

How Common Is Melanoma Black; Can a Normal Mole Be Black?

A dermatologist discusses how often a mole with melanoma is a black color.
I wondered how common is it that a melanoma lesion is black — not dark brown, but true black. And can a perfectly normal mole be black?
“Yes, normal moles can be black, more commonly in darker skinned individuals,” says Dr. Rebecca Baxt, a board certified dermatologist with Baxt CosMedical.
“Most moles are brown, but some can be pink or black,” continues Dr. Baxt. “Generally, darker skinned people get darker moles; fair skinned people get lighter moles.

“The general rule is if it’s new or changing, it needs to be evaluated by a doctor, preferably a dermatologist.
“If the mole has changed and turned black, that mole needs a biopsy to rule out melanoma.”
Melanoma can definitely appear black (top image and below).


Can a normal mole be black?
“There are other reasons a mole could turn black such as trauma, but melanoma should be ruled out,” says Dr. Baxt.
“Moles can definitely change during pregnancy. They can grow and get darker and they need close follow-up by a dermatologist.
“I always tell my patients to follow up with me more often when they are pregnant and not less often. Self-tanner can make moles look darker temporarily.”
Dr. Baxt is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Image 2 and 3:
CDC, Carl Washington, MD, Emory Univ. School of Medicine, Mona Saraiya, MD, MPH
pcds.org.uk/clinical-guidance/melanoma-an-overview1

Are Many Moles on Dark Skin Still a Melanoma Risk?
You may know that having many moles is a melanoma risk factor, but is this still a risk if you have a dark complexion?
Have you ever seen a person with a dark complexion and a large number of moles, and wondered if having so many moles placed that individual at a higher risk for melanoma?
After all, dark skin is less likely than a light complexion to develop this lethal skin cancer.
Each year, approximately 20,000 to 22,000 Americans die from melanoma, according to the American Cancer Society (2023).
Having many moles is a risk factor for melanoma.
“More moles is generally thought to be a risk factor, as is light skin, light hair, light eyes,” says Dr. Rebecca Baxt, a board certified dermatologist with Baxt CosMedical.
“Darker skinned people tend to get worse melanomas probably due to delay in diagnosis.
“It’s important to check hands and feet, especially in darker skinned individuals.”
There is actually no data that strictly applies to melanoma risk in people with many moles and fair skin, as compared to those with many moles and darker skin tones.
No research is out that gives conclusive information on comparative melanoma risk for dark skinned people who have a large number of moles.
Nevertheless, the comparison is certainly fascinating to speculate about.
Why is this malignancy “worse” in those with dark skin?
Dr. Baxt explains, “No one knows, but when African-Americans for example are diagnosed with melanoma, it tends to be at a later stage.
“We can infer that this might be due to lack of recognition since their skin is darker, or that doctors assume they have a low risk and don’t look for melanoma, or that they have less access to medical care; there is no good answer, just suppositions.
“But the fact is that the melanomas are often diagnosed later, so they have a poorer prognosis.”
In black people, melanoma often appears in less typical locations compared to lighter-skinned populations.
One of the most common areas for melanoma in black people is the palms of the hands and the soles of the feet.
This type of melanoma is known as acral lentiginous melanoma, which, while relatively rare overall, is more prevalent among people with darker skin.
Another area where melanoma can appear is under the nails, in a condition known as subungual melanoma.
This is characterized by dark streaks or spots beneath the nails and can be challenging to detect early due to its subtle presentation.
This stealthy cancer can also occur in mucous membranes, such as those in the mouth or genital area.
These sites are less frequently affected in people with light skin.
It’s simply not known, due to lack of research, if a dark skinned person with few moles is at less risk for melanoma than is a dark skinned person with many moles, even moles in very sun-exposed areas.
Why Is the Prognosis for Nail Melanoma Much Worse than Skin?
Dr. Baxt is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can a Lentigo Turn into Melanoma?

