosis.
But she had suffered serious and unexplained symptoms for years before I met and married her.
For her teenaged son Brad, it was more than a year, including many months after his mom was accurately diagnosed with a condition that he could inherit.
Porphyria is tough because it can look like so many other conditions.
It’s an enzyme deficiency that can attack any part of the voluntary or involuntary nervous system. Because of this, some researchers have nicknamed the disease “The Little Imitator.”
So, when you and your loved-one are looking for a diagnosis, be patient, be persistent and trust yourselves.
During the diagnostic process, both Connye and Brad were told that it’s “all in their head.” This isn’t an uncommon experience for people with rare diseases.
One emergency department doctor said this to me about Brad even after I explained his mother’s hereditary condition and the fact that she was currently a patient in the same hospital.
If a diagnosis doesn’t feel right or complete, it probably isn’t. Healthcare workers may be the medical experts, but you are the expert of your situation.
Encountering Dead Ends
Along the road to an accurate diagnosis, you’ll likely receive advice, diagnoses, procedures and treatments that are dead ends.
For Connye, this included guesses about infectious disease, multiple sclerosis, depression, heart disease, pancreatic cancer and other conditions which led to treatments and procedures such as:
- Steroids
- Colonoscopy
- CT scan
- Transesophageal echocardiogram
- Radioactive gallium scan
- Psychiatric hospitalization
- Electro-convulsive therapy
Some dead ends can’t be helped. Many healthcare providers will be trying to do their best in the face of what can be scant and baffling evidence.
Again, trust yourself. Avoid non-reversible treatments such as a major surgery if you don’t trust the reasoning.
And on the flipside, if your path to getting a test that you believe would help is blocked, find a way around.
Luckily for us, the test for porphyria is easy and inexpensive: chemical analysis of a 24-hour urine collection.
But twice, we needed to go outside our insurance network to get the care we needed.
- First, to find an available neurologist, which led finally to an accurate diagnosis.
- Then, after the diagnosis, we again went outside of our network to start getting the treatment that Connye needed. Our approach was to get the treatment now and argue with the insurance company later.
Becoming a Rare Disease Expert
Seeking an accurate diagnosis of a rare disease is an involuntary education.
By the time you have a correct diagnosis, you’ve likely become an expert in your condition.
You will have spent more time researching your specific illness than nearly all medical personnel whom you encounter.
We saw this when we went outside of our insurance network to get treatment at an out-of-state medical school.
Even while under the care of the school’s porphyria researcher, we found that most of the nurses and medical students knew less than we did about porphyria.
You’ll need to help train your healthcare providers in how to care for someone with your condition.
For example, with porphyria there are classes of drugs that can trigger or worsen symptoms. Giving our healthcare providers that information to place in Connye and Brad’s medical records helped them to help us.
You are a primary way, and maybe even the only way, that providers will learn about these things.
Finding Your Rare Disease Community
Along the way, you’ll build up a network of other people who are on the same journey. This was true even 20 years ago, before the advent of social media platforms and smartphones.
Be a good traveling companion to others. Share what you’ve learned and the sources where you learned it. It’s okay to vent and commiserate at times, but generally a good attitude will win you more friends, information and insights.
Connye eventually connected with other patients and a great hometown specialist for porphyria through a group on Yahoo.com. (Yahoo shut down their groups feature at the end of 2020.)
Ironically, she’d been seen by another doctor in the same practice as that specialist, but no mention or connection was ever offered.
Many rare diseases have a genetic component. That means you might find insight, community and answers within your extended family.
Or — you might be the trailblazer who unravels a medical mystery that’s followed your family for generations. That was our experience.
Reaching a New Normal
Once you find an accurate diagnosis, you’ll feel like you’ve reached a new normal.
Diagnosis will give you clarity and a course of action. You’ll have a new body of knowledge and a new group of connections that you couldn’t have pictured at the start.
Life won’t be the same, even if your rare condition can be permanently cured.
The journey changes you, but you will get there.
Matthew Spaur is a marketing consultant, author and voice actor. His memoir “Making a Small Fortune” details his family’s struggle with porphyria while he ran a weekly newspaper. More on porphyria.
Top image: Freepik.com/katemangostar

Is Exercising Three Times a Day Overtraining or Obsessive?

How can you tell when exercising three times a day is harmful? Working out three times daily doesn’t necessarily mean an obsession or unhealthy fixation.

10 Gym Mistakes by Plus Size Women Wanting to Lose Weight

Here are 10 common workout mistakes that overweight women wanting to lose weight often make.

