
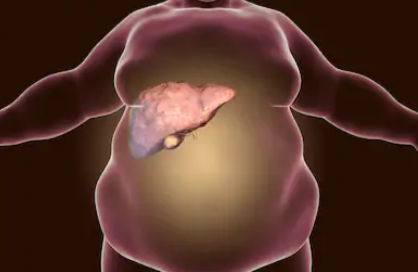
Can Non-Alcoholic Fatty Liver Disease Cause Bad Body Odor?
Can a bad body stink be caused by non-alcoholic fatty liver disease (NAFLD)?
Ever wonder if non-alcoholic fatty liver disease cause foul body odor? If so, how?
“Yes. If the patient is in liver failure, they’ll develop the odor regardless of whether or not alcohol is involved,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“However, alcohol is the most common cause of liver disease in this country.
“Obesity and high triglycerides are also common causes.”
Non-alcoholic fatty liver disease can cause foul body odor as follows:
A damaged liver doesn’t detoxify chemicals as efficiently as it should.
Compounds like ammonia, sulfur byproducts and ketones can build up in the blood and get released through breath, sweat and urine.
This can create a musty, sour or “rotten” odor that can be detected by someone near that person.
It even has a name: fetor hepaticus.
Hormonal changes, insulin resistance and altered gut bacteria in NAFLD can make this odor even stronger.

Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Kateryna Kon

Benign Causes of Elevated ALT and AST

Find out if an elevated ALT or AST can ever have a benign cause.
Just what does “elevated” mean in reference to the liver enzymes of ALT and AST?
The elevation can be mild, moderate or significant.
You may be wondering if the cause of a very mild elevation could ever be benign.
Benign Causes of Elevated ALT
“The only benign reason would be if that patient’s normal range is beyond the average, but that is very rare,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“For the most part, there are no benign elevations of ALT — there’s always a reason. Some medications can affect ALT levels, so can alcohol consumption and over-working your muscles.”
If you’re scheduled for a blood test for liver enzymes, do not lift weights for two to four days prior to the test, if you want to ensure that muscle fiber damage won’t influence the results.
However, a report in the British Journal of Clinical Pharmacology notes that in a study, the ALT and AST remained elevated seven days out from an intense weightlifting session in healthy men who were not weightlifters.
Benign Causes of Elevated AST
If the person’s normal range for AST is above average, says Dr. Fine, this can explain an “elevation,” but that’s rare.
“For the most part, AST elevations aren’t benign. There’s usually an underlying pathology like muscle inflammation or alcohol consumption.”
And keep in mind the study in the BJCP noted above.
“If your AST or ALT levels are elevated, see a qualified physician as soon as possible.”
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Monkey Business Images
Source: ncbi.nlm.nih.gov/pmc/articles/PMC2291230/

Do AST and ALT Values Show Liver Cancer? What About Hep?

