
Top of Head Pain from Fibromyalgia: Cause

Pain at the top of your head can be caused by fibromyalgia, and a top fibromyalgia doctor explains why and what to do about it.
“Fibromyalgia can cause a host of different pains, most often from muscle pain and sometimes from nerve pain,” including that at the top of the head, says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
What does the pain at the top of the head feel like to fibromyalgia patients?
“The nerve pain is characterized by sharp electric shooting type pains,” says Dr. Teitelbaum.
“Most of the other pains are associated with what are called ‘trigger points’ which are the ‘bunched up bellies’ of tight muscles or tender points where the tight muscles attach to the bones,” he continues.
The discomfort at the top of the head, which can also be described as the crown of the skull, is actually referred from an origin point that’s located at the base of your skull at the back of the neck.
In other words, the location of discomfort is distal from the origin of the problem.
The origin, at the base of the skull, back of the neck in those with fibromyalgia, consists of tight muscles — the tightness being “where they attach at the base of the skull in the back of the neck,” says Dr. Teitelbaum.
“This refers pain to the crown of the skull and behind the eyes.”
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

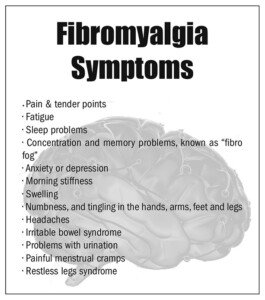
Pinprick Sensations & Fibromyalgia: Cause, Natural Solutions

Fibromyalgia can sometimes cause a pinprick sensation in your skin. Why is this?
“Fibromyalgia can cause a whole range of nerve sensations including pins and needles (mostly in the hands and feet – called paresthesias),” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally.
His latest book is “The Fatigue and Fibromyalgia Solution” (Avery Penguin 2013).
“In the absence of other nerve problems such as severe localized weakness or numbness, these may be reasonably ignored,” adds Dr. Teitelbaum.
“Other nerve pains are also common in fibromyalgia and can be readily treated with natural treatments.”
A sensation of pinpricks can be difficult to ignore, even though you now know that they don’t mean anything serious as long as there isn’t any numbness or focal weakness.

Dr. Teitelbaum suggests a natural remedy for pinprick feelings that consists of a mineral, vitamins, an antioxidant and an amino acid, as follows:
• Magnesium: 200 mg a day
• Vitamins B6 (25 mg daily) and B12 (500 mcg daily)
• Lipoic acid (300 mg twice daily)
• Acetyl l-carnitine (1500 mg every day)
Can medications be useful in reducing pinprick sensations from fibromyalgia?
Yes, says Dr. Teitelbaum.
Ultram, Neurontin and Cymbalta are several examples of medications that can reduce or numb nerve pain. NSAIDs like aspirin are usually not effective.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why Does Gastric Bypass Surgery Cause Belly Pain?
Pain in the belly following gastric bypass surgery can have a number of causes, and it’s not even that uncommon.
Also keep in mind that a major cause of this is the fact that you were just cut open in the stomach.
Belly Pain after Gastric Bypass Surgery: Here Are Some Causes
“Again, this can be benign from something as simple as indigestion or a tight abdominal wall muscle,” says pain specialist Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
“But if it is a new pain, especially if it is severe and the surgery was recent, call your physician,” continues Dr. Teitelbaum.
“Any severe abdominal pain, especially if associated with vomiting without diarrhea, or with severe tenderness when pushing on the abdomen, should be checked.
“If the surgery was recent, concerns include a rupture or infection, or obstruction from an adhesion.”
These last few possible causes are life threatening. Waste no time getting to the emergency room.
What seems like even a minor delay can be the difference between life and death.
Another possible cause of pain in the belly region after gastric bypass surgery is that of kidney stones, since the procedure alters the way the body absorbs oxalate and calcium.
This problem, though, would not occur right away; it’s a possible long-term complication.
Interesting statistics regarding bariatric surgery:
A surgeon earns between $4,000 and $6,000 per operation.
A Fresno, California team of three physicians performed 1,128 gastric bypass operations in a single year.
The fatality rate is half a percent.
So in summary, though pain in the belly is not all that uncommon after a gastric bypass operation, it can also be a sign of something that needs immediate medical attention.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Lina Wolf, magenverkleinerung.tips
Source: gastric-bypass-surgery-lawsuits.com/pgs/gastric_bypass_statistics.html