A lentigo can pass as a mole or birthmark; can it ever become a melanoma?
Whether or not a lentigo, which often looks just like a small mole or birth mark, could morph into melanoma, here is what Dr. Rebecca Baxt, a board certified dermatologist with Baxt CosMedical, explains:
“Usually no, but there is a variant of melanoma called lentigo maligna which is basically a lentigo gone bad that grows and becomes a melanoma.

A lentigo maligna. Omar Bari, Philip R. Cohen
“The good news is that these are rarely aggressive; they are usually melanoma ‘in-situ’ [confined to the site of its origin] in its earliest stage, and they grow slowly so there is lots of time to catch them before they become a problem.
“They are most common on the face of older people. If left to grow large, they can be very difficult to remove surgically.”
Dr. Baxt is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

White Sticky Stuff on Inner Walls of Mouth: Causes

There are several possible causes for the white, slimy and sticky substance that forms on the inner walls of your mouth.
Though experiencing a white, gooey substance on the inner walls of your mouth is a very unpleasant issue, be assured that the causes are not life-threatening.
“Dry mouth is the most common cause of this unpleasant sensation,” Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
If you find that your dry mouth seems unrelated to dehydration, place a small piece of lemon rind between your back teeth and inner wall of the mouth, and it will stimulate salivary gland production.
Other Causes of White Sticky Substance Inside Mouth
Dr. Goldenberg says, “Medical causes also exist, however. A yeast infection in the mouth can cause this sensation — this is especially common in patients with diabetes and those with very weak immune systems.
“An allergy to a food or your dental filling can also be the cause.”
In addition, certain toothpastes or brands can cause a white slimy substance to form inside of your mouth.
However, this would be an immediate result of using the toothpaste, and it will dissipate as the hours pass.
The solution is to find a toothpaste that doesn’t cause this problem.

Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/farland2456

Itchy Arms and Legs in Winter: Causes & Solutions

A dermatologist explains causes of itchy arms and legs during winter and what you can do about this.
“Winter itch is extremely common,” says Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
“It is caused by lack of skin moisture in cold, dry environments. It is particularly bad in patients who suffer from eczema and psoriasis.”
Eczema and psoriasis will cause visible changes to the skin, namely reddish or pink patches, bumps and scales.
Frequent aggressive scratching can cause the area to become crusty and leak fluid.
The itching can be so bad as to temp the sufferer to scratch with a hair brush — up and down the leg or arm. And it feels wonderful — as long as the scratching is in progress.
But soon after the scratching is stopped, the itching returns. There seemingly is no end to this winter itching.
Solutions to Wintertime Itchy Arms and Legs
“There are multiple things one can do to improve dry, flaky, itchy skin,” says Dr. Goldenberg.
“Applying moisturizer is extremely important. There are several products I recommend to my patients, including Cetaphil, Restoraderm, CeraVe lotion, and Kiehl’s Creme de Corps.
“Using a gentle cleanser instead of soap in the shower is also important. The shower should be quick and lukewarm, not hot. Using a humidifier in the bedroom while you are sleeping can also be very helpful. Interestingly, drinking more water does not seem to hydrate one’s skin.”
Beware also that wool clothing can make the arms itch, and wool socks can make the legs itch.
To keep warm in frigid outdoor winter air, instead of wearing wool you can try thermal “underwear.” This thin material, made of polypropylene, is highly effective at insulating the body from very cold temperatures.
And yet one more solution to wintertime itching of the arms and legs is to loosely wrap the most affected areas with Ace bandaging — as this harmless barrier will discourage scratching.
Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/namtipStudio

Is a Scab that Won’t Heal Always Cancer?

