
Is It Safe to Let Go when Walking a Steep Treadmill Incline?

Step-by-step instructions in how to use a steep treadmill incline without holding on to get the most calorie burn and fitness benefits.
Every time I see a person using a high percent incline on a treadmill, he or she is grasping the bar in front or are gripping behind the display console.
This big mistake cancels out the effect of that huge incline.
When using a 30 percent incline and hanging onto the treadmill, the user will report that it’s impossible to walk this level of steepness without “falling off.”
If you’ve been using a steep incline and feel you must hold onto the treadmill, here is my question:
- What is the slowest speed you’ve ever used at this grade?
- My next question is: How slow can the machine be set at?
Think good and hard about your answers. If you stood on the incline but the belt was not moving (the treadmill wasn’t on), would you fall off? No. You’d be standing vertically and stable.
Now, march in place while on the high incline while the belt is still turned off. Do you fall? No.
Now, turn the machine on and set the speed at half a mile per hour and move your feet to keep up with the belt, but do not put your hands on the treadmill.
Keep them at your side, as they were when you were marching or as they’d be if you were walking this pace up a hill outside.
Do you fall? I’m betting you’ll come nowhere near falling off. That’s because your body is vertical and your legs are able to keep up with the very slow moving belt, even though it’s at a high incline.
Now gradually increase the speed, but do not advance it over that threshold to where your legs would not be able to keep up. For most trainees, that will be somewhere around 1.5 mph.
You won’t necessarily get out of breath at 1.5 mph, but unless your lower extremities are trained to move at considerable steepness, the back of your lower legs will fatigue quite quickly and you’ll be forced to take a rest.
What’s the best way to take a rest?
By lowering the incline. You can also increase the speed at this point. The lower incline will relieve your aching calves and Achilles regions.
When you reach the point of too much fatigue at a steep grade, do NOT hold onto the treadmill for the relief!
This “un-duplicates” a natural gait and trains your body to become dependent on an external support.
Instead, reduce the incline, even if this means waiting 30 seconds for the machine to sink down to 10 percent or even zero.
Be patient and wait, as you continue walking with a natural arm swing.
To get used to a 30 or higher percent incline, you’ll need to work it interval style:
Walk at 1 to 2 mph on it for five minutes (or three minutes, whatever it takes to fatigue you), and then reduce the grade to where you can walk comfortably for a few minutes (or three or four minutes; this isn’t engraved in stone). Then raise the incline to 30 again for another round.
- And all the while, your hands are OFF the treadmill.
- This is the only effective way to acclimate to such a steepness.
Over a period of weeks, you’ll note you can increase the speed slightly to achieve the same fatigue, and/or you must walk the high incline for longer and longer to stimulate the same fatigue.
You will never progress as long as you hold onto the bar or console, any more than you’d progress with chin-ups if every time you pulled yourself up, you received assistance from a gravity machine.
Be patient and remind yourself how you’d sustain a walk on a steep hill outside: without holding onto anything, and very slowly.
Intimidation of a “moving floor” is the biggest obstacle to keeping one’s hands off a treadmill. I can’t stress enough the effectiveness of just standing on an unmoving belt set to 30 percent.
Then march in place. Then turn it on to half a mile per hour, and begin walking.
Take my word for it: A 1.5 mph pace at 30 percent, maintained for 20 minutes, without holding onto the treadmill, will provide a nice introductory workout to incline walking.
You may think 1.5 mph is too slow, give this a try and you’ll be surprised!
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
How Fast Should You Walk on an Inclined Treadmill ?

