

Climbing Hand Pain & Cramps from Climbing: Solution

Did you hurt your fingers rock or wall climbing and now they’re too painful to crimp or grip hand-holds or even do any kind of pulling?
Other symptoms of this common climbing injury are that of awakening with stiff, crampy fingers, and also you feel cramping or pain when trying to grip something, or holding something heavy that has a handle where you curl your fingers around.
The remedy I’m about to describe is based on my own climbing experience, after diagnosing myself with annular flexor pulley injury.
I did hand grips for three weeks and also avoided climbing altogether, and after three weeks, there was NO improvement whatsoever.
I then found a rehab website that said the solution is eccentric exercise (the site then charged a fee for more details). Fortunately, as a personal trainer, I knew what eccentric exercise meant.
Remember that I said hand grips were useless? That’s because I used them the standard way. Use them eccentrically.
To heal painful fingers from climbing
Assume that your symptoms are as described in this article, and especially if you believe that the injury is the result of hanging too much body weight while supporting yourself with a two- or three-finger hold, or pulling yourself up on such a hold:
- Position your grip on a V-shaped hand gripper tool.
- With free hand, close your gripping hand while it holds the gripping tool. Do not squeeze the gripping tool closed with your injured fingers! Let your other hand do this.
- After closing your hand with your free hand, release your free hand, and keep the gripping tool closed.
- Now, VERY SLOWLY release the grip. Do this VERY SLOWLY. The release should take at least 7 seconds, up to 10, depending on the tool’s tension.
IMPORTANT: There should not be any pain. If you feel scary pain, STOP and consult with a physician. My fingers were not swollen and I had no reason to believe anything was torn.
The exercise did not cause me pain, and unless you have a serious injury, it should not cause you pain.
- Once it’s released, close your hand back up with your free hand, and repeat the SLOW release.
- Do this eight times, then switch hands if the other is also injured. Do three sets per hand…three times a day.
- After every session, soak your painful fingers in hot water for 15-20 minutes to increase blood circulation—something I decided to do at the onset of the eccentric program.
Thus, I don’t know what percentage the exercise contributed to healing my climbing injury, versus the hot water—but do BOTH.
You’ll need to replenish the water if it’s in a bowl to keep it hot. Keep fingers completely submerged.
The starting point for the water should be hot enough that you can barely tolerate the submersion. Warm is not good enough. It must be HOT. If you can’t maintain submersion, wait a few minutes.
Within a few days of doing this, I finally began feeling an improvement in my hurting fingers—and the situation resolved.
As you feel definite improvement, go up to 10 reps, then 12. Give it time; the cure to this climbing injury won’t be overnight.
This plan is well-worth the try to heal painful or cramping fingers from the typical climbing injury.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Burning, Sharp or Stabbing Pain Near the Vagina: It’s for Real

If you suffer from a stabbing or burning pain near your vagina, it has a name, and more women than you think have it.
According to one study (Reed et al, American Journal of Obstetrics and Gynecology), over 25 percent of women have experienced stabbing, burning or sharp pain about their vagina.
“Causes are vulvodynia, vestibulitis, Bartholin cyst or abscess, any type of vaginitis, herpes simplex, round ligament pain during pregnancy,” says Dr. Vivika Joshi, OB/GYN at Dr. Felix Online Pharmacy.
“Vulvodynia is a poorly understood condition that produces burning and sharp pain around the vaginal opening or vulva,” explains Dr. Joshi.
“Other common symptoms are soreness, stinging, searing, throbbing, rawness, pain and fear of speculum insertion during pelvic exams.
“Pain with intercourse and subsequent relationship problems are commonplace.
“Most of these women avoid activities that aggravate the symptoms such as bike riding, wearing tight jeans or clothes, prolonged sitting; even walking can trigger the pain.”
You now know it has a name and is a well-documented medical condition: vulvodynia.
What’s really alarming about vulvodynia is that, according to the women in the AJOG study, it’s a very much misdiagnosed condition.
Only two percent of the women in the study sought medical attention for the symptoms, not knowing what they had.