The value of the ALT and AST liver enzymes will vary depending on the type of liver sickness including cancer.
In general (numbers vary from one lab to the next), a blood test value of over 50 for the ALT is considered elevated, not within the normal range. For AST, the cut-off point is 40 (anything above is elevated).
Again, realize that these cut-off points will vary with different testing labs.
What are the AST and ALT values that are associated with fatty liver disease, the common hepatitis viruses, liver cancer and other liver disease?
“AST and ALT levels vary greatly depending on the liver disease and the individual patient,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“In fatty liver disease for example, the AST and ALT values are usually twice the normal range or higher.
“They can be as high as 10 times normal. They can also be up to 10 times the normal range in common hepatitis cases like in hepatitis A, B and C.”
What about cancer?
“With liver cancer, the AST and ALT levels could be mild to normal because those cells are burnt out, so there is no AST or ALT leak,” says Dr. Fine.
Autoimmune Disease
“In autoimmune liver disease, which is more common among women, the AST and ALT levels can be three to six times normal.”
How to protect yourself against liver disease
– Avoid drinking alcohol, or drink only occasionally at the most.
– Exercise regularly, and this includes strength training.
– Avoid processed foods as much as possible.
– Avoid unhealthy ingredients like trans fats and preservatives.
– Lose weight if you’re overweight. If you’re not overweight, don’t gain excess weight.
– Limit foods with added sugars. This includes the so-called nutrition or meal bars.
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Chinnapong
Can “Bad” Cholesterol Be Raised by Non-Fatty Liver Disease?
Non-alcoholic fatty liver disease means something is very wrong with your body.
Can this condition, which is often brought on by poor diet, actually raise your LDL (bad) cholesterol?
“Yes. LDL receptors are located primarily in the liver and their number is regulated by the cholesterol content in the liver cells,” explains Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“When a person’s diet is high in saturated fat and cholesterol, the cholesterol content generally rises. This causes the LDL receptors to fall and plasma LDL levels to rise.”
It’s important to note that the biggest perpetrator in raising cholesterol levels in the body is refined carbohydrates.
The influx of added sugars and white-flour-based foods really does a number on body chemistry and health.
- Avoid white flour as much as possible.
- Limit saturated fats, and avoid trans fats (partially hydrogenated oils).
Non-alcoholic fatty liver disease is often caused by poor diet. High LDL cholesterol is a risk factor for heart attack.
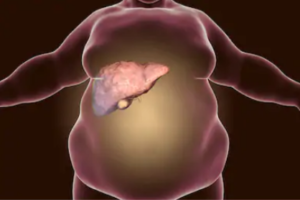
Symptoms of Non-Alcoholic Fatty Liver Disease
Also known as NAFLD, this condition encompasses numerous liver diseases that affect those who drink only a little or no liquor at all.
Too much fat gets stored in the liver cells and can lead to non-alcoholic steatohepatitis, which can permanently damage the liver.
In fact, the damage is similar to what can occur with a heavy drinker, and can lead to failure of this organ.
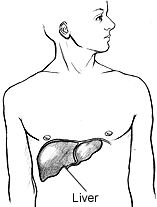
Usually there are no symptoms, but they may be fatigue and pain in the upper right abdomen.
But the steatohepatitis can cause fluid retention in the stomach, causing it to swell.
Other symptoms of non-alcoholic steatohepatitis: visibly enlarged blood vessels under the skin’s surface, red palms, enlarged breasts in men, and jaundice (yellowing of the skin and eyes).
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Kateryna Kon
Liver Disease Answers: Body Odor, Urine Color, ALT, AST
Below are links to articles about liver disease that answer questions that perhaps you’ve been struggling to find answers for with extensive online searches–which either turned up nothing or vague, overly-broad information.
So I asked a medical doctor to give me the straight answers and wrote the following articles — which include his statements.
Body Odor
Perhaps you’ve heard or read somewhere that liver disease can cause a distinct body odor.
No, not the typical “BO” that one might detect on someone who just had a gym workout, who wears dirty clothes or who doesn’t shower often enough.

Shutterstock/ESB Professional
Can body odor be a single symptom of liver pathology?
How many people with liver problems have bad body odor
Labs
What about those blood tests for liver function?
Ever wonder about those and how telling they might be?

Shutterstock/Olena Yakobchuk
ALT and AST: Looking at the Values
Urine Output
Liver disease can change urine color due to a buildup of bilirubin, a yellow pigment produced during the breakdown of red blood cells.
When the liver is damaged, it cannot process bilirubin properly, causing it to spill into the bloodstream and be excreted in the urine.
This often results in dark brown, amber or tea-colored urine.

James Heilman, MD/CreativeCommons
How common is liver disease?
As of 2025, liver disease remains a serious and growing health concern in America.
An estimated five million adults — about 2% of the U.S. population — have some form of liver disease.
Nonalcoholic fatty liver disease (NAFLD) continues to rise, driven by increasing rates of obesity, diabetes and metabolic syndrome.
In fact, type 2 diabetes and metabolic syndrome are strongly associated with obesity.
Other common forms include alcoholic liver disease, hepatitis B and C, and cirrhosis.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why Your Shins Hurt when Walking & How to Prevent Pain

