

12 Causes of Blood Clots and DVTs in Children

There are at least 12 causes of blood clots or deep vein thromboses in children. No age is immune.
Blood clots can occur anywhere in the body, but when they occur in larger vessels, they can become a serious problem.
When it comes to any kind of blood clot anywhere in the body of a child, the list of causes grows.
Not all blood clots are a deep vein thrombosis.
For example, a blood clot can occur in the brain due to head trauma.
There are causes of blood clots and deep vein thrombosis in the pediatric population.
“Genetic clotting disorders are very common,” begins Dr. Lisa Lewis, MD, a board certified pediatrician in Fort Worth, Texas, and author of “Feed the Baby Hummus, Pediatrician-Backed Secrets from Cultures Around the World.”
“Other causes include certain medications, surgery, anomalies of the blood vessels (for example a blood vessel that is not developed properly), immune system disorders, heart disease, immobility due to a medical condition or hospitalization, injuries, infection and cancer.”
Poor Blood Circulation
This can result from excessive inertia or constriction of a vein. Excessive inertia can easily be remedied by imposing limitations on how much time is spent watching TV and sitting around with a smartphone or computer game.
Turn the TV off and tell your child to go outside and play. HOWEVER, the directive of “go outside and play” is often not enough to encourage physical activity in a sedentary child.
But at least squatting down and making mud patties engages more muscles than does slumping on a couch staring at a screen.
Make sure your child has ready access to items that encourage movement: various balls, skates and other implements.
This can even include an air-filled striking bag for kids to have fun punching and kicking at.
A mini trampoline is also an option for older kids to offset inertia — and hence, reduce the risk of blood clots.
Damage to a Vein’s Inner Lining
Catheter placement into a vein can damage the inner lining of the vessel. Certain medications can also have this effect.
When children present with a DVT or pulmonary embolus, a combination of the above potential causes is often present.
Birth Control Pills
“Adolescents on birth control pills are more at risk of clotting disorders,” says Dr. Lewis.
“This is enhanced by smoking. Smoking is an independent risk factor for the formation of a deep vein thrombosis. So is obesity.
“At times a blood clot forms in a child for no apparent reason,” adds Dr. Lewis.
“A blood clot forms for various reasons depending on the cause. In general, a clot forms because of a cause that activates the components of clotting.
“For example, children with genetic clotting disorders may be missing a protein necessary for normal blood flow.”

Having 25+ years’ experience, Dr. Lewis completed her pediatrics residency at Texas A&M University Health Science Center, Scott and White Memorial Hospital. For two years afterward she was assistant professor in the department of pediatrics at Texas A&M University Health Science Center.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Who Should Have Upper Endoscopy to Diagnose Heartburn?

Too many upper endoscopies are being done unnecessarily, so if you have heartburn (GERD), take notice of this information.
If you’ve been diagnosed with heartburn secondary to GERD, but you have not had an upper endoscopy, have you ever wondered if you need this procedure?
A person may also find themselves tinkering with the idea of an upper endoscopy after learning that years of heartburn can lead to precancerous changes in the esophagus (Barrett’s esophagus).
“GERD or gastroesophageal reflux disease is a very common condition, with heartburn being the most common symptom of GERD — and seen in up to 50% people with GERD,” says Alan Gingold, DO, a board certified gastroenterologist with Central Jersey Ambulatory Surgical Center.
“Not everyone with heartburn needs to get an upper endoscopy,” continues Dr. Gingold.
“Typically an EGD is recommended for anyone who has heartburn that is longstanding (more than five years), symptoms not responding to medication, anyone aged 45 or over who has new symptoms or anyone with alarm symptoms: nausea/vomiting, dysphagia, anemia, blood on stool, weight loss.”
Dysphagia is difficulty swallowing.
Nevertheless, there may still be too many unnecessary endoscopies being done. In 2012, the Annals of Internal Medicine reported this.
Though that was years ago, it’s quite possible that people with heartburn are continuing to get unneeded upper endoscopies.
- After all, ads for heartburn relief continue to regularly air on TV and appear in print media.
- Furthermore, Barrett’s esophagus has received increased publicity.
However, if you seem to have heartburn or even if you were recently diagnosed with this condition, the next step is NOT to gun for the upper endoscopy.
Other Reasons for an Upper Endoscopy
If one’s heartburn doesn’t respond to medication after 4-8 weeks, this may call for an upper endoscopy.
Another reason for this exam is if the patient’s esophagus has a history of tightening or narrowing.
If the patient is over 50, male, has had diagnosed heartburn for at least five years, AND has other risk factors for Barrett’s esophagus – then he’s a candidate for an upper endoscopy.
Other Risk Factors for Barrett’s Esophagus
- Overnight reflux symptoms
- Excess body fat, especially in the belly
- Hiatal hernia
- Tobacco use
This patient may undergo an initial screening test for Barrett’s esophagus or esophageal cancer. If the result is negative, then periodic upper endoscopy is not needed.
What if you have Barrett’s esophagus?
Upper endoscopy should be done every three to five years.
If the patient has dysplasia, the upper endoscopy should be more frequent.
Overuse of upper endoscopy has not been found to improve the health or survival of patients suffering from heartburn.
 Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/airdone
Source: sciencedaily.com/releases/2012/12/121203183341.htm
What’s the Strongest Risk Factor for a Deep Vein Thrombosis?
You’ll be shocked at what the greatest risk factor is for a DVT (deep vein thrombosis).
If you’re thinking that obesity is the strongest risk factor for a DVT — you’re on the right track as far as the seriousness of this risk factor.
But there’s another one that trumps obesity, says a study.
And that biggest risk factor is the non-O ABO blood type, according to a study that’s published in the Canadian Medical Association Journal.
The report says that this blood type comprises up to 20 percent of risks for VTE (venous thromboembolism).
Data on over 66,000 people, who’d been tracked for 33 years, was analyzed.
But could the ABO blood type be linked to a higher risk of DVT in the general population?
The study authors determined that DVT risk grew when the ABO blood type was combined with the factor V Leiden R506Q or prothrombin G20210A, which are genetic mutations that increase venous thromboembolism risk.
The researchers add that ABO blood type was indeed the most important risk factor in the general population for DVT/PE.
Other Big Risk Factors for Deep Vein Thrombosis
Obesity. “There are probably multiple factors relating to obesity and DVT risk,” says Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.