Shutterstock/siam.pukkato
However, of these patients, only five percent were diagnosed with vulvodynia.
The misdiagnoses were those of estrogen deficiency or yeast infection. Not surprisingly, the treatments that ensued were useless—evidence supporting the misdiagnoses.
What is the cause of vulvodynia?
“Causes of vulvodynia is presumed to be allergens, history of bedwetting, early age of menarche, and a history of yeast vaginitis — either repeated episodes or one very severe case,” says Dr. Joshi.
“A history of sexual assault has been described as a risk factor, but this has not been substantiated.
“An underlying psychological cause has been disproven since studies show similar psychological profiles in women with vulvodynia.
“Subsequent psychological issues may ensue when a patient is dismissed and not taken seriously with their symptoms.”
Vulvodynia is not “all in the head.” How can anyone imagine stabbing, tearing, stinging pain?
A pain that’s described as burning, sharp or raw is not the product of imagination.
“This is a very real and complicated condition associated with chronic inflammation, increased vascularity and nerve overgrowth,” says Dr. Joshi.
How to Calm Down that Burning, Stabbing Vaginal Pain
“Systemic/oral drugs that target ove active nerves like Gabapentin are more effective than tropical agents that can aggravate the symptoms,” says Dr. Joshi.
“The fact that a ‘nerve calming’ drug like Gabapentin improves symptoms is further proof that this is a real medical condition.
“Avoidance of any chemicals, lotions, perfumed soaps and prolonged exposure to hot tubs is recommended.
“Cold packs for acute pain are a better choice than topical lidocaine.”
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
,
Source: sciencedaily.com/releases/2011/09/110914131354.htm

How Likely Is Rectal Bleeding Caused by Colon Cancer?

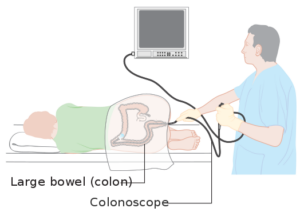
The rectum is the lower portion of the colon. What are the odds that any rectal bleeding is a sign of colon cancer?
“Most often there are no symptoms in early stages,” says Dr. Maxwell Chait, MD, gastroenterologist at ColumbiaDoctors Medical Group in Westchester County, NY. By the time a person begins having signs of CC, it’s almost always in an advanced stage.
“Rectal bleeding is only one symptom of colon cancer,” continues Dr. Chait.
“Rectal bleeding is most often microscopic in colon cancer shown by an occult blood test of the stool.
“Less than 20 percent of rectal bleeding cases are due to colon cancer.”
What is this disturbing rectal sign usually more indicative of, then? Dr. Chait says that it’s “more often associated with hemorrhoids, rectal fissure, bleeding from a colon diverticulum,” and the following additional problems can cause the symptom:
A vascular malformation of the colon called angiodysplasia
A saccular out-pouching of the structure
Other common indications of CC include: “Abdominal pain, weight loss and a change in bowel habits, such as diarrhea or constipation, narrowing caliber of the stool, depending on the part of the colon where the cancer occurs.”
More colon cancer symptoms occur when the malignancy is on the left rather than right colon.
Dr. Chait urges that people get screening for this disease.
This is done by a colonoscopy, during which the precursor to a malignant tumor, called a polyp, can be removed, thus preventing the disease.
Cancer Research UK
For average people, the time to get the first colonoscopy is at age 45, and then every 10 years after that.
If there is a family history of colon cancer under the age of 65, then a person should begin screening at an earlier age.
Your doctor can recommend what age this should be, based on your and your family member’s medical history.
During a colonoscopy, the patient is comfortably sedated and will often sleep through the procedure, which typically lasts around 30 minutes to up to 45 minutes.

Dr. Chait’s practice interests include digestive conditions such as colon cancer, gastrointestinal endoscopy and internal medicine. He has authored numerous publications in reputed journals.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Ovarian Cancer vs. Colon Cancer: Symptom Comparison