Do you dread walking anywhere thanks to a mysterious pain that’s developed in your shins?
There are multiple possible explanations for a recurring pain in your shins whenever you go walking.
“Shin pain when walking can be due to exertional compartment syndrome, shin splints, tendonitis or stress fractures,” says Reggie Alexander, MD, an orthopedic surgeon with Orthopaedic Specialists in Los Angeles, CA.
Dr. Alexander explains, “It’s important to obtain a good history as to when and what events trigger the pain.
“In addition if appropriate, a dietary history may be important in making a diagnosis.”
Shin Pain from Exertional Compartment Syndrome
The pain from this usually does occur in the lower leg, and though it’s usually induced by exercise, particularly running, it can occur to those whose only activity is walking.
There may also be tingling, numbness or weakness.
Pain from Shin Splints
Athletes and runners are more affected by this than are less active people, but again, walkers can get this condition of inflammation of the connective tissue along the shin bone.
Tendonitis
Tendons attach muscle to bone. An inflamed tendon, depending on the area of compromise, will make the lower leg hurt when walking.
Stress Fracture
A stress fracture is just that: a fracture from stress. The fracture is a tiny crack in a bone that’s too small to displace the bone.
What should be done?
“Possible solutions include proper stretching and warmup, orthotics to correct alignment, activity modification and/or a short course of anti-inflammatory agents,” says Dr. Alexander.
Orthotics are custom-made shoe inserts that help realign the foot.
Improper foot alignment can cause pain that travels up the leg.
Each specific possible cause for shin pain will have a unique course of treatment.
But regardless of cause, the common treatment among all will be that of reducing your walking time and/or intensity.
You may even need to back off entirely from non-essential walking until the injury heals.
 Dr. Alexander’s sports experience covers many teams including those at the University of Chicago and at UCLA. Surgical and pain areas of expertise include the rotator cuff, ACL reconstruction, neck, back, hip and foot.
Dr. Alexander’s sports experience covers many teams including those at the University of Chicago and at UCLA. Surgical and pain areas of expertise include the rotator cuff, ACL reconstruction, neck, back, hip and foot.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/ BEAUTY STUDIO

Why Running Might Cause Sharp Pain in the Knee

If running causes a sharp pain in one or both of your knees, don’t ignore this or try to “run it out.”
It is not normal and can have a variety of causes.
The human body was designed to run, and that’s how our ancient ancestors survived in the wilderness.
But today’s running is a lot harder on the joints and a lot more excessive in duration than what’s required for survival by a hunter-gatherer society of ancient or present-day times.
Knee Pain After Running
“Pain after running can be attributed to a wide variety of causes: meniscal pathology, ligamentous injury, exercise induced compartment syndrome or exertional compartment syndrome, cartilage degeneration or tendonitis,” explains Reggie Alexander, MD, an orthopedic surgeon with Orthopaedic Specialists in Los Angeles, CA.
- Meniscus: cartilage in the knee joint
- Ligament: band of tissue that attaches bone to bone
- Compartment syndrome: pressure buildup involving the muscles, resulting in reduced blood flow. Can radiate pain to the knee.
- Tendon: band of tissue that attaches muscle to bone. Can become inflamed.
“Also, it’s not uncommon for runners to have iliotibial band syndrome or tight hamstrings,” continues Dr. Alexander.
The repetitive bending of the knee during running can lead to iliotibial band syndrome.
The IT band, a group of fibers, runs the length of one’s upper leg, from hip to the top of the shin.
Overuse can cause the IT band to tighten up. A tightened band can then rub against the outside of one’s knee — causing pain that’s hard to ignore and should never be ignored.
As for tight hamstrings, these are frequently a culprit in knee as well as low back pain.
“It’s important for runners to note when the symptoms occurred (immediately, in the middle, or at the end of your run), associated symptoms that you may have with that knee pain (such as numbness or tingling), and how long it takes for your symptoms to resolve.”
Dr. Alexander’s sports experience covers many teams including those at the University of Chicago and at UCLA. Surgical and pain areas of expertise include the rotator cuff, ACL reconstruction, neck, back, hip and foot.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Pain where Butt Meets Back of Thigh: Causes

Do you have a pain where your rear-end meets the back of your upper thigh?
This area is also known as the glute-hamstring tie-in or junction.
What could be causing pain there?
“Pain in the buttocks can be attributed to a wide variety of issues, such as nerve entrapment, bursitis, spinal pathology, tendonitis, and partial or complete hamstring injuries,” says Reggie Alexander, MD, an orthopedic surgeon with Orthopaedic Specialists in Los Angeles, CA.
“Taking a good history and teasing out whether or not there are neurologic symptoms can help distinguish between an entrapped nerve versus muscle or tendon pathology.”
A mechanical cause of discomfort or pain where the butt muscles merge with the upper hamstrings is that of repeatedly decelerating very quickly from a hard run, as you might do when doing fast running intervals on a treadmill or in a parking lot.