If you’re a treadmill incline devotee, chances are 99 percent you do this wrong, namely, going too fast, and here’s why.
The treadmill incline is perhaps the most incorrectly performed type of exercise because people “walk” way too fast for the selected angle.
I’m a personal trainer and have worked out at many chain gyms in different states; everywhere I’ve ever been, just about every person who uses a treadmill incline goes too fast and clings on, totally negating the intended effect!
How fast should you use a treadmill incline?
I declare with confidence that THE most incorrectly performed exercise involves the treadmill incline: holding onto the machine.
This mistake is angrily defended by those with an assortment of problems such as inner-ear balance issues, dizziness, neuropathy pain, recent knee or back surgery, and other ailments.
It’s not logical to assume that most people who jack up the incline and set the speed to 4 mph, then look like a water skier as they grip the bar, suffer from diabetes neuropathy, vertigo, hip arthritis, herniated disks or inner-ear problems. Many are also young and not overweight.
Many of the people who set the incline to super high and the speed to at least 3 mph are muscled gym rats.
They do superb in other exercises such as the back squat, bench press, chin-up and deadlift.
These are not fragile people. A person who cleanly squats 225 pounds is not likely to have a medical problem that requires them to hold onto a treadmill.
I’ve seen the same people who jack up the incline and speed and hold on for dear life participate in step aerobics and go up staircases without any issues.
So many people commit this error, that it’s illogical to conclude that the vast majority of them have medical problems.
So how fast should the treadmill go at high incline or any incline?
The formula is simple:
Choose a speed that’s similar to what you’d walk up an outdoor hill. How fast to use a treadmill incline mirrors your hiking speed outside.
How fast would you walk up an ongoing hill outdoors? Suppose this hill (assume it’s relatively smooth) is the same angle as the treadmill’s highest incline: 15 percent.
If you normally set the incline at 15 percent and the speed at 4 mph, even 3 mph, ask yourself if you’d be walking this fast up that ongoing outdoor hill.
Suppose that hill goes for miles. Really, would you be maintaining 4 mph, even 3 mph, on that 15 percent grade?
I guarantee it, if you planned on walking that hill for only 10 minutes, you’d naturally set your speed to around 2 mph or less!
What beast maintains a 4 mph walk up a 15 percent trail for 45 minutes?
As an avid hiker and trail runner, I have yet to witness this extraordinary feat. The only people who move this fast up a prolonged grade are trail runners.
How fast should you walk on a treadmill incline?
The same speed you’d move if outdoors on a hike.
You’ll then be able to let go. You don’t hold onto anything while hiking, so why hold onto a treadmill? Because you’ll fall off, right?
No. You won’t fall off if you move at your hiking speed!
Reduce the speed and let go.
This will force your posture to be upright.
If this is too difficult for your legs, don’t hold on. Instead, reduce the speed more.
Pretend you’re hiking outside.
Using a fast speed on a high treadmill incline while holding on subtracts significant workload, burns only a fraction of the calories shown on the console, and can cause repetitive stress injuries in the hips and shoulders.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Treadmill Walking Guidelines for Elderly: Do’s & Don’t’s

Most elderly people walk on a treadmill wrong, so here are guidelines for individuals of all fitness levels for optimal, safest results.
Most people 65-plus (and younger as well) do not walk on a treadmill correctly.
I’m a former certified personal trainer who has guided many elderly women and men on correct treadmill walking.
How do you walk on a treadmill wrong?
The vast majority of elderly individuals grasp the treadmill’s side rails or front portion while walking.
Though at first, to an unassuming person, this seems like the smart thing to do, it will actually cause much more harm than good.
I want to make it clear that this article pertains strictly to able-bodied elderly people, meaning, they do not require a walker or cane to ambulate, and are functionally sighted.
Most able-bodied seniors hold onto a treadmill. When I ask why, the No. 1 response is fear of falling off, rather than a physical disability or pain.
The next most common reason, believe it or not, is something like, “Everyone else is doing it.”
However, I’ve had clients who reported pain when walking, but then after removing their hands from the treadmill and walking with an arm swing for a few weeks, they reported either elimination of pain or reduction.
One 55-plus woman told me her shoulder pain disappeared.
Another 55-plus woman’s gait, including off the treadmill, improved markedly after she abandoned holding on, even though she had knee osteoarthritis.
Why is holding onto a treadmill harmful, even to elderly walkers?

It shuts down the body’s proprioception.
It eliminates the need to balance and know where your body is in space. By shutting this mechanism down, you prevent improving your balance.
The rails balance for you; why should your balance get better? Holding onto a treadmill outright prevents improvement in balance, coordination and ambulation.
“As we get older balance and proprioception are areas that tend to deteriorate,” explains Dr. Charles J. Pelitera, assistant professor of kinesiology and coordinator of the Health/Wellness Program at Canisius College, located in NY.
He continues, “Using a treadmill is a perfect opportunity to work on these areas because it is a controlled exercise with a specific pattern.
“Pumping the arms as opposed to hanging on not only helps with balance but increases cardiovascular output.”
It promotes bad posture.
This is obvious with most walkers who hold on, even young ones, and applies to people of all heights.

