

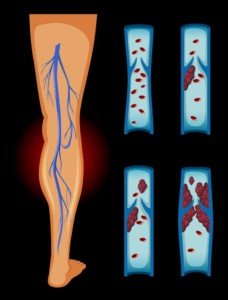
Should You Avoid Running with a DVT in Your Leg?

Running with a DVT? Risky or safe?
“Since running would significantly increase arterial flow to the lower extremities, and therefore venous return is also increased, it may be safer to avoid running in the ACUTE (when the clot is fresh and prone to breaking off) period,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
That makes a lot of sense, even though it’s not the news that an avid runner wants to hear.
Dr. Gashti continues, “After 2-3 weeks, these clots become more chronic, and risk of embolization would be decreased.”
There is another important factor to consider, however:
“What I will be more concerned about in someone with an acute DVT and running is that they most likely would be on anticoagulation (coumadin), and they have to be careful not to fall or sustain any other injury, since the risk for massive bleeding would be increased while on this medicine.”
Signs of a DVT
- Unexplained redness or ruddiness in a localized area of the leg, particularly the calf
- Soreness or discomfort in that area — not just when walking or using a staricase, but also at rest; sitting down or lying down does not relieve the pain. This is concerning.
- The area (which may not be red) seems unusually warm to the touch.
- If part or all of such a blood clot breaks loose and travels to the lungs, common symptoms would be chest pain and/or difficulty breathing.
- It is estimated that about half of DVTs do not present with symptoms involving the leg or pelvic area where the clot is, but this doesn’t mean it can’t dislodge and get into the lungs.
If you’re a runner and have recently sustained a very long plane flight, and you develop a mysterious cramping or pain in a leg, especially a calf, pay very close attention to this.
It would be a safe choice not to run until you’re sure that you don’t have a DVT.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: ©Lorra Garrick

DVT in Your Calf: Is Lifting Weights Safe or Out?

Can working out with weights harm that DVT in your calf or possibly help dissolve it?
Being that a sedentary lifestyle is one of the many risk factors for a deep vein thrombosis, it’s fair to wonder if lifting weights with a DVT in one’s lower leg could actually help improve the situation.
On the other hand, it’s equally as compelling to wonder if strength training could make the blood clot worse.
“Our management of DVT is very different now as opposed to several years ago,” says Dr. Moji Gashti, Chief, Division of Vascular Surgery, Department of Surgery, Union Memorial Hospital, Baltimore, MD.
Dr. Gashti continues, “It used to be that these patients would be on bed rest for days before they were allowed to ambulate.”
The irony with that is that excessive bed rest is another risk factor for a DVT.
“These days, however, we have them ambulate right away and carry on with their normal activities.
Lifting Weights with a DVT
“Lifting weights would actually produce a valsalva maneuver, which, if anything, would actually reverse venous blood flow from your lower extremities (towards your feet), and therefore should not cause any problems.”
The valsalva maneuver is practiced by some weightlifters and bodybuilders.
It’s when a person holds their breath while bearing down — like you might do when straining to push out a very hard bowel movement that doesn’t want to exit.
Upon straining to push against resistance at the gym, a person may find themselves bearing down — holding their breath as they strain with the lift rather than exhaling.
However, not all people who lift weights do this; most exhale against the lift.
If you do not employ the valsalva maneuver during your strength training, you should ask your doctor what he thinks about working out with a deep vein thrombosis.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Is Peripheral Vascular Disease Pain Similar to Spinal Stenosis?

Spinal stenosis and PVD (peripheral vascular disease) both cause “leg pain.”
Is there a way to tell the difference between these two conditions?
“The pain from PVD, referred to as intermittent claudication, is very different from pain from spinal stenosis,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
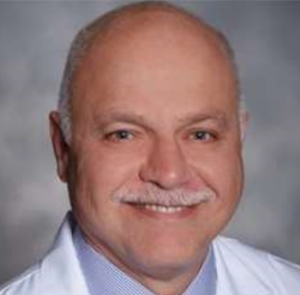
“Peripheral vascular disease typically causes achy, crampy pain in a certain muscle group supplied by a certain artery, most commonly calf muscles, after walking a certain distance,” says Dr. Gashti.
“The hallmark of pain caused by PVD is that it is very reproducible; since the arterial occlusion is a constant, meaning the blockage is there every day, patients complain of experiencing calf pain EVERY TIME they walk from point A to point B.
PVD. National Heart Lung and Blood Institute/Wikimedia Commons
“Pain that presents different than this should raise other possibilities.
“Spinal stenosis causes compression of the nerve roots/spinal cord and typically presents with a burning, or pins and needles kind of pain that may have no relation to walking at all.
“It can occur at rest, while sitting, flat in bed, or walking. It is typically very variable in presentation.”
Spinal stenosis can be confirmed with an MRI.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Beauty Studio