Freepik.com
Dr. Besser explains, “It is theorized that significant obesity increases the hyper-coagulability of the blood (tendency to clot), especially if the person has a genetic predisposition to clotting (certain blood factors that are inherited can affect a person’s clotting ability).
“Additionally, physical factors, such as immobility (common in the obese) is another factor.”
Smoking. Quit. Just quit. Find another way to deal with stress or boredom.
Excessive sitting. Do you have a sit-down job? Every hour, get up and walk somewhere briskly, or do stationary lunges, squats or high knee marches for several minutes.
No exercise program. Start lifting weights and using cardio equipment, or join a cardio class. Go on hikes, bike rides, etc.
Though the greatest risk factor for a deep vein thrombosis is a blood type that you may not even have, this doesn’t mean that the other risk factors are insignificant. They count big-time.
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2013/02/130204130034.htm

Low Back Pain Cure with Simple Walking on a Treadmill

A consistent walking program using a treadmill can dramatically reduce or even eliminate low back pain. But if you use a treadmill, there’s a catch.
A report in Clinical Rehabilitation presents conclusions of a walking-study done with participants who had low back pain.
Frequency and Duration of Walking to Effectively Treat Low Back Pain
The program in this study, headed by Dr. Michal Katz-Leurer from Tel Aviv University’s Stanley Steyer School of Health Professions (Sackler Faculty of Medicine), consisted of walking two or three times a week for 20 to 40 minutes at a time.
This walking protocol turned out to be as effective for relieving low back pain as are the typical muscle strengthening exercises that require equipment and often supervision by rehab specialists.
How does walking cure or relieve low back pain?
Few people actually realize that the “core” is involved in walking. I’m a former certified personal trainer, and I’ve told my clients that the core—which is primarily the abdominals and low back—is engaged when one walks.
This is why when some very sedentary people suddenly do a lot of walking, their low back starts aching. These muscles have worked in a way they’re not used to.
Your body doesn’t have to bend in order to engage the core.
However, don’t let the possibility of backache stop you from a regular walking program if you suffer from low back pain.
You may feel some achiness at first, but it will subside sooner than you think as you stick with the program.
It’s like any new exercise to the body; the muscles are adjusting to the new stimulus, and in the process, develop benign aching or soreness. As the muscles get stronger or adapt, they will no longer get sore.
How the Study Was Done
Twenty-six people completed a muscle exercise program, and 26 others completed a walking program.
All participants had low back pain, and both programs lasted six weeks.
At the end of six weeks, both groups had great improvement in their condition.
How to Properly Use a Treadmill to Alleviate Back Pain
In order for walking to effectively treat low back pain, it must be done with correct biomechanics.
This means if you use a treadmill, DO NOT HOLD ON — other than for momentary steadying such as when drinking water.