Look at this man’s poor posture. By holding on, he is molding a forward spine and hunched, rigid shoulders. This will have a ripple effect on his hips and knees.
However, depending on height, hand placement on the rails will force one’s shoulders to unnaturally jab up and down with each stride.
Taller individuals may exhibit forward posture. Holding on in front somewhere, as well, will still disrupt walking mechanics.
Regardless of height or where one places their hands, walkers (and joggers) will be forced into unnatural hip motion to compensate for the upper body’s lack of motion.

Very unnatural, regardless of age!
This can all be summed up quite simply: Holding on impairs natural gait and posture, and it can result in repetitive stress injuries of the hips, shoulders and even knees.
The last thing an elderly person needs is ruined posture, impaired gait mechanics and a false sense of security when it comes to walking outside.
“Changing of the gait can always lead to injuries, especially soft tissue injuries such as tendinitis,” says Dr. Oliver Zong, DPM, a foot specialist and surgeon based in New York.
He adds: “To the extent that holding onto the treadmill changes one’s gait, this could happen. Clearly it is better to walk or run naturally with a natural gait pattern.”
It’s unrealistic.
When you walk about in the community, you must rely upon your body for balance and control. Holding onto a treadmill fails to prepare you for real-life walking.

Look at this. How on earth can doing this make her walk more efficiently OFF the treadmill where there’s nothing to hold onto? If all she wants is a faster heart rate, holding on will STILL cause the other harm already explained.
Though one might argue that a treadmill, regardless of how it’s used, is unrealistic, this is actually not true.
One’s feet/legs and core must work to keep up with a moving tread to prevent falling off.
This is exercise, and based on my own experience with treadmill workouts, it definitely transfers to outdoor activity! As long as you swing your arms!
Use the rails or front to momentarily hold on while changing the program, sipping water, rubbing one’s eye, wiping away sweat, turning to greet someone or taking heart rate.
- And by the way, the calorie-reading is meaningless because the treadmill can’t tell if you’re holding on or not.
- Walking without holding on will burn 20 percent more calories.
How can elderly walkers learn to swing their arms on a treadmill?
The user below demonstrates exactly what seniors’ hands should be doing on a treadmill.
And don’t forget, I’m referring to seniors who can walk without assistance in their daily lives.

One of the elderly men who had told me he was afraid of falling off had the incline at 15 percent and the speed at 4 mph!
Even my young clients couldn’t maintain a hands-off pace at this intense setting!
If you like a high incline, reduce the speed until you can walk with an arm swing. This will probably be around 1 to 1.2 mph — possibly even less than one mile per hour.
When the incline is maximum, there’s really no such thing as a “too slow” speed.
If you like a fast pace, then reduce the incline. An intense program setting, in combination with holding on, will prove fruitless and waste your time.
To preserve or improve balance, walking efficacy, coordination, fitness, posture and lose weight, it’s crucial that elderly people use an arm swing when walking (or jogging) on a treadmill.
 Dr. Pelitera is the owner of Pelitera Fitness Consultants, which specializes in athletic training, weight loss and strength training.
Dr. Pelitera is the owner of Pelitera Fitness Consultants, which specializes in athletic training, weight loss and strength training.

Dr. Zong, a foot and ankle surgeon, has appeared on national and local TV programs such as “Good Morning America” and “The Doctors.”
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Iammotos

Should You Hold Onto Treadmill while Walking Backwards?