Can a non-healing scab be benign or is it always cancer?
You’ve probably heard for years that one of the classic signs of cancer is “a scab that won’t heal.” But is a non-healing scab always a sign of cancer?
“A non-healing lesion can be completely benign or could be malignant (cancerous),” says Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
“It really depends on the lesion in question.
“Sometimes something does not heal simply because more time is needed.
“This is especially true in the elderly and on the legs.”
But what if a lot of time has passed and the scab still has not healed?
Yes, cancer can be a cause, but there are a few more benign explanations for why a scab has not healed after a period of time. One of them is a low grade infection at the site that can be caused by bacteria or fungus.
Another benign cause is repeated trauma to the site that you may not even be aware of, such as a clothing strap or button chafing against the area.
If the non-healing scab is on your face, it’s possible that you’ve been unknowingly traumatizing the area over and over by habitually scratching there or rubbing the area as a stress habit.
If the non-healing lesion is on a leg, have you been unknowingly running a razor blade over the spot when shaving?
Cancer and a Scab that Won’t Heal
Dr. Goldenberg explains, “A more concerning scenario is when a non-healing lesion is a sign of underlying cancer.

A skin cancer that strongly resembles a common scab. Shutterstock/terry meador
“These lesions often ‘try’ to heal, only to scab and bleed again. A bleeding lesion is particularly concerning.
“The way to diagnose the lesion is to have a dermatologist perform a biopsy; this is a procedure in which the doctor will take a piece of skin and send it in for a pathology diagnosis.
“I always advise my patients to see me if they have a non-healing, bleeding lesion, to make sure it’s not cancerous.”

Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/thodonal88

Can Microdiscectomy Be Performed Under Regional Anesthesia?

If you need a microdiscectomy but are not suitable for general anesthesia, this procedure CAN be done using regional.
You may fear general or be a poor candidate for it, but this doesn’t mean you can’t undergo a microdiscectomy with regional anesthesia.
“Lumbar spinal surgery, especially a microdiscectomy, may be performed under regional anesthesia,” says spinal and orthopedic surgeon Kenneth K. Hansraj, MD, who specializes in minimally invasive spine surgery, laminectomies and spinal fusions, and is author of the book, “Keys to an Amazing Life: Secrets of the Cervical Spine.”
He continues, “Usually however, the anesthesiologists use a short-acting fentanyl to assist with analgesia.”
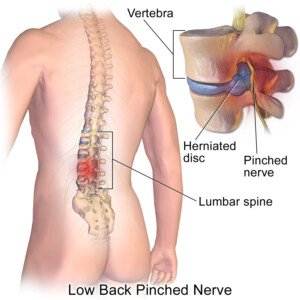
Herniated Disc Surgery
An Internet search may not bring up a lot of information on regional anesthesia being used for a microdiscectomy—a procedure that involves removing the portion of a lumbar disc that’s herniating (protruding out) from its natural space.
Thus, you may think that your only option is general.
“Lumbar microdiscectomy surgery is already performed under spinal anesthesia (SA) in many institutions,” states an abstract from a study (Dagher et al).
Another study (Papadopoulos et al) concludes: “Epidural anesthesia as an alternative to general anesthesia has shown less post-operative nausea and vomiting in lumbar microdiscectomy.”
Contraindications to herniated disc surgery under general include advanced age and severe heart disease.
More About Microdiscectomy
The procedure may be performed by either an orthopedic or a neurosurgeon.
A small portion of the bone over the disc material under the nerve root and/or nerve root is removed.
The surgery is been shown to be more effective as a general rule for relieving leg pain rather than low back pain.
In the case of leg pain, the relief is usually felt almost immediately after the procedure.
However, numbness or weakness symptoms may take weeks or even months to subside.
The microdiscectomy has been around for quite some time, and hence, many spine surgeons are very experienced with it, making this a reliable operation for nearly immediate – and sometimes outright immediate – relief of leg pain from nerve root compression.
Ask your physician about regional anesthesia, as there should be no reason why this can’t be done.
 Dr. Hansraj is an orthopedic surgeon in Poughkeepsie, NY, and is affiliated with St. Francis Hospital-Roslyn. He received his medical degree from Drexel University College of Medicine and has been in practice for 20+ years.
Dr. Hansraj is an orthopedic surgeon in Poughkeepsie, NY, and is affiliated with St. Francis Hospital-Roslyn. He received his medical degree from Drexel University College of Medicine and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/pressfoto
Sources:
ncbi.nlm.nih.gov/pubmed/15112850
deepdyve.com/lp/elsevier/lumbar-microdiscectomy-under-epidural-anesthesia-a-comparison-study-DBiuVBhDms