Shutterstock/Khakimullin Aleksandr
Otherwise, when your hands are latched onto the sides or front, even lightly, this disrupts the natural gait pattern and can make low back pain worse, as well as cause new pains elsewhere in the body, such as in the hips, knees and feet.
If your back hurts more upon walking on a treadmill, this is because your lumbar muscles are being engaged. This achiness will especially occur if you use an incline without holding on.
This is because when you walk on a slope or incline, without holding on, your lower back muscles work to prevent you from falling backwards!
If you hold on, this will relieve the soreness or aching, but holding onto the treadmill is WRONG!
Keep walking without holding on, and that aching in your low back will vanish. Give those weak, out of shape muscles a chance to get strong and reliable!
Use a SLOW pace and medium to low incline. There is no need to crank the machine up to 15 percent and run the tread at 4 mph, which is too difficult to sustain a walk without holding on.
But holding onto a treadmill at ANY setting will cheat your low back from the work it needs to help prevent or eliminate pains and aches.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com/shayne_ch13
Source: sciencedaily.com/releases/2013/03/130305131404.htm

How Long Can “Stool Beeturia” Last?

Here is what a GI doctor says about how long beet juice in one’s stools can last.
Beet juice in the stools, to some, is “cool,” but to others, is very frightening, as this can masquerade as blood in the stools.
In medicine, “beeturia” refers to the unabsorbed crimson pigment of this vegetable, called betanin, in a person’s urine, not their bowel movements.
If you’re seeing red in your stools three or four days after eating whole beets or beet juice, it might be tempting to start thinking that this is blood.
The betanin comes out in the urine, which comes out with your poops, creating the illusion that your BMs themselves are reddish.
What’s actually happening is that your stools are surrounded by the urine that has the beet pigment in it.
Of course it’s going to get on your bowel movements.
But can this “stool beeturia” still occur five days after you ate the beets or drank beet juice?
Yes — because I myself have had it five days out.
I might also add that I had the beeturia five days in a row, rather than skipping the first four days and then seeing it on day 5.
“In the stool it’s also generally two days, but maybe three or four,” says Jonathan Zinberg, MD, chief of gastroenterology at South Nassau Communities Hospital, Oceanside, NY.
“It is more likely to occur in those who have increased iron absorption, such as those with iron deficiency.
“But remember, not all biologic specimens (i.e., people) follow the rules, so there can be variability.”
For a more in-depth — and reassuring look at this phenomen, read my other article:
Red Stools from Beets vs. from Blood: How to Tell the Difference
 Jonathan Zinberg, MD
Jonathan Zinberg, MD
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Volosina

Sharp Sudden Pain in Upper Arm: Non-Cardiac Cause

Find out what can likely cause a sudden sharp pain in the upper arm that’s not related to your heart.
If you’ve been experiencing episodes of a sudden and sharp pain located in your upper arm, this may very possibly be a condition called long head biceps tendonopathy.
This is when the tendon of the long head of the biceps is torn; it may or may not cause pain.
If you have LHB tendonopathy, you may also have a shoulder problem, namely, a rotator cuff tear.
A torn rotator cuff, as well, can cause a sudden sharp pain in the upper arm.
However, these aren’t the only musculoskeletal causes of a sudden sharp pain in the upper arm; hence, a thorough examination, which includes radiographic imaging, will be necessary for precise diagnosis.
The treatment for long head biceps tendonopathy may be surgical or nonsurgical, says Shane Nho, MD, a Chicago-based orthopedic surgeon.
His report appears in the Nov. 2010 Journal of the American Academy of Orthopaedic Surgeons.
Statistics & Trends
-There’s no big difference in patient satisfaction or function between the two main surgical options, which are biceps tenotomy and tenodesis.
-The complication rate from surgery is less than 1 percent.
-Both surgeries can be performed via arthroscopy.
-The JAAOS report urges the pursuit of nonsurgical treatment at first, as this may suffice for ending the upper arm sudden pain and other related issues.
-Younger, active patients should undergo the biceps tenodesis if surgery is warranted.
Conservative Treatment for Long Head Biceps Tendonopathy
Rest, avoiding and/or modifying the offending activity, taking anti-inflammatory drugs, and physical therapy.

Shutterstock/Photographee.eu
If these don’t work, then corticosteroid injections may be done, though these may put a patient at risk for tendon rupture, depending on site of injection.
Besides sudden sharp upper arm pain, long head biceps tendonopathy can also cause the following symptoms:
-Audible snapping or popping in the elbow or shoulder
-Biceps cramping resulting from strenuous use
-Bruising from the middle of upper arm down towards elbow
-Tenderness, pain and/or weakness at elbow or shoulder
-Difficulty turning palm up or down
-Funny bulge above the elbow (from flaccid muscle)
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2010/11/101104101653.htm

How Effective is Weight Loss for Arthritic Knee Pain?