Can’t Sleep and Have Pain All Over? Solutions

If you’re suffering from pain all over your body but also from insomnia, find out what you may have.
If your entire body is suffering from pains or aches, and you have trouble with sleeping, these issues often go together.
Of course, body-wide pain can easily cause insomnia.
Here is information about when these two symptoms are independent from each other, that is, caused by a third agent.
And what is that third agent?
“Chronic widespread pain is becoming increasingly common,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “From Fatigued to Fantastic!”
“Unfortunately, most physicians are still clueless about how to evaluate this symptom. The first and key question to ask is, ‘Can you get a good night sleep?’
“If the answer is no and you have horrible insomnia associated with the widespread pain, it is likely coming from fibromyalgia or a fibromyalgia related process. If so, fatigue and ‘brain fog’ are also commonly present.
“This is true even if there is another problem such as lupus triggering the fibromyalgia.
Unfortunately, some physicians who have not stayed up-to-date with the science have a simple motto: IF I.”
What Dr. Teitelbaum is referring to is that of a doctor thinking, “If I don’t know what’s wrong with you, you’re crazy!”
Dr. Teitelbaum continues, “Then, instead of doing a proper evaluation, they may simply tell the patient that they are depressed.”
Though depression can cause body-wide pain, this article is about people who do not have any depression or diminished mood issues.
“If a good doctor does not know what is wrong with a patient, they will simply say so.”
Pain All Over Body, Insomnia, Fibromyalgia
Dr. Teitelbaum further explains, “My randomized double-blind placebo-controlled published research has shown that by treating with the SHINE Protocol (Sleep, Hormones, Infections, Nutrition, and Exercise), 91% of fibromyalgia patients improve with an average 90% increase in quality of life and more than 50% decrease in pain.
“The study and information on this can be found at www.endfatigue.com, and the free Symptom Analysis program on the homepage can be dramatically effective at helping you determine the cause of your fibromyalgia and how to effectively treat it.”
If you’ve been having trouble sleeping, along with pain all over your body, consider that this might be fibromyalgia.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes
Are Pushups Painful Due to a Strange Lump in Wrist?

Does pain in your wrist make pushups difficult and you’ve now noticed a little rubbery lump in your wrist?
The lump may be tender if you press on it.
It’s not rock hard; it gives a little when you press on it, but it’s not super soft, either.
What is this strange painful lump in your wrist that messes up your pushups?
“The most common cause of a lump in the wrist is a small fluid filled cyst called a ganglion cyst,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
“The good news is that it is quite benign and reasonable to ignore unless it is annoying you enough to need treatment.”
In other words, it’s not cancer and cannot turn into cancer. It also will not cause local destruction.
This odd but harmless mass stays the same size if one decides not to have it removed.