Because symptoms of ovarian and colon cancer overlap quite a bit, women need to be extremely vigilant about what’s going on in their bodies.
Is there a way to tell the difference between ovarian cancer symptoms and those of colon malignancy?
In ovarian cancer, “GI symptoms are common because the ovaries are so close in contact with the GI tract,” says Dr. Maxwell Chait, MD, gastroenterologist at ColumbiaDoctors Medical Group in Westchester County, NY.
“There can be warning symptoms of ovarian cancer and can be present for up to one year before diagnosis.
“They may include intermittent abdominal bloating and distention, change in bowel habits — either diarrhea or constipation often unrelated to meals or specific foods, and lower abdominal pain.”
It’s not uncommon for women with these symptoms to repeatedly visit gastroenterologists to find out what’s wrong, and not even consider seeing a gynecologist.
They may even end up undergoing a colonoscopy (which turns out normal), having no idea that ovarian cancer has brewing all along.
Colon malignancy gets ruled out, and the patient may end up trying all sorts of medications to relieve what she still believes are GI symptoms.
As ovarian cancer becomes more advanced, the symptoms become more persistent and may include unexplained weight loss and urinary problems, adds Dr. Chait.
In ovarian cancer, there are no bloody stools, but this can be a colon tumor symptom.
However, not all CC cases produce visible blood in the stools!
Malignant colon disease can result in very skinny or ribbon-like stools, whereas ovarian malignancy won’t cause this; however, not all colon cancers cause skinny stools!
Both of these diseases can produce the symptoms of:
Alternating Diarrhea with Constipation
Abdominal Pain/Cramping
Unexplained Weight Loss and Fatigue
Appetite Suppression
Bloating
Gas
Nausea
Both can also cause back pain, though OC can cause leg pain and pelvic heaviness that are not part of the symptom repertoire of CC.
Dr. Chait adds the following information:
“If symptoms persist for more than 2-3 weeks, they should see their doctor.
“May first be interpreted as irritable bowel syndrome
“Colon cancer screening is as important for women as for men since no sex difference.” (Screening should begin at age 45 for those at average risk, male or female.)
“You want to find a premalignant lesion as a colon polyp that has no symptoms before a cancer develops.
“GYN exam screening for women with persistent lower GI symptoms.
“You want to find an ovarian cyst or other premalignant lesion before cancer develops.
“Colon and ovarian cancer have an association in the genetic colon cancer disorder HNPCC; 10% of women can also have ovarian cancer.”
Dr. Chait’s practice interests include digestive conditions such as colon cancer, gastrointestinal endoscopy and internal medicine. He has authored numerous publications in reputed journals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/gpointstudio
Source: mayoclinic.com/health/ovarian-cancer/DS00293/DSECTION=symptoms
Can Excessive Burping Mean Cancer?

Believe it or not, frequent burping can be caused by several different cancers.
A symptom as seemingly harmless as burping can actually be a sign of cancer.
“Cancer can affect motility of the GI tract, increasing gas and belching either directly by invading the stomach, or by distal and hormonal effects affecting the motility of the upper GI tract,” says Dr. Maxwell Chait, MD, gastroenterologist at ColumbiaDoctors Medical Group in Westchester County, NY.
What cancers can lead to excessive burping?
“Cancers of the organs adjacent to the stomach such as stomach cancer, esophageal cancer, cancer of the liver and biliary tract and pancreas cancer all can do this,” says Dr. Chait.
If stomach cancer is present, burping may be accompanied by other symptoms like persistent nausea, abdominal pain and unexplained weight loss.
Burping can occasionally be a sign of esophageal cancer, especially if it’s accompanied by difficulty swallowing down food, forcing a transition to soft foods and eventually regurgitating food because it can’t go down.
Burping may rarely occur with liver cancer, but if it does, there’ll probably be other symptoms such as suppressed appetite, yellowing of the skin, upper right abdominal pain and fatigue.
Biliary tract cancer blocks bile flow which can lead to buildup of stomach gases: burping.
Pancreatic cancer can lead to gas buildup as well, leading to increased burping.
But burping without other concerning symptoms such as unintentional weight loss or grey bowel movements will not put cancer on the radar for your doctor.
“GERD is one of the most common causes of belching (burping) in the U.S. as well as Western Europe,” adds Dr. Chait.
GERD stands for gastroesophageal reflux disease.
“It is associated with a condition called Barrett’s esophagus,” continues Dr. Chait.
“This is a premalignant disorder of the lower esophagus that is associated with cancer of the esophagus.
“This is one the fastest growing cancers by incidence in the U.S. Remarkably, its highest incidence is in older white males.”
In other words, if you’ve been diagnosed with GERD, it’s absolutely mandatory that you take this seriously and don’t dismiss it as some harmless condition just because you’ve seen goofy TV commercials about “acid reflux.”
Dr. Chait adds, “GERD can be silent, especially in the older population who have reduced symptoms but often more severe disease.
“It can present with only upper abdominal pain or spasm.
“Nighttime GERD may go unnoticed except for poor sleeping and be associated with sleep apnea.
“Other important symptoms are difficulty swallowing, painful swallowing, chest pain, anemia, weight loss or intestinal bleeding. One should see their doctor if any of these symptoms occur.”
Excess burping can also be caused by a hiatal hernia.
A lot of burping may seem funny, but now you know that it can be a sign of cancer and thus warrants a medical checkup.
Dr. Chait’s practice interests include digestive conditions such as colon cancer, gastrointestinal endoscopy and internal medicine. He has authored numerous publications in reputed journals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/TunedIn by Westend61
Source: mayoclinic.com/health/hiatal-hernia/DS00099/DSECTION=symptoms

How Are Fibromyalgia Symptoms Similar to Depression’s?