Find out why you should not hold onto a treadmill while walking backwards…
Nearly every time when I see someone walking backwards on a treadmill, that individual is holding onto the side rails.
When I was a personal trainer at a large gym and saw this, I’d tell him or her that this was wrong and that it defeated the purpose — whatever that person’s goal was.
“Walking backwards hands free improves posture,” says Dr. Tom Carpenter, corrective exercise specialist, certified personal trainer and chiropractor, inventor of Stand Corrected™, a portable harness-like stretching tool that helps alleviate back, neck and shoulder pain.
“It does this by engaging the posture muscles to a much higher level than normal,” continues Dr. Carpenter. “It strengthens the quads and calves as well as the stabilizing muscles for the hips, knees and ankles.
“Your body is forced to balance itself to a greater degree than normal by walking in a completely different way than it is accustomed to.
“Even though it may feel a little awkward at first, letting go of the support and allowing your body to learn to move more naturally when walking backwards will increase coordination, balance and stability.”
I’m a former certified personal trainer with a large gym, and I’m going to explain why even a light grip defeats the purpose of walking backwards and has other disadvantages.
Your first reaction might be, “But holding on is smart because it prevents falling off.”
However, if the speed is slow enough, you won’t fall off. I’ve had many clients walking backwards on a treadmill and I’d start them off at 1 mph.
The problem is that people typically try to walk backwards at much faster speeds.
Though I’ll also point out that sometimes I’ll see someone holding on while walking backwards at a very slow speed.
Regardless of speed, holding onto a treadmill while walking backwards will defeat the purpose of this different approach to movement.
So why do you walk backwards on a treadmill?
You have a reason or two.
- Is it because you read somewhere it helps alleviate knee pain?
- Or perhaps you read that “muscle confusion” will burn more calories.
- Maybe you’re bored moving forwards?
Reason aside, you should teach yourself NOT to hold on, because the whole point of walking backwards is to — walk backwards in the true sense of the word, to keep up with a moving tread in the opposite direction.
If you hold onto the rails, the rails become stabilization points, relieving your body’s stabilizer muscles (which include those in the core) from their duties. What good is this?
Furthermore, holding onto the rails encourages bad posture. Next time you see someone holding on while walking backwards, note their posture: shoulders, neck, spine, the whole works. The entire gait is wrong.
Now, if you do not hold on while walking backwards on a treadmill, you will be forced into executing perfect posture! I mean perfect!
Stabilizer muscles will be fully engaged to prevent you from falling, and major muscles will be doing all the work.
Start the Right Way
Start out at 1 mph and walk backwards without holding onto the treadmill. Watch your feet if you must.
Or watch the edge of the tread belt, or even the floor just beyond it; you’ll find your sweet spot.
As you get used to moving hands-free, increase the speed a little.
When your legs must keep up with a tread that’s moving backwards, without your hands assisting on the rails, this will force your legs to become more efficient; it will force your ankle, knee and hip joints to become stronger in a unique way.
To reap benefits from walking backwards on a treadmill, go for five to 10 minutes, and swing the arms naturally in synch with your body rather than hold onto the rails.

Photo credit: Aleesia Forni
Based upon 30+ years of experience, Dr. Carpenter’s practice approach reflects his belief that restoring optimum health and function will enable his patients to enjoy a much greater amount of vitality and wellness. Chiropractic care is true health care, not sick care!
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why the Fat Isn’t Coming Off Despite All Your Treadmill Walks

The reason you haven’t lost weight from all that treadmill walking will shock you, but it can easily be remedied.
Why is it that you haven’t lost a single pound or have experienced only marginal weight loss, despite months on end of walking on a treadmill?
If it’s not the No. 1 reason that prevents people from weight loss despite loads of walking on a treadmill, then it’s certainly the No. 2 reason:
Holding Onto The Machine
Yes, that’s right. One of the biggest saboteurs of weight loss attempts is holding onto a treadmill.
Ironically, with so many men and women struggling to lose weight, desperate to burn body fat, the weight loss saboteur of holding onto a treadmill is extremely prevalent.
Now before I go on about how to solve this problem, I need to emphasize that this article targets the general population of treadmill users in a gym, rather than exceptional populations such as the visually impaired who would need to hold on.
When I see hoards of people holding onto a treadmill while walking, I see able-bodied men and women, many in their 20s and 30s, who will often trot up the gym’s staircase without a problem to do some dumbbell work on the second floor.
One faithful treadmill-holder whom I had observed was a martial arts instructor!
What — he could throw kicks in the air but needs to hold on when using a treadmill???
I’ve witnessed these trainees participating in group fitness classes and even doing barbell squats!
So as you can see, physical handicap does not play into this.
People with physical handicaps, in fact, rarely use treadmills — at least at gyms; I’ve seen them on the stationary bike, elliptical machine and rowing machine.
If you haven’t lost weight despite spending months and months walking on a treadmill, your question to yourself should be:
“Where are my hands while I’m walking?” It should NOT be, “Why am I cursed with fat genes?”