Best Medications for Sciatic Nerve Impingement
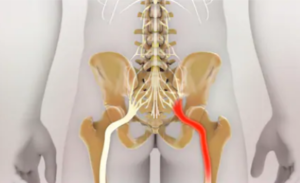
A spine doctor explains about medications for the pain of sciatic nerve pressure.
Sciatic nerve impingement can be caused by a herniated disc or a spasming piriformis muscle.
Either way, the pain has been described as “excruciating” by many patients.
It can come on suddenly, seemingly for no apparent reason, no known trigger.
Best medications for sciatic impingement pain?
“Medications in the classes of aspirin, non-steroidal anti-inflammatories, muscle relaxants, oral steroids, antidepressants and narcotics could be recommended to suppress the pain of symptomatic sciatic nerve,” says spinal and orthopedic surgeon Kenneth K. Hansraj, MD, who specializes in minimally invasive spine surgery, laminectomies and spinal fusions, and is author of the book, “Keys to an Amazing Life: Secrets of the Cervical Spine.”
He adds, “Each physician seems to have their own recipe for diminishing inflammation and calming the sciatic nerve.”
Why don’t prescription narcotics work (e.g., two Percocets)?
“Prescription narcotics may not work after a while when the patient develops a tolerance to the medication,” says Dr. Hansraj.
Oral steroid medications are often recommended as a pain reliever for people with sciatic pain, but at the same time, these can be taken only short-term.
“Long-term use of oral steroids may lead to increased blood sugar, osteoporosis, cataracts, muscular weakness and avascular necrosis (loss of blood supply leading to damage of the joints) of major joints including the hips and knees,” points out Dr. Hansraj.
But what if you absolutely cannot have surgery for your herniated disc?
For example, a person with a very bad heart may be a poor candidate for surgery simply because of the anesthesia.
“I have taken care of patients who have medical problems and comorbidities which will never allow them to have spinal surgery,” says Dr. Hansraj.
“Usually these patients are handled with continued conservative options.”
For sciatica these include heat and cold therapy, special chairs, physical therapy and of course, medications such as NSAIDs and antidepressants like Cymbalta.
Dr. Hansraj is an orthopedic surgeon in Poughkeepsie, NY, and is affiliated with St. Francis Hospital-Roslyn. He received his medical degree from Drexel University College of Medicine and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Nathan Devery