Fibromyalgia symptoms vs. depression symptoms: Just how similar are the symptoms of these conditions anyways?
After all, both cause pain, and both can cause brain fog and fatigue.
Fibromyalgia can leave a person feeling very depressed — after the fact.
And it’s possible to have both these conditions, independent of each other.
“These are two very different conditions,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
Depression can be primary, or secondary, i.e., the result of a disabling illness.
One in eight people with fibromyalgia have secondary depression, says Dr. Teitelbaum.
“But they are two separate processes, and therefore do need to be addressed separately,” he further explains.
“The problem usually occurs when physicians mistakenly blame the fibromyalgia symptoms on depression, trying to invalidate the person’s illness.
“This is the same as telling somebody with metastatic cancer that they’re just depressed – and then trying to convince the family that the person is crazy and denying them health and disability benefits because of this. It is not only incorrect and unethical, but it is also abusive.”
Symptoms of fibromyalgia
Body-wide pain, sleeping difficulties, considerable exhaustion and even some compromise of mental function.
These symptoms can also describe severe primary depression. In fact, they can also describe low thyroid!
However, a diagnosis of low thyroid can easily be made or ruled out with a blood test.
Can you tell the difference between depression and fibromyalgia?
“Depression is usually associated with sadness and lack of interests,” says Dr. Teitelbaum.
“Fibromyalgia is usually associated with many interests, but with frustration over lack of ability to do them,” he continues.
“Biochemically, they are also very different.” An example is that “cortisol levels are usually high in depression, but tend to be low in fibromyalgia.”
Cortisol is a stress hormone.
“Overall, they are very different conditions, but which may both be present in the same person.”
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Fever Feeling with Fibromyalgia: Causes, Treatments

Many with fibromyalgia experience a fever-like feeling, but there is something you can do to help alleviate this.
If you have fibromyalgia and feel like you have a fever, this doesn’t mean you actually have a fever.
“Although people with fibromyalgia often feel feverish, they normally have low temperatures under 98,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
“I consider anything over 98.6 to be a fever in fibromyalgia,” he continues. “If chronic persistent temperatures over 98.6 are present, I look for evidence of infections (e.g., sinus, dental, lung or bladder).”
You can have one of these infections and not even know it, other than being aware of the fever feeling.
“For sinusitis, treatment with antifungals are necessary, as this is the root cause of sinusitis,” says Dr. Teitelbaum.
In people with this pain disorder who feel as though they have a fever, there is usually no infection source to be found, adds Dr. Teitelbaum.
“In these cases I do recommend an empiric trial of the antibiotics doxycycline or Zithromax for six weeks to see if it helps the fibromyalgia.
“Also, have you ever had a course of antibiotics that also improved your fibromyalgia symptoms?
“I am amazed at how often the answer is yes, but then the doctor refuses to repeat the antibiotics.”
For these particular cases, Dr. Teitelbaum prescribes an extension for the antibiotic that had improved the symptoms of the mysterious pain disorder.

Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why Fibromyalgia Can Cause Scalp Pain; Treatment

It’s no secret that fibromyalgia can cause pain in your scalp, and many frustrated patients suffer with this problem.
The pain of fibromyalgia is body-wide, so it shouldn’t be surprising that it extends to the scalp. Nevertheless, why does this occur?
“This often comes from the scalp muscles being tight if it’s diffuse,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
“…or can be referred to the top of the head from neck muscles where they attach to the skull,” he continues.
“In addition, allodynia is another kind of pain that may be present in fibromyalgia.” Allo means other, and dynia means pain.
“Allodynia refers to when light touch on the skin is painful,” adds Dr. Teitelbaum.
“It is associated with increased activity of a neurotransmitter called NMDA, and generally responds to overall treatment of the fibromyalgia.”
So what treatment is best if you have scalp pain coming from fibromyalgia?
Dr. Teitelbaum recommends the low cost generics Ultram and Neurontin over the pricey and, as he says, less effective Savella, Cymbalta and Lyrica.
He also recommends End Pain by Enzymatic Therapy, and Curamin by EuroPharma.
For both of these, take two caps three times daily, over six weeks to reap the full effect. Then the dose can be lowered.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Difficulty Breathing, Tight Chest & Fibromyalgia: Solutions