Obesity is one of the leading risk factors for osteoarthritis knee pain; it stands to reason that weight loss will improve the condition.
If you have knee pain, particularly osteoarthritis, and are overweight, then weight loss will probably result in a notable reduction in pain — even though osteoarthritis of the knee can affect medium-built or thin individuals.
Just because thinner people suffer from osteoarthritis of the knee doesn’t mean that obesity isn’t a major risk factor.
The knee is not the most stable joint in the body. Most of one’s body weight is above this joint.
Losing weight will have its virtues for those with painful knees.
Don’t let deluded body-positive people on Instagram trick you into thinking that excess body fat cannot cause issues with quality of life.
- Thin people with knee problems are never told to gain weight for symptom relief.
- Plus size patients are routinely told to drop pounds for symptom relief.
Weight Loss Reduces Knee Pain: Study
Research at the Penn State College of Medicine shows that obese patients who had early-onset osteoarthritis of their knees experienced major improvement in symptoms after an average weight loss of 57 pounds.
Exercising with Knee Pain to Lose Weight
When I was a personal trainer I had overweight clients with knee pain. Losing weight is a must for these men and women.
Aerobic activity can assist with weight loss, but painful arthritic knees will interfere with how rigorous the exercise is.
However, upper body strength training can be done very intensely by overweight people with arthritic knees.
- Lying down bench press and dumbbell press
- Seated chest press with a machine
- Seated overhead dumbbell press or shoulder press with a machine
- Seated cable row
- Seated lat pull-down

Overhead Dumbbell Press

Seated Chest Press

Lying Triceps Extension
As for aerobics, some patients will get a clearance from their doctor for pedaling on a stationary bike or elliptical trainer, plus walking inclines on a treadmill, as long as the arthritis doesn’t cause any pain.
A combination of these aerobics plus weight workouts will facilitate fat loss, which will lead to an improvement in the symptoms of knee arthritis.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Hannamariah
Source: sciencedaily.com/releases/2011/02/110219160015.htm

Rotator Cuff Tear Diagnosis: MR Arthrography vs. Regular MRI
Find out which procedure, the MR arthrography or a standard MRI, is better at detecting a rotator cuff tear.
Diagnosing a rotator cuff tear or other type of tissue tear isn’t always as simple as a patient may think, even if the resulting shoulder pain is classical of this condition.
A study that was done at the Neuroskeletal Imaging in Merritt Island, Florida showed that magnetic resonance (MR) arthrography of the shoulder better identifies a rotator cuff tear, when compared to a regular MRI.
However, not all doctors will inform the patient that the MR arthrography is an option.
When a doctor wanted to figure out what was going on with my mother’s painful shoulder, the only imaging study that was mentioned was the regular MRI.
So if you have a painful shoulder or suspect a torn rotator cuff or some other tear (e.g., labral), be sure to inquire about the MR arthrography, which requires that a contrast dye be injected into the joint.
Says Thomas Magee, MD, the study’s lead author, in the report: “With MR arthrography we were able to see things with a high degree of accuracy in the shoulder.”
Dr. Magee explains that with a non-contrast procedure (3T MRI), the “resolution and picture quality” is high, “except for lesions that are hidden without distension (swelling) of the joint,” he says.
“During MR arthrography, distention of the joint allowed us to uncover lesions that could not be seen on conventional MRI.”
The MR arthrogram provides a “better road map for surgeons,” says Dr. Magee.
If you’ve had only an MRI, and your doctor recommends surgery, WAIT — first insist upon the MR arthrogram for a more accurate assessment.
It may determine you don’t even need surgery.
The report appears in the 2009 American Journal of Roentgenology.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Andrey_Popov
Source: sciencedaily.com/releases/2009/01/090106154410.htm