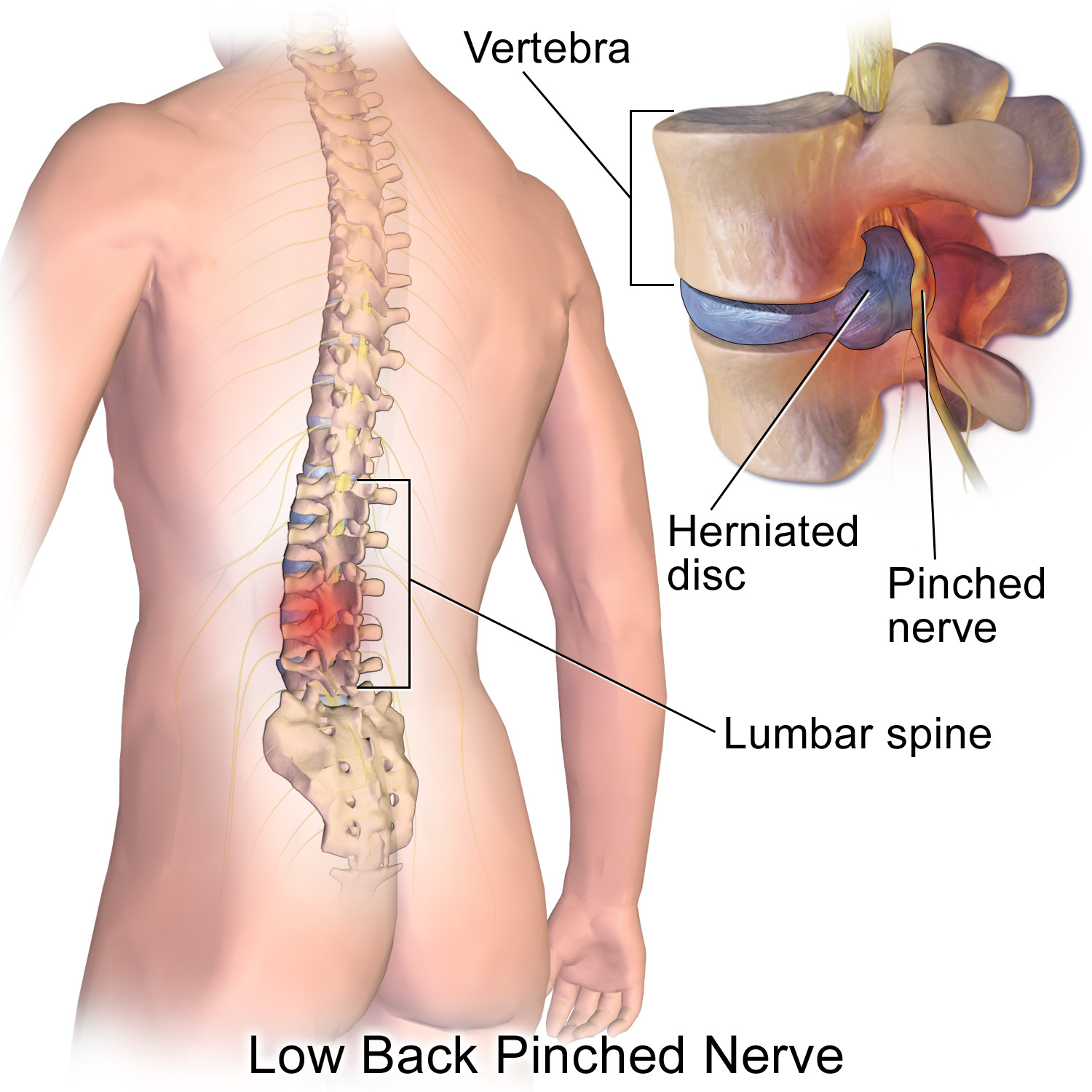
How Painful is Therapy for a Bulging Disc Supposed to Be?
How can a patient do physical therapy for a herniated disc if it hurts too much to exercise?
What if you have a herniated disc and find that the physical therapy exercises are impossible to do because you can’t get into the position without a lot of pain?
Some patients have this experience, yet surgery for the herniated disc is clearly out of the question — either because they are afraid of “going under the knife,” or because they have an unrelated medical condition that makes surgery risky.
Should you just grin and bear it? After all, a person who has never had an exercise regimen will find the pain of physical therapy more unbearable than will someone who is quite used to rigorous workout sessions or physical activity.
One thing that will invariably cross the patient’s mind is if the pain during physical therapy means that the movements are actually making the bulging disc worse.
Can physical therapy worsen a bulging disc?
“Physical therapy is employed to diminish pain and suffering,” says Kenneth K. Hansraj, MD, who specializes in minimally invasive spine surgery, laminectomies and spinal fusions, and is author of the book, “Keys to an Amazing Life: Secrets of the Cervical Spine.”
Dr. Hansraj continues, “Unfortunately, especially in the phases of pain, just touching the involved spinal area may lead to further pain and tenderness.
“I encourage my clients to stay with the therapy at this point, since the therapy will lead to diminished inflammation and restoration of function along with further tolerance of therapy.”
In other words, grin and bear it. Because if you do nothing for a disc herniation, it will likely never get better, and it certainly won’t magically go away.
Risk Factors for a Bulging or Herniated Disc
Several factors can increase the risk of developing a herniated disc.
Age is a primary risk factor, as the discs in the spine naturally degenerate and become more prone to herniation over time.
Physical activity also plays a role; individuals who engage in heavy lifting, repetitive bending, or strenuous activities are at higher risk, especially if they execute poor form.
Obesity adds extra pressure on the spine, increasing the likelihood of disc problems.
Poor posture and prolonged sitting can stress the spine and contribute to disc herniation.
Smoking is another risk factor, as it reduces blood flow to the spinal discs, impairing their health and resilience.
Additionally, genetics can contribute, as some people inherit a predisposition to disc issues.
Physical therapy is one of the best non-surgical treatments for the so-called bulging disc.
Do not give up on physical therapy, even if it causes some pain.
Dr. Hansraj is an orthopedic surgeon in Poughkeepsie, NY, and is affiliated with St. Francis Hospital-Roslyn. He received his medical degree from Drexel University College of Medicine and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus/CreativeCommons