Ganglion cyst. Shutterstock/girl-think-position
Treatment for a lump in your wrist is something you should consider if it’s interfering with pushups.
I have a ganglion cyst and I must do pushups while grasping dumbbells or pushup handles on the floor.
This is no big deal and actually allows for greater range of motion.
However, a ganglion cyst can also cause pain when doing bench dips due to the positioning of the hands.
At one point in my life, it was causing pain while doing lying chest presses with heavy dumbbells as well as when pushing against handles for the seated chest press.
But that inconvenience was short-lived and eventually went away spontaneously.
Dr. Teitelbaum says that “treatment includes putting a needle in to drain the cyst or surgically removing it. Recurrence is not uncommon with either of these options.
“The best option? Ignore it (as long as it does not cause pain). It may go away spontaneously.
“If you need to do something, I would begin with having the doctor simply put a needle in to see if it can be drained (depending on how thick the fluid inside the cyst is). I would save surgery as a last resort.”
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
When to See Doctor for Sharp Pain when Breathing
If you’re experiencing sharp pain when breathing, this may mean something quite serious that needs fast medical attention.
This can also mean something that’s nothing to worry much about.
Breathing that’s accompanied by a sharp kind of pain can be benign…or…it can be dangerous, says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
“Because of this, if it is a new symptom you should check with your physician – especially if it is associated with shortness of breath, cold sweats or fever.”
When is sharp pain when breathing a serious issue?
“The worrisome causes include irritation of the lining of the lung (called the pleura) or the heart (called the pericardium),” says Dr. Teitelbaum. Pneumonia can cause this.
“In most cases, however, it simply turns out to be benign pain coming from tight chest wall muscles – most commonly along either side of the central chest bone (called the sternum) or on the chest wall two inches below the right or left nipple where the muscles attach.”
This problem is often referred to as costochondritis “because of the likely mistaken assumption that the pain comes from tender cartilage around the ribs and sternum,” says Dr. Teitelbaum.
The discomfort “usually originates in muscles that are tight, in areas called trigger points or the muscle insertions where they attach to the bones.
“A simple telltale? If pushing over the painful area (give a good hard push with your thumb) reproduces or relieves the pain, it is most likely to be muscle related” — perhaps caused by overdoing an exercise regimen in the gym or on the job lifting heavy items.
“If it does not, it is likely coming from something beneath the ribs – like the heart or lungs,” adds Dr. Teitelbaum.
Sharp pain while breathing that’s coming from the heart or lungs always warrants medical attention. Always. This is nothing to brush off — never.
“If you have ever eaten ribs at a restaurant you can see that they are pretty thick.
“Pushing on them is not likely to affect the organs underneath the ribs – but will affect the pain in the muscles overlaying the ribs.
“But see your physician anyway for this symptom, to be on the safe side.”
A rib fracture can also produce this scary symptom, though with a rib fracture, there will be visible bruising in the area of the fracture. There will also be tenderness in the area.
If you’ve been experiencing a sharp kind of pain when you take breaths, it would be a very smart idea to have a doctor check you out — even if you’re “young and healthy.”
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She is also a former ACE certified personal trainer.
.
Top image: ©Lorra Garrick

Ankle Swelling in the Elderly: Causes & Solutions

Though the site of swollen ankles in elderly people is quite common, this commonality does not rule out a potential life-threatening cause of this symptom.
Ankle swelling in an older person can mean a very serious medical condition.
“If the swelling is new and only in one ankle, especially if the calf or back of the thigh is tender, see your physician to rule out a blood clot,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
Another Serious Cause of Ankle Swelling in the Elderly
If both ankles are swollen, this could mean heart failure.
Dr. Teitelbaum explains, “This is usually associated with shortness of breath, which gets worse after you have been lying down for a while, as well as shortness of breath with exertion.”
An elderly person may assume that shortness of breath is a normal part of aging and not see it as a sign of something more serious.
“Heart failure is a common cause of unnecessary deaths,” continues Dr. Teitelbaum. “Why do I say unnecessary?” he adds.
“Because simple natural therapies are dramatically effective at improving heart failure.
“Your physician, sadly, will likely not have seen this research because these treatments are generally low cost and therefore not profitable for the drug companies to advertise.”