A Woman Diagnosed Autistic in Middle Age: My 10 Superpowers
Yes, autism DOES come with superpowers. I can’t split the Red Sea, but I have exceptional abilities that are clearly the result of an autistic brain.

10 Immune Boosting Tips and Tricks for Postmenopausal Women

Postmenopausal women need to incorporate these 10 immune boosting practices if they want to live their healthiest, longest life.

“Pimple” on Teen Girl’s Chin Diagnosed As Rare Cancer Called Rhabdomyosarcoma

One day you are a regular mom and the next day you are a cancer mom. It happens in an instant.
It doesn’t matter if bottle fed or breast fed or if your child ate McDonalds or broccoli, played sports or read books, if you are black, brown or have white skin, if you are an infant or a teenager.
Cancer knows no boundaries, knows no race. It seems to come from nowhere and then one day you find yourself thrown into this world of cancer where terms like chemotherapies, MRIs, radiation, PET scans, nausea medicines and mouth sores become your everyday vocabulary.
My oldest daughter, Katie [above], was 15 when she was diagnosed. She was a star athlete, ate all her fruits and vegetables, did all the right things, and it didn’t matter.
What started as a little pimple on her chin turned into a malignant tumor, a rare form of rhabdomyosarcoma, within a matter of months.
I recall feeling like this must be the start of her “acne” days since she was a hormonal teenager.
We went through all the expensive forms of skin care to no avail. We ended up seeing two dermatologists, one urgent care visit, two emergency room visits before we finally got some answers as to what this mass was growing on Katie’s chin.
No one was thinking cancer during those months and when we finally got the proper diagnosis, it was like the wind was knocked out of all our sails.
Instead of Katie’s sophomore year in high school being filled with football games, homecomings and prom dates….it was filled with various forms of chemotherapies, 28 days of radiation, a bald head, not to mention hundreds of hospital visits.

Karen and Katie
She was robbed of her normal teenage experience the day of diagnosis and our family was robbed of the normalcy of a carefree family life.
Katie is now (as of 2022) thankfully thriving as a senior at Valdosta State University.
She still gets scans and checkups every six months. The protocol that she endured for a year had not changed much since the chemotherapies she had to take were invented back in the early 1960’s.
Thankfully, this 50+ year regime did the trick for Katie. She was lucky.
But the fears of relapse will never be far from this mother’s mind. Knowing that there are no “new tricks” if she does relapse makes me catch my breath.
The fact that Katie’s drug protocol and most other childhood cancer treatments have had no significant changes or improvements in decades was one of the most upsetting pieces of knowledge I learned when my family was thrown into the world of pediatric cancer.
When I think of all the other progress that has been made in literally all other industries of life in 50 years, and no real significant changes to pediatric cancer treatments, honestly makes my blood boil.
The only reason for this is that pediatric cancer treatments is still considered too rare and therefore not a “money maker.”
Less than 4% of federal funding goes towards pediatric cancer treatments. I know we all feel our children deserve so much better.
The thing is, it is the treatments themselves that normally lead to a child’s death.
These treatments are so toxic that even though they kill the cancer, they leave behind such destruction to the child’s body and there are just so many devastating side effects. This needs to change.
During Katie’s battle, she was treated by the amazing staff of Children’s Healthcare of Atlanta.
While there, we learned of an amazing organization called CURE Childhood Cancer. This group would bring us meals while Katie had her inpatient visits, provided counseling services, as well as included us in various activities throughout the year that provided much needed smiles.
Even though our world had been thrown upside down, there was such comfort to be surrounded by people who truly understood what our family was going through.
Once Katie finished treatment, I knew I needed to be part of moving the mission forward of spreading awareness about lack of funding for childhood cancers. I joined the staff of CURE Childhood Cancer a few months after Katie’s completion.
CURE’s mission is to conquer childhood cancer through funding targeted research as well as support families currently in the battle.
CURE invests over $4 million annually to very promising research. At the same time CURE is walking alongside families who are facing a cancer diagnosis by providing financial assistance, meals, counseling and so much more.
I truly believe we will be able find a CURE in my lifetime and so thankful to work for an organization whose sole mission is to do so.
September is Childhood Cancer Awareness Month. This is a time to shine the light on the realities of childhood cancer, emphasize the importance of life-saving research, and join to make a difference for children diagnosed.
To learn more how you can help, please visit https://curechildhoodcancer.org.






































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}