Torn Rotator Cuff Pain: Reverse Total Shoulder Replacement

If you have constant pain from a torn rotator cuff, the reverse total shoulder replacement may be a realistic option.
If you have a completely torn rotator cuff and suffer with constant shoulder pain, no amount of physical therapy or cortisone shots will subdue the pain to the extent where you can live a normal life—especially if you also have arthritis in this joint.
The rotator cuff refers to a group of four muscles and their tendons.
They are frequently the subject of some degree of injury, ranging from strain and overuse, to inflammation and impingement syndrome, to a partial or a complete tear.
However, other things can go wrong for which replacement of the shoulder joint is a viable option.
What is the reverse total shoulder replacement and whom is it for?
The shoulder joint is a “ball-and-saucer” structure. In osteoarthritis, there is bone on bone contact, which causes a lot of pain and is “usually associated with joint stiffness,” says Omer llhai, MD, orthopedic surgeon at The Methodist Hospital in Houston.
In osteoarthritis, there is a wearing down of the cartilage between the bones.
The job of this cartilage is to cushion the bones and to provide shock absorption.
When this cartilage deteriorates, the bones begin to rub against each other, leading to pain, stiffness and reduced joint mobility.
The loss of cartilage not only disrupts the joint’s smooth movement but also contributes to the formation of bone spurs and inflammation, exacerbating the discomfort and functional limitations associated with osteoarthritis.
The reverse total shoulder procedure is not designed to remedy a tear in a rotator cuff tendon.
Rather, this surgery is for the replacement of the warn-down saucer part of the joint with a metal ball.
And the worn-out ball part of the arthritic joint gets replaced with a device — this device contains a big plastic cup.
When the saucer is replaced with a metal ball, and the natural “ball” is replaced with the cup, this renders the shoulder joint no longer requiring an intact rotator cuff for motion or stability.
Hence, the patient’s shoulder joint, with proper post-op rehab and physical therapy, should then function normally.
Prevention of a Torn Rotator Cuff
One of the most effective ways to prevent a rotator cuff injury is through strengthening exercises that target the shoulder muscles — in combination with GOOD FORM.
Exercises that enhance the strength and flexibility of the rotator cuff and surrounding muscles can provide better support and stability to the shoulder joint.
Incorporating activities such as resistance training, stretching and range-of-motion exercises into your routine will help maintain shoulder health and prevent injury.
Proper technique and body mechanics during physical activities are crucial for preventing rotator cuff tears.
This includes using correct posture and alignment while lifting weights, participating in sports or performing repetitive tasks.
Reducing the odds of injury can also be achieved if you devote time to warming up your shoulder joints prior to any intense lifting of weights.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Leszek Glasner
Source: sciencedaily.com/releases/2009/03/090325190508.htm

Is Shoulder Surgery Safe for Elderly with Rotator Cuff Pain?

Find out what kind of shoulder surgery is safer for elderly patients suffering with debilitating rotator cuff pain.
An elderly person may be concerned about complications from shoulder surgery.
However, a Rush University Medical Center study shows that for the elderly, arthroscopic surgery is a safe bet, and it works to reduce pain and improve function. Arthroscopy is minimally invasive.
The paper states that for people over the age of 70 who want pain relief, this relief is a fairly predictable outcome of the surgery.
For those of advanced age, pain relief tends to be a higher priority over that of 100 percent restoration of shoulder function.
An example of function is that of being able to retrieve an item from a high shelf, requiring maximum overhead reach of the arms and hands.
Arthroscopy may not restore all the function in some patients, such as those with a large tear in their rotator cuff, but it will go a long way in relieving the pain.
In short, people over age 70 are not too old for shoulder arthroscopic surgery for the treatment of rotator cuff pain.
Tear in the Rotator Cuff
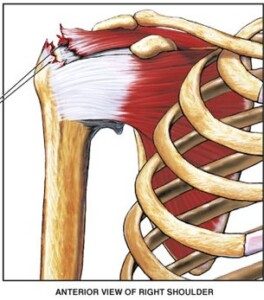
A tear in a rotator cuff tendon. Nucleus Communications, via Wikimedia Commons
“According to a systematic review in 2020, which looked at rotator cuff repair in patients over the age of 70 years, there was a high satisfaction rate with significant improvement in function and pain in this patient population,” says Marc F. Matarazzo, MD, a board certified orthopedic surgeon with Total MD Family Medicine & Urgent Care.
Tears in the rotator cuff occur to about 20 percent of people over age 65.
A surgeon might advise against an operation for elderly patients due to less resilient bone quality and circulation.
But for older people for whom conservative treatments were not effective, arthroscopy is their last hope.
Studies have followed rotator cuff repair patients long-term and found that not only was their pain greatly reduced, but in many cases, their range of motion had improved significantly.
This means being able to raise the surgical arm in front as well as rotate it to the side — motions that were impossible or difficult prior to the procedure.
Another area that the procedure can improve in the elderly is that of strength.
Ninety-four percent of the patients for the Rush University study said they’d have the surgery again if they had to do it over.
Why does arthroscopic shoulder surgery turn out so well for elderly patients?
There are newer surgical techniques, plus the patients’ commitment to post-operative rehab.
However, there will always be patients of elderly age whose rotator cuff tears are determined to be non-repairable, and hence, are not candidates for arthroscopic surgery.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}