DVT Calve Pain vs. Pulled Calve Muscle Soreness

Can DVT pain in the calve, and the pain of a pulled muscle in the calve, be distinguished?
DVT stands for deep vein thrombosis: a blood clot.
A blood clot in the calve can cause aching or discomfort. So can a pulled or strained muscle in this region.
If there a way to tell the difference between blood clot pain and that which results from a sore or pulled muscle in the calve?
“It is going to be difficult,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“Both most likely would present with achy kind of pain,” continues Dr. Moji.
“Perhaps the history may be more important here; a pulled muscle most likely would happen with some kind of trauma or activity as opposed to pain related to deep vein thrombosis, which most likely would happen in an individual after some inactivity (post-op, cast, long trips, etc.).
“The pain from DVT most likely would also come about slowly rather than suddenly, and be associated with swelling.”

DVT in lower leg. James Heilman, MD, CreativeCommons
As you can see, a better way to tell the difference between a DVT and a pulled muscle is by evaluating the preceding activity—or lack thereof.
The suspicion for a DVT is heightened if the symptom of what feels like a pulled muscle in one of your calves is accompanied by a redness or warmth in that area, and the discomfort persisting even when you’re seated and not moving the leg.
Another suspicious symptom is that of tenderness to the touch.
Nevertheless, if you suspect a blood clot, head immediately to the emergency room. An ultrasound can make the proper diagnosis.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Shaynepplstockphoto

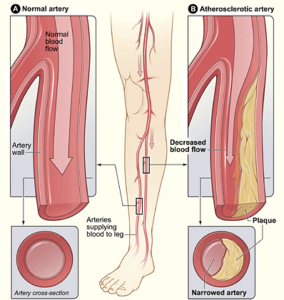
What Parents Should Know About Concussions: Truth vs. Myths

Concussions are far more common in athletic kids and teens than parents realize, and their child could have had a few concussions without the parents ever knowing.
Many parents continue to be grossly uninformed about concussions. How many parents, for instance, even know that nausea is a sign of a head injury?
The nausea from a concussion can occur hours after the injury, too, but by coincidence, shortly after their teenager ate a lot of French fries and ice cream.
Situations like this could make a parents think that the nausea is from the eating (and it could be), but … a bleed in the brain can produce nausea.
Many kids keep their head bangs a secret, and when they themselves don’t even know that their new-onset symptoms are being caused by a concussion (e.g., drowsiness), this makes it even less likely that the parents will find out what really happened and get medical help.
It’s alarming how uninformed so many parents and others are about concussions.
The myths continue to swirl out there, and not knowing the truth can be deadly.
The following concussion myths and truths come from Chris Hummel, certified athletic trainer and clinical associate professor, Ithaca College’s Department of Exercise and Sport Sciences.
MYTHS
Normal CT scan means no concussion.
Hummel says that a neuro-metabolic event, triggered by trauma, causes a concussion.
This involves chemicals, not brain structure. A CT scan cannot detect chemical imbalance. “CT scans can only view structural damage.”
A concussion is worse if you’re knocked unconscious versus not losing consciousness.
Says Hummel, “In some cases, individuals who are knocked out may suffer less severe trauma.”
He adds that a patient need not lose consciousness to suffer serious injury.
My mother had to have two brain surgeries to drain bleeding and fluid buildup after hitting her head, even though she never lost consciousness.
The harder the impact, the worse the injury.
Hummel says, “Any contact to the head or body that causes rapid head movement can cause a concussion.”
He adds that repeated, lighter impacts over time may be more injurious than one impact of great force.
Helmets will prevent concussions.
Hummel says that helmets are “designed to prevent skull fractures, not concussions.” During impact, the brain still moves like jello while the head is helmeted.
TRUTHS
A history of concussion makes you more likely to experience another.
This isn’t because you’re more likely to continue contact sports; it means that “the threshold for sustaining another concussion can be diminished,” says Hummel.
Beware of second impact syndrome, in which severe trauma or death can result if one suffers a head blow before fully recovered from the first impact.
No two concussions are alike.
Patients should be treated individually rather than cookie-cutter style.
If you suspect a concussion, assume you’re right and proceed to a medical evaluation.
If your gut instinct says head to the emergency room, then do so.
It’s unlikely that one of the regrets you’ll ever have in life is that of spending time waiting around in the emergency room for test results that turned out to be normal.
Nobody kicks himself for having taken the time to get a thorough medical evaluation that turns up negative.
Concussions are a very real problem in youth sports.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: sciencedaily.com/releases/2012/03/120329170220.htm