Shutterstock/AppleDK
Dr. Teitelbaum’s Recommendation for a Healthier Heart
“I find that a recipe of ribose (10 g a day), coenzyme Q 10 (200 mg a day), magnesium orotate (3,000 mg a day), acetyl-L-carnitine (1500 mg a day), plus a good B complex vitamin with 200 mg of magnesium (The Energy Revitalization System vitamin powder) will dramatically improve heart failure and other cardiac symptoms within six weeks – and has also been shown to prolong life.”
Innocuous Cause of Ankle Swelling in Elderly Men and Women
“If it is mild swelling that occurs at the end of a long day and was gone by the time you wake up in the morning and occurs in both legs, this is most often simply the effect of gravity,” says Dr. Teitelbaum.
“It helps to prop your feet up on a pillow while you’re resting at the end of the day,” explains Dr. Teitelbaum “so the fluid drains out of your legs before you go to bed.
“Otherwise it will do so while you are sleeping, and you’ll have to wake up to go pee. Varicose veins or venous insufficiency can also cause this.”
Kidney disease, liver cirrhosis and tight socks can also cause ankle swelling (and this is not limited to the elderly).
Additional causes of edema swelling in the ankles of an elderly person: kidney or liver disease, low thyroid, celiac disease and excessive salt/sodium intake.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Toa55

Is Twitching in the Bottom of Your Foot Scaring You?

If the twitching in the bottom of your foot is driving you mad, this article is a must-read.
Twitching in the bottom of the foot may at first seem innocent enough, and at the most, just a nuisance.
It may be most prominent while you are seated in a relaxed position, or reclined in a comfortable chair.
The problem with twitching in the bottom of your foot occurs when you decide to search the Internet about this, and are led astray by ALS sites or even multiple sclerosis sites.
Though you learn that muscle twitching (called fasciculations) can have quite a few benign causes, for some reason you zero in on what’s actually the least likely cause: ALS.
You zero in on this because it’s also the deadliest cause. This is how the mind can work.
YOU ARE NOT ALONE.
I was once reading a forum thread regarding the issue of fasciculations.
This phenomenon is often referred to as benign fasciculation syndrome when it becomes frequent and annoying enough.
People with benign fasciculation syndrome may spend too much time perusing the ALS sites and even reading the forums on these sites, going as far as registering and getting involved to collect more information.
Every time they have a fasciculation, the fear ALS. In that forum I had once read, somebody summed it up beautifully: “This thing really messes with your head.”
So what can be causing the twitching in the bottom of your foot?

Shutterstock/Pamela Au
“There are many causes for muscle twitching, most of which are benign,” explains neurologist Dr. Mary Dombovy, a neurologist with Rochester Regional Health in New York.
Dr. Dombovy continues, “Most people will have at least some episodes of muscle twitching during their life and if it is isolated to one area and not associated with other symptoms and goes away in a few hours or days, you don’t need to see a doctor.
“Some common causes of muscle twitching include exercise, particularly prolonged exertion, electrolyte abnormalities, muscle or nerve injury, muscle or nerve disease (most of which is not ALS).”
Massage the bottom of your foot if it continues to twitch, and curl the toes in and release them, alternating this way, to give the foot some exercise.
Drink plenty of water, as dehydration can also be causing the fasciculations.

Freepik.com
Anxiety can aggravate this symptom. Try to relax, meditate, strike some yoga poses, relax in a hot tub, listen to some soothing music – anything to calm your nerves and restore some positive thinking.
Like that one forum participant said, an obsession with fasciculations can really mess with your head.

Dr. Dombovy completed her neurology residency at Mayo Graduate School of Medicine. She is board certified in both neurology and physical medicine and rehabilitation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/cunaplus