NO, NO, NO! This won’t cut it. Hold on for temporary balance checks, but not for the whole “workout”!
When you swing your arms, your body must work harder to prevent falling off the moving tread. This means more calories burned = weight loss.
Holding on removes work from many important muscles, including those of the core!
Perhaps in desperation to lose weight, you’ve been using a faster speed and/or higher incline.
Guess what: A faster speed or higher incline means a tighter grip by your hands! You will not lose weight this way.
Holding on burns 20-25 percent fewer calories.
The calorie display is inflated because it’s determined by the speed and incline, not the trainee’s effort level!
Pretend you’re walking outside next time you use a treadmill. What would your hands and arms be doing?
Then do that. If you think you can’t, then set a slower speed and/or lower incline until you can swing your arms.
If you want to lose weight from walking on a treadmill, it just doesn’t make any sense whatsoever to keep the upper half of your body paralyzed as a result of holding on.
In addition, “Reaching a plateau in weight loss often indicates that a change is needed in the program,” says Jacque Crockford, MS, CSCS, an ACE certified personal trainer and an ACE exercise physiologist.
“Begin jogging on the treadmill, increase incline, add intervals, introduce strength training. All of these are great ways to get over a weight loss plateau.”
 Jacque Crockford is also the exercise physiology content manager at ACE (American Council on Exercise) and has been an personal trainer for 15+ years.
Jacque Crockford is also the exercise physiology content manager at ACE (American Council on Exercise) and has been an personal trainer for 15+ years.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Kzenon

Treadmill: High Incline Holding On vs. Low with Hands Off

Here’s the answer to the question of which is more effective: holding onto a treadmill at high incline or letting go at lower incline?
Many people wonder which is more effective for weight loss and fitness: using a high incline while holding onto the treadmill, or using a low grade but then not holding on at all.
The answer is basic: Holding onto a treadmill during an incline is never better than letting go.
Now, if you want to get argumentative about this, you can always compare holding onto the highest incline at 4 mph to not holding onto a 2 percent grade at 1 mph.
In this unfair comparison, the holding-on version will burn more calories.
But let’s be fair and real about what to compare.
A fair comparison would be a 15 percent incline at 3.5 mph while holding on, matched up to a 7 percent slope at 3.5 mph with an arm swing.
The lower angle with hands off wins hands down for calorie burn, weight loss and cardiovascular training.
You don’t need science to know this.
Try it yourself:
For 10 minutes, “walk” at the highest incline at 3.5 mph while holding anywhere on the treadmill. How do you feel?
On another day (so that you don’t use the first part of this test as an excuse for how fatigued you get during the second part), walk the 7 percent incline at 3.5 mph, without any holding on; swing the arms naturally.
Sustain this, no holding on, for 10 minutes. How do you feel?
Your first rating of fatigue level will be far lower than your second.
This is because the second part of this test (lower incline, hands off treadmill) is more demanding on the body, much more demanding indeed.
The calorie readout will be higher with the higher incline.
Do not let this dupe you into thinking that a high incline session while holding onto a treadmill is better than a low incline without holding on.
The only reason the calorie total will be bigger is because the total is determined by the steepness of the incline, not by how hard you’re working on the machine.
To prove this, walk level at 2 mph for five minutes while holding on, then note the calorie total.
Now, hold 5 lb. dumbbells in each hand and again walk level at 2 mph for five minutes.
You’ll burn more calories walking while holding 10 pounds than walking with your hands on the machine, yet the treadmill’s calorie total will be precisely the same!
Letting go at a lower incline means that more muscles will be forced to work: low back, abs, hamstrings, glutes, calves, quads and more.