Fibromyalgia may actually be the cause of your shortness of breath and tight chest, so here’s what a top FMS doctor says you can do about it.
“Shortness of breath, or a sense of breathlessness, sometimes associated with chest tightness is a common symptom in fibromyalgia,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
There are three main categories of breath shortness in ibromyalgia, says Dr. Teitelbaum:
Exertion-caused shortness of breath and/or chest tightness
This may be angina and thus requires testing by a cardiologist. “Once heart problems or lung problems are ruled out,” says Dr. Teitelbaum, “then treatment with ribose, coenzyme Q 10, and acetyl-L-carnitine can help.”
Feeling like you can’t take a deep enough breath, with no accompanying anxiety or dizziness?
“This is very common and likely comes from tight muscles in the chest,” says Dr. Teitelbaum.
“An excellent study over 15 years ago by the acupuncturists and physician Neoh Aum Choo, MD, showed that three acupuncture points at the base of the skull on each side could relieve this sense of breathlessness in fibromyalgia,” continues Dr. Teitelbaum.
“Simply putting pressure on, or massaging, these points can be very helpful in relieving the feeling of shortness of breath.”
Hyperventilation
“When the shortness of breath is associated with feeling of inability to take a deep enough breath, numbness and tingling in the fingers and especially around the lips, and anxiety,” begins Dr. Teitelbaum, “it most often comes from hyperventilation.
“This is basically a severe anxiety attack, where feelings that have been buried earlier bubble to the surface during periods of relative calm.”
This explains why these attacks typically occur when you are relaxed watching TV or reading—stress-free activities.
“Taking rapid deep breaths for 30 to 60 seconds will dramatically flare symptoms confirming the diagnosis,” continues Dr. Teitelbaum.
“Unfortunately, this can also trigger a full-blown panic attack.” Thus, it’s advisable to do this at home.
“Doing calming exercises, as well as letting your stomach expand out at the end of each breath will allow more air into your lungs and can also help end the hyperventilation attack.”
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Aaron Amat

Twitching Muscles and Fibromyalgia: Natural Solutions

A leading fibromyalgia expert comments about muscle twitching and what you can do about this.
Many people with fibromyalgia experience twitching of their muscles. This can be very annoying and even interfere with sleep.
“Muscle twitching, called fasciculations, are very common in fibromyalgia,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
“They will decrease after proper treatment with the SHINE Protocol for fibromyalgia (Sleep, Hormones, Infections, Nutrition, Exercise),” continues Dr. Teitelbaum.
People without the pain disorder have been known to experience a lot of benign muscle twitching, and one of the most recommended solutions is magnesium.
“Magnesium is especially helpful,” says Dr. Teitelbaum. This is because this mineral, if insufficient in your body, can lead to fasciculations or make existing fasciculations more pronounced.
The SHINE Protocol consists of:
• Sleep. Get 8-9 hours!
• Hormones. See an endocrinologist to get tested for any hormone deficiencies.
The blood testing is very thorough but worth it, as hormone deficiencies can play a role in your pain disorder.
• Infections. An infection can contribute to, or even cause, FMS. You may have an infection and not even know it.
A perfect example of a sneaky infection is that of sinusitis, which can cause headaches that you think are solely caused by fibromyalgia! Get prompt treatment for all infections.
• Nutritional supplements. Acetyl l-carnitine, glutathione and vitamins A, the B’s, C and D will help reduce muscle twitching when taken in therapeutic doses.
• Exercise. Though FMS can cause exercise intolerance, following the four steps above will increase your tolerance.
Muscle twitching is most pronounced during inertia.
If you have fibromyalgia, exercise as well as you can, but keep in mind that exercise — particularly vigorous — can cause fasciculations (which is perfectly normal).
In fact, only the secondary mover in a strength exercise (e.g., triceps in the bench press) might end up being the muscle with the twitchies.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}