Why Does Anxiety Cause Muscle Twitching?
Anxiety can cause muscles to twitch, and this includes stressing over this very situation.
It’s common for a person, who’s been experiencing twitching muscles, to notice an increase in frequency and/or a “spreading” of the fasciculations in relation to increased anxiety over this.
How is it that anxiety, even if it’s about finances or workplace security, can cause muscles to twitch?
“Persons with anxiety or panic attacks have higher levels of excitatory neurochemicals such as epinephrine and norepinephrine,” explains neurologist Dr. Mary Dombovy, a neurologist with Rochester Regional Health in New York.
“In essence they are having a ‘misdirected’ fight or flight response. These neurochemicals cause the feeling of anxiety, increased heart rate, increased blood pressure and tremors or twitching.
“When one is in this state, they are also hyperalert, and external stimuli such as a sudden noise may cause a startle response.”
The Fight or Flee Response
This is the body’s way of preparing for … a fight or flight … to a perceived danger.
We inherited this reaction from our primitive ancestors, who needed this response to survive in the harsh wilderness with wild animals.
In a modern world, we continue to perceive threats that trigger this survival response.
Except the threats aren’t dangerous and thus don’t require a fight or flight, such as being stuck in a traffic jam, trapped in a stressful business meeting or stressing about mounting debt.

Freepik.com
The body doesn’t distinguish between facing a wild animal and balancing the checkbook.
Stress causes the increased heart rate and blood pressure, and the muscle twitching.
The fasciculations are the body’s way of revving up for the fight or flight.
Anxiety over this will almost always intensify the twitching. Stress management is key to subduing this annoying reaction to a perceived threat.
The best way to battle stress is with regular rigorous exercise.
Intense exercise causes increased production of hormones that counteract another hormone that we’ve all heard of: cortisol, the “stress hormone.”
Exercise also promotes changes in the brain that lead to a mellowing effect and clearer thinking.

Freepik.com, javi_indy
Dr. Dombovy completed her neurology residency at Mayo Graduate School of Medicine. She is board certified in both neurology and physical medicine and rehabilitation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Twitching Arch of Foot: Causes, and Should You Worry?
If the arch of your foot has been twitching lately, you need to read this information.
Twitching in the arch of the foot can be very annoying and distracting, but this doesn’t mean it more likely is a serious problem than is not a serious problem.
Have you been reading too many ALS sites and are now scared you might have this deadly disease, since muscle twitching (fasciculations) can be a symptom?
“There are many causes for muscle twitching, most of which are benign,” states neurologist Dr. Mary Dombovy, a neurologist with Rochester Regional Health in New York.
“Most people will have at least some episodes of muscle twitching during their life, and if it is isolated to one area and not associated with other symptoms and goes away in a few hours or days, you don’t need to see a doctor.”
The thing about fasciculations in the arch muscle of your foot is that this location makes the experience particularly bothersome.
But just because something is bothersome doesn’t mean you should worry about it.
What could be the cause of the twitching in the arch of your foot anyways?
Many things could explain it.
Dr. Dombovy says, “Some common causes of muscle twitching include exercise, particularly prolonged exertion, electrolyte abnormalities, muscle or nerve injury, muscle or nerve disease (most of which is not ALS).”
Shutterstock/ Phase4Studios
Though “muscle and nerve disease” are mentioned here, this does not mean that these are the most likely causes of your situation.
They are in the list because these conditions can cause fasciculations. So can Lyme disease, which is caused by getting bitten by a tick.
The arch of the foot takes a good beating every day; all your body weight is on it as you walk and especially as you exercise. This area is subject to plenty of fatigue.

Shutterstock/zoff
Don’t forget that inadequate water intake can also cause fasciculations, and so can insufficient potassium and magnesium, two important minerals.
The key is if you have other symptoms such as weakness, numbness, cramping or pain.
However, cramping could be the result of an overworked arch muscle or even improper footwear.
Pain can be from plantar fasciitis, a benign but sometimes very painful condition. If discomfort is troubling, see a doctor.
“Neurologists have the expertise to sort out the cause by taking a complete history, performing a clinical examination and often performing nerve conduction studies/electromyography, and blood tests,” says Dr. Dombovy.
“If the cause is benign and the symptoms quite bothersome, there are also medications that can help decrease the twitching.”
Dr. Dombovy completed her neurology residency at Mayo Graduate School of Medicine. She is board certified in both neurology and physical medicine and rehabilitation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}