When you hold on, even at high incline, many of these muscle fibers are deactivated.
This is a fake vertical position that’s being generated by gripping the front of the treadmill.
The result? Significant subtraction of workload from your lower body.
In fact, even a 4 percent incline at 3.5 mph without holding on beats out the high grade while grasping the machine.
Holding on encourages bad posture and poor biomechanics and can result in repetitive stress injuries to the hips and shoulders.
“A high incline puts more of a concentration on the muscles in the leg,” says Dr. Charles J. Pelitera, assistant professor of kinesiology and coordinator of the Health/Wellness Program at Canisius College of NY.
“When one is holding on, they reduce the tension and thus the opportunity to add an overload and thereby more development.
“The effect of no hands in a low incline and holding on in a high incline will not be the same because of the simple concept of gravity and the role it would play in resistance.”
You now know the many reasons why a lower incline without holding onto the treadmill is far superior to a high grade while keeping your hands on the machine.
Dr. Pelitera is the owner of Pelitera Fitness Consultants, which specializes in athletic training, weight loss and strength training.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Do You Know Your Treadmill Etiquette at the Gym?

There’s a surprising number of ways to be rude with treadmill use at the gym; chances are you’ve breached one of these rules of etiquette with the treadmill.
If you’re a treadmill user, it’s so important to be aware of treadmill etiquette.
There are so many ways a person can be inconsiderate when using this particular piece of equipment at the gym.
In no particular order, here are the top treadmill etiquette infractions that I’ve observed over the years, at many different gyms (these behaviors are universal):
Leaving the treadmill up at a high incline after exiting it.
Instead, reset it back to zero for the next person.
Leaving germy junk in the treadmill’s cup holder.
This includes used tissue paper, empty cups and bottles, and gum wrappers. Yuck.
Using a treadmill that, due to a malfunction, creates a loud squeaky noise.
This typically occurs even when several other machines are available.
The noise signals that the equipment needs servicing and thus, should not be used.
Before using a treadmill, turn your headset off, in the event that a loud headset would muffle the machine’s squeaking. This way you’ll know if there’s a problem.
Creating a loud, squeaky noise by allowing your feet to strike the juncture of the tread belt and machine’s base up front.
This only happens when people hold onto the equipment, a bad habit that’s not even necessary beyond the brief heart rate check or to momentarily steady yourself.
Jogging like an elephant.
Ironically, these guilty joggers are not heavy people! Often, they are lean, and the speed isn’t necessarily fast; sometimes it’s 5 or 6 mph. So why do they sound like elephants?
Though some treadmills have defective belts that create thunderous noise no matter how delicate the user, I have witnessed plenty of times someone’s feet slamming with each stride, yet on that very same treadmill, I have witnessed other users, including heavier ones, make a fraction of the noise while using the same speed or faster.
I’m banking that these users figure that the louder their feet are, the harder or more effective the workout.
But hitting your feet hard to the tread will not increase the effectiveness of the workout.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Depositphotos
Should You Hold Onto Treadmill During Sprints or Hard Runs?

Find out why you won’t get results by holding onto a treadmill during sprints or hard runs.
One of the biggest mistakes in exercise is that of holding onto a treadmill, even when the user is “sprinting” or running hard at a fast clip. I’m a certified personal trainer.
I see this quite often: The user cranks up the speed at a zero incline, grips the bar in front and “runs” for a brief period, then slows the speed and releases their hands during their “recovery.” This is not the proper way to conduct interval training.
I like to point out the case of a lean, attractive woman who worked out from 5 a.m. to 7 a.m. Monday through Friday.
Her workout included 7 mph one-minute runs on a treadmill, during which she’d plaster her palms around and over the top of the console.
Because of her tanned, lean physique, many naïve people thought she was doing things the right way.
She actually spent a lot of time on the treadmill, plus lots of time strength training. She watched what she ate.
But this didn’t excuse her from committing such a blunder on the treadmill.
Because her body was so used to that steel-hard clasp of her palms at 7 mph, there’s no way this would carry over to running outside where there’s nothing for her hands to latch onto.
Think about it: The harder or faster you run, without holding onto anything, the more your abs and low back become engaged, along with your butt and leg muscles.
This is why competitive short-distance runners have killer abs and wonderful glutes!
If you hold onto the treadmill (front bar or behind top of console), then the faster the speed, the tighter your grip will be.
The more locked up your arms and shoulders are, and the more deranged the motion of your hips are, the more you’ll set yourself up for possible future hip strain.
The foot strike becomes unnatural, increasing risk of plantar fasciitis (heel pain). The entire gait pattern becomes warped and will not carry over to running, especially sprinting, on the basketball court or outside.
There is a HUGE difference between sprinting while holding onto a treadmill and sprinting naturally with an aggressive arm pump.