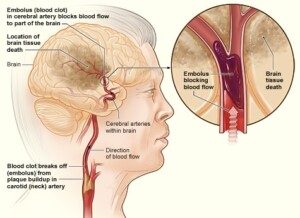
Risk of Stroke after TIA “Soft” Symptoms vs. “Hard”

The risk of stroke seems to differ depending on type of transient ischemic attack symptoms a person experiences.
A transient ischemic attack (TIA) is a mini stroke, when a clot forms in a blood vessel in the brain, temporarily cutting off blood (and thus oxygen) to the portion of the brain that the vessel feeds.
Which portion of the brain suffers this event determines the nature of the symptoms; the nature of the TIA.
TIA symptoms vary as much as brain function does, according to Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
TIA symptoms are classified as either “soft” or “hard.”
Typical warning information regarding a transient ischemic attack states that one-third of people, who experience this event, will suffer a stroke within 12 months.
This is a general figure that does not take into account type of symptom.
For instance, what percentage of people, whose TIA(s) consisted of only dizziness and double vision, will go on to have a stroke within 12 months?
And what percentage of people, who have a transient ischemic attack consisting of slurred speech or one-sided weakness or paralysis, eventually will have a stroke within 12 months?
When type of TIA symptom is considered, these percentages will change.
The average is 30 percent when all the symptoms — any TIA — are taken into account.
Dr. Mikolaenko explains, “From my experience I see plenty of elderly patients with many TIAs in the past and no stroke, not even old strokes on MRI imaging.
“I always ask myself: Are these people, with multiple admissions for ‘soft’ stroke symptoms, will they ever have a stroke if they live long enough, or [is it that] secondary prevention medication which they are on keeps them away from developing a full-blown stroke?”
Secondary medication consists of blood thinners, which may include a daily aspirin.
Dr. Mikolaenko says the following are soft symptoms of a transient ischemic attack:
- Hemiparesthesias [one-sided numbness/tingling]
- Dizziness/vertigo/lightheadedness
- Blurry vision
- Short lasting diplopia (double vision)
- Confusion
- Neck pain (cervicalgia)
- Unilateral limb pain/heaviness/discomfort
- Very short lasting memory loss.
NOTE: The pain, heaviness and discomfort here do not refer to weakness, which is a hard symptom.
Dr. Mikolaenko says, “‘Hard’ symptoms of TIAs are: aphasia (expressive or comprehensive, or mixed), hemiparesis ( one-sided weakness) or hemiplegia, monocular painless blindness.” Aphasia refers to speaking difficulties.
If all you’ve experienced are the soft symptoms of TIA, this doesn’t mean brush them aside and assume you’ll never have a stroke.
You are still at increased risk of a stroke; transient ischemic attacks mean that something is seriously wrong with the blood circulation that leads to, or that’s in, your brain.
National Heart Lung and Blood Insitute
Soft TIA symptoms that occur while you’re driving, operating machinery, walking down stairs, etc., can result in a fatal accident.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}