How Does Melanoma Get on the Bottom of a Toe?

It’s true: People have been diagnosed with melanoma on the BOTTOM of a toe–a place that’s almost always in total darkness.
How the heck is this possible?
“Yes, melanoma can exist anywhere,” says Rebecca Baxt, MD, a board certified dermatologist in NJ.
How does melanoma end up on the bottom of a person’s toe?
Dr. Baxt explains, “No one understands it completely. Even where the sun doesn’t shine. There are causes that we don’t fully understand.
“We know that sunburn is a risk factor and that ultraviolet light can cause skin cancer, but we don’t know why these cancers occur all over the body.”
For women, the highest risk area of developing this deadly skin cancer is on the calves and back of the legs, and for men, the highest risk area is the back.
“If it were just about sun exposure, you would think all the skin cancers would be on the face and arms, but that’s not true,” adds Dr. Baxt.
Do skin exams once a month, and check everywhere, including the bottom of your toes, since the “seeds” for melanoma may have been planted during childhood sun exposure to the bottom of your toes while you were playing outside barefoot or lying beside the pool.
How to Check the Feet for Melanoma
Your feet, along with the rest of your skin, should be self-inspected every month for suspicious signs of cancer.
Use a hand mirror and position it under your foot and toes.
If you’re flexible enough, place your foot in the bathroom sink while standing on the other foot.
Place the mirror under your foot and toes. People who practice yoga or martial arts will have no problem doing this.
Don’t hesitate to ask your partner to inspect your feet and under the toes for signs of melanoma which include a dark spot that was never there before, or a pre-existing mole that’s getting bigger or changing shape.

Dr. Baxt is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Can Sphenoid Sinusitis Headaches Occur Every Day?

“The sphenoid sinus can be affected by an acute bacterial infection, chronic inflammation or a cyst or a polyp,”
says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
“An acute infection can cause severe headaches on the top of the head,” continues Dr. Silvers.
“The location of the sinus is located between an intersecting line from the top of the head down and between the ears.
“Located in the back of the nose. If the infection is bacterial, then the headache will be persistent until the infection is treated.
“Patients with chronic sinus congestion will have fluctuating headache symptoms depending on the barometric pressure, environmental allergens or a mild URI (which cause and increase obstruction swelling around the doors of the sinus and therefore an increase in sinus swelling).
“As we are all exposed to environmental stimuli, it is patients with prior structural narrowing who are at higher risk for sinus symptoms when specific allergens are present.
“Patients are usually asymptomatic from a small polyp or a small cyst in the sphenoid sinus.”
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Stiff Tongue: 10 Possible Causes Including Cancer