You should never stop abruptly! Always gradually decelerate, taking at least 12 seconds. How do I know?
It happened to me: pain in the gluteus maximus hamstring junction from abrupt cessation of treadmill sprints.
I switched to a gradual slow-down of the speed once I completed each fast interval, and within a few weeks the discomfort where my buttocks meets the back of my thigh was nearly gone.
Competitive sprinters avoid stopping abruptly after a false start by gradually decelerating. You’ll see this at every Olympics.
They understand that a sudden stop from high-speed running can lead to muscle injuries.
Instead, they allow their body to slow down naturally, which helps to prevent strain and damage to their muscles.
This controlled deceleration minimizes the risk of injury and ensures they remain in good condition for their next attempt.
“Resting after the initial injury can be helpful,” says Dr. Alexander, regarding injuries in general to the area where the buttucks meets the thighs.
“Other possible solutions include anti-inflammatory agents, stretching and physical therapy once the initial pain subsides.”
Dr. Alexander’s sports experience covers many teams including those at the University of Chicago and at UCLA. Surgical and pain areas of expertise include the rotator cuff, ACL reconstruction, neck, back, hip and foot.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Cause of Neck Pain that Runs into the Left Shoulder

Though pain in the neck that makes its way down to the left shoulder usually has a benign orthopedic cause, lung cancer can also cause this symptom.
“Pain in the neck and shoulder region can be hard to discern,” says Reggie Alexander, MD, an orthopedic surgeon with Orthopaedic Specialists in Los Angeles, CA.
Dr. Alexander continues, “Patients should note if the pain starts in the neck or shoulder. Radicular symptoms (pain that starts in the neck and shoots down the arm) can be helpful in figuring out if the pain is coming from the neck or shoulder. Neck pain tends to radiate past the elbow into the fingers.
“Pain in the neck can be due to arthritis, a herniated disc, or muscle spasms — to name a few.
“Shoulder pain also has a variety of causes, such as rotator cuff tears or inflammation, impingement, acromiocalvicular arthritis or shoulder separation, or labral pathology.”
In rare cases, pain in the shoulder that does not respond to orthopedic treatments or physical therapy may actually be caused by lung cancer.
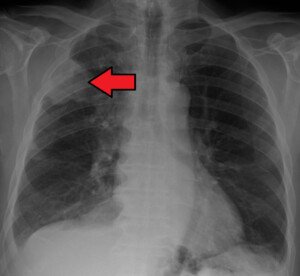
James Heilman, MD, CreativeCommons
The tumor is at the top portion of the lung and is making contact with a nerve that leads into the shoulder.
This type of cancer, called a Pancoast tumor, may cause pain that radiates to the shoulder, upper back or arm, often without typical lung symptoms like coughing.
A doctor may order imaging tests like a chest X-ray, CT scan or MRI to look for tumors near the lung apex.
Dr. Alexander’s sports experience covers many teams including those at the University of Chicago and at UCLA. Surgical and pain areas of expertise include the rotator cuff, ACL reconstruction, neck, back, hip and foot.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Comparing the Symptoms of Knee Bursitis with Chondromalacia

Chondromalacia patella and bursitis are common conditions that involve the kneecap, causing distinct pain.
But does one have any unique characteristic that the other one doesn’t?
“Bursitis usually involves inflammation of the prepatellar bursa,” says Reggie Alexander, MD, an orthopedic surgeon with Orthopaedic Specialists in Los Angeles, CA.
“It can be exacerbated by kneeling. It may be associated with local tenderness. Patellofemoral syndrome involves anterior [front] knee pain that can be exacerbated by kneeling, stairs or squatting.
“There may be crepitus (popping or crackling) in the patellofemoral joint when the knee is taken through range of motion.”
This range of motion can include simply extending and flexing the knee (straightening and bending) from a standing or seated position.
Any way for the layman to know what their knee condition is more likely to be?
“The presence or absence of swelling is helpful for determining this,” says Dr. Alexander. “If swelling is present, it’s more likely to be knee bursitis as opposed to patellofemoral syndrome.
“Also, people should keep track of what activities exacerbate their symptoms. If kneeling is the only activity that exacerbates your symptoms, it’s more likely to be knee bursitis.”
If there’s no pain or discomfort when going up stairs, this does not rule out patellofemoral syndrome (which many laypeople also refer to as chondromalacia).
However, the feature symptom of this condition is that of increasing pain as one deepens into a squat or crouching position.
Any home tests they can give themselves to provide a clue to which condition they have?
Dr. Alexander says, “Note whether or not pain occurs with range of motion or if it’s isolated to one spot.
“If it’s isolated to one spot, then it is more likely to be knee bursitis. Also, if you’re experiencing swelling, it’s more likely to be knee bursitis.”
Dr. Alexander’s sports experience covers many teams including those at the University of Chicago and at UCLA. Surgical and pain areas of expertise include the rotator cuff, ACL reconstruction, neck, back, hip and foot.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}