Shutterstock/Den4is
“By not holding on the treadmill, you will raise the heart rate without having to increase speed,” says Jacque Crockford, MS, CSCS, an ACE certified personal trainer and an ACE exercise physiologist. “It is also not safe to hold the treadmill while running, as it can cause more balance issues or tripping.”
Listen to someone running very fast on a treadmill while gripping it. Their feet slam down with each step.
That’s because the gait pattern is disrupted. Their lower body is not keeping up with the fast speed.
What’s happening is that the bones in their arms, and their hand grip, are providing significant assistance.
If you cannot run a speed without holding onto a treadmill, then that speed is too much for you, be it 7 mph, 12 mph, 14 mph or 5.5 mph. Everyone, even top athletes, has a speed limit.
Sprint as hard and as fast as possible without holding onto the treadmill.
If you can do this for only 15 seconds, that’s good! This is your work interval.
Sprinkle in several of these intensity intervals during a walk or slow jog. By definition, a sprint is supposed to be very brief.
Jacque Crockford is also the exercise physiology content manager at ACE (American Council on Exercise) and has been an personal trainer for 15+ years.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

How Obese People Can Use Treadmill Desk to Reduce Sitting Time

If you’re obese, don’t let that stop you from using a treadmill desk to help offset the “sitting disease,” which is as dangerous as smoking.
If you’ve been thinking of getting a treadmill desk to discourage excessive sitting while doing computer work, but are reluctant because you’re obese, I have good news.
And that is this: Obesity is no deterrent to using a treadmill desk. As a personal trainer, I’ve worked with many very overweight clients, and plus, I use a treadmill desk, so I know all about this device.
How Obese Walkers Can Adapt to a Treadmill Desk
Initially use the device for 10 minutes at a time, or even five minutes if that’s all you can tolerate, and set the speed to 0.5 mph and a zero incline.

Do not hold on if you’re simply reading off the computer screen. Use of the mouse and keyboard will necessitate resting your forearms and portions of your hands on the structure, but when you’re not using the mouse or keyboard, swing the arms.
This is very important; one reason is because a natural arm swing will encourage good posture, proper gait, and engage the low back muscles.
No matter how soon you may become uncomfortably fatigued, this is no reason to give up the pursuit of using a treadmill desk. Simply step off of it when fatigue becomes overbearing and take your usual seat.
The caveat of switching back and forth is that you’ll need to keep transferring your computer back and forth, unless you have two computers: one at the treadmill desk and one at your sitting station.
Time your sessions using the treadmill desk:
Set a timer for five, 10, 15 or more minutes. Don’t overdo it at first. Don’t try to walk any marathons.
Sudden prolonged walking in a sedentary obese individual can result in strained feet, hurting heels or sore knees.
Wear comfortable shoes. If your shoes are not comfortable, don’t try to tough it out. When using a treadmill desk, always wear supportive walking shoes.
If your lower back begins aching, do not hold onto the machine (again, the exception for arm/hand contact is when you’re using the mouse or keyboard.
If your lower back begins aching, step off the machine and take a break from it. An aching lower back simply means that the muscles are fatiguing from getting worked. Over time these muscles will adapt!
Obese individuals should walk as much as possible.
Obese people can benefit from a treadmill desk and should not let their size discourage them.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