Have you noticed that lately, your tongue is rather stiff?
There are a number of possible causes, according to Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology (ear, nose and throat).
List of possible causes of a stiff tongue
Dr. Silvers says, “Many things can affect the tongue: poor oral hygiene, different medications, infection, vitamin deficiencies, Sjogren’s syndrome, yeast infections, acid reflux, smoking and other tobacco use, excessive coffee intake and dehydration.”
Sjogren’s syndrome, which affects mostly women, is an autoimmune disorder characterized primarily by impaired secretion of moisture by the lacrimal glands (tear glands of the eyes) and salivary glands.
The resulting dry mouth can lead to a feeling that your tongue is stiff.
A dry mouth can cause a stiff tongue.
Dr. Silvers continues, “Unless a patient has an issue with the salivary glands in general (Sjogren’s syndrome or a history of radiation to the oral cavity), then one blocked salivary gland by a calcification will not affect oral dryness, as the minor salivary glands play a large role in hydration.
“Diagnostic testing involves reviewing diet and tobacco use.”
A doctor will also want to know about any medications that you began taking at around the time you started noticing that your tongue was getting stiff.
A physician may also want to take blood work to test for an underlying connective tissue disorder, adds Dr. Silvers. “Medications like Salogen (3-4 x per day) can improve oral hydration.”
Cancer
Unfortunately, cancer of the tongue itself can cause it to be rigid, with reduced movements.
This occurs because the cancerous cells invade and disrupt the normal tissue structure, leading to several physical changes in the tongue.
As the tumor grows, it invades the surrounding muscle tissues of the tongue.
This invasion leads to stiffness and rigidity because the malignant cells replace or disrupt the normal muscle tissue.
Plus, the presence alone of the tumor can limit the tongue’s ability to move freely.
This restriction is due to both the physical mass of the tumor and the inflammation or scarring that accompanies the cancer growth.
Are you at risk?
The main risk factors for tongue cancer are smoking, heavy drinking and an HPV infection.
Additiona risk factors are as follows: Chronic irritation from poor oral hygiene, such as persistent inflammation or infection, can increase the risk.
A diet low in fruits and vegetables and high in processed or salty foods can contribute to an increased risk of tongue cancer.
Persistent irritation from ill-fitting dentures or rough teeth may also bump up the risk.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Koldunov Alexey

Can an Irritated Trigeminal Nerve Be Buzzed by Nose Gunk?

Nose gunk or mucus builds up in the sinuses where the trigeminal nerve begins. Can this crusty mucus actually irritate this nerve?
What is the trigeminal nerve?
There are 12 cranial nerves. The trigeminal is one of them: the fifth.
It sends sensations to your face, nasal passages and other head structures. It also supplies movement to the jaw.
Fun Fact: Ever notice that when you feel a sneeze coming on, but it just won’t come – but if you look directly at a bright light above, it brings on the sneeze?
This is because the trigeminal nerve, if irritated, can cause a sneeze – and this complex motor nerve is located close to the optical nerve.
Now that’s something you can bring to the water cooler.
“Trigeminal neuralgia is a chronic irritation of the trigeminal nerve,” explains Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
“It is thought to be related to compression of the nerve by a mass, trauma directly to the nerve and/or effects on the blood flow near the nerve,” continues Dr. Silvers.
“The dry mucus in the nose is irritating and can cause nasal pain; this is not trigeminal neuralgia.”
Yucky Gunk in the Nose
This, too, can cause a two or three sneezes in a row.
“Dry mucus can cause nasal crusting and nosebleeds with painful scabs,” says Dr. Silvers.
“Cultures for Staph infections should be done for non-healing nasal dryness and scabbing.
“Changes in climate, altitude and humidity are common causes of dryness and crusting in the nose.
“Treatment for this is over the counter nasal moisturizing ointments or sprays, humidifiers or prescription nasal ointments.”
When spraying, aim the stream at an angle rather than straight up your nose.
This will reduce the amount of trauma to the tiny blood vessels in the nasal passages — and minimize tiny bleeds.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Can Neck Pain Be Triggered by Sinusitis?

Have you been having pain in your neck lately?
Most people will think it’s from a neck source, but what about the sinuses? Is this possible?
“Chronic sinusitis can cause neck pain,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
Dr. Silvers continues, “The direct cause may not be known. There are no sinuses in the back of the head and there is no direct causation of the symptoms.
“However, neck pain can occasionally be a complaint with acute or chronic sinus infections.
“The neck is the support structure for the head. When the head is congested, inflamed and blocked, the neck has more to support, and the way we support our head may differ depending on the degree of discomfort.”
It’s also possible that, due to the sinusitis being, figuratively speaking, a pain in the neck, the patient assumes slumped posture or excessive sleep — both of which can cause tension in the neck muscles.
See if some self-massage won’t help alleviate the discomfort. Maybe a brisk walk for five or 10 minutes will do the trick, if the discomfort is musculoskeletal in origin.
Briskly walking will loosen up these muscles and increase blood flow through them. A warm compress may also help.
Dr. Silvers explains more about neck pain and sinusitis.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}