30 Percent Treadmill Incline: How Not to Hold On

Here’s a simple way to reap maximum benefits with a 30 percent incline, which can be achieved only if you do not hold onto the treadmill.
You may think you’re getting an amazing workout by using a 30 percent incline on a treadmill, but if you’re holding onto the machine, you’re cancelling out the effects of this generous slope.
I know what you’re thinking: “How can anyone walk on a 30 percent incline without holding on? They’ll be thrown off!”
Have you not ever walked up a steep hill outdoors? Were you holding onto anything?
And certainly, you’ve walked up flights of stairs countless times without grasping anything for support. Why should an angled treadmill be any different?
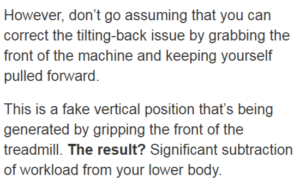
If your entire body is leaning back (like a water skier) while you’re holding onto the front bar with straight, locked-out arms at an incline — and you release your hands in that position — then yes, you’ll fly backwards off the machine.
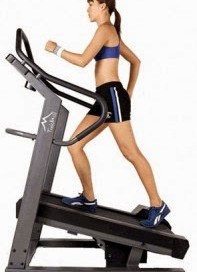
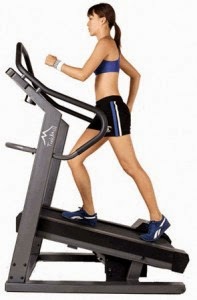
How about standing straight (no leaning back) as you walk, so that your body is vertical?
Reduce the speed so that the tread isn’t whizzing under your feet at such a high incline.
NOW let go. You won’t fall backwards any more than if you were walking outside up a 30 percent hill.
How Not to Fall Off a Treadmill at 30 Percent Incline Without Holding On
Again, keep your body vertical — as you would when walking up a staircase, which is actually angled more steeply than 30 percent.
When you climb a staircase or steep hill outdoors, your body is vertical, which is why you don’t fall backwards.
Apply this practice to a treadmill that’s set at 30 percent slope. Set the speed to 1 mph and start walking with your arms at your sides.
If you’re free of any neurological disorder that impairs balance when walking, you will not fall off at such a slow speed.
At 1 mph, walk 10 minutes at 30 percent incline without your hands making contact with the treadmill.
What seems like a crawl is actually comparable to the pace that you’d choose if hiking in the mountains on a similar grade.

Even WITHOUT the backpack, you probably would NOT exceed 1.5 mph sustained on this angle of a hill — which appears to be close to 30 percent.
Because you’re now vertical, with significant ankle flexion, you should feel the entire backside of your lower legs working.
If you remain vertical while holding on (which would require a continuous pulling against the bar with your hands), this will relieve the work from your legs.
Thus, a vertical body while holding on with a “tugging” grip is NOT the same as a vertical body while walking hands-free. NOT THE SAME!
With your hands off, you may also soon start feeling a burn in your hamstrings,.quads and/or low back, especially if you slightly increase the speed.
All these signs mean that your body is out of condition for high incline walking.
Holding onto the treadmill will not condition it, not in the least, never, even if you’re tugging yourself into a vertical position.
To set the treadmill at 30 percent, speed at 3 mph and THEN hold on is just plain insanity.
Now, if 1 mph proves to be unchallenging, then raise the speed to 1.5 mph and see how five minutes of that goes without holding on. Experiment to find the speed for which you can sustain.
The only way that you’ll gain fitness benefits from 30 percent incline work on a treadmill is if you mimic walking up a same-grade hill outside. And how would you walk outdoors?

Stockfreeimages/Kapu
1) Body vertical
2) Hands not holding onto anything
3) Pronounced hip and knee flexion due to the acute angle formed by your vertical body to the hill before you.
These three features must be duplicated on the treadmill, and the only way to do that is to keep your hands off the machine (except for brief heart rate check or brief, temporary steadying while you adjust the speed, wipe sweat or sip water).
It’s extremely unrealistic to think you can walk a 30 percent incline at 3 mph without holding on.
To sustain this pace hands off requires exceptional cardiovascular and musculoskeletal conditioning. So just because you’re not this advanced doesn’t mean you should hold on!
Instead, go down to 1.5 mph or 1.2 mph or whatever — and let go. If this is too difficult, go down to 1 mph. Remember, you’re at 30 percent incline; you can’t expect to move like a mountain lion.
Using a 30 percent incline without hanging onto the treadmill will force adaptations in your core, hamstrings, calves, Achilles tendon, quadriceps and other muscles.
If you hold on, you’ll be wasting your time. If letting go is too exhausting, you’re going too fast, even if it’s “only” 1.5 mph.
Another Option
“There is a slight learning curve to using a treadmill without holding on,” says Dr. Charles J. Pelitera, assistant professor of kinesiology and coordinator of the Health/Wellness Program at Canisius College, NY.
“This refers to proprioception or knowing where your body is in space. A person who is not in ‘shape’ should be encouraged to not hold on — and they can work on a progressive routine that ‘weans’ them off of holding on.
“Have them start off by trying one minute with hand contact, one minute without, and begin to decrease the hand contact time and increase hands-free time as they progress along. Confidence and consistency play a large role in this.”


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}