

Earliest Brain Tumor Sign in Dogs: Subtle But Observable

What is the earliest brain tumor sign in a dog?
I can only speak from my experience with my parents’ German shepherd.
But I’m sure that this very early sign of a brain tumor in a dog is not unique.
If you’ve been noticing subtle changes in your dog’s behavior lately, do not be satisfied passing this off to “old age” or “he’s getting older” or anything like that.
When I think about it, the earliest sign that something wasn’t quite right with the dog was that he wasn’t as enthusiastic about maintaining play with a ball. Note the key word here: maintaining.
The dog was responding as enthusiastically as always to the “Let’s Play!” signals, which were verbal or visual.
And at the beginning of the play sessions, he was exuberant and puppy-like, though over eight and a half years old. But soon after he’d lose interest.
Normally, the dog went for 35 throws in the backyard, retrieving the ball to me, and then at around throw No. 35 (though historically sometimes about 30), instead of bringing the ball to me, he’d pause at the stairs leading up to the deck; this was his communication, since youth, that he wanted to go inside and drink a lot of water.

The dog was now doing this only after about 10 throws.
But I didn’t think anything of it, and figured maybe it was the arthritis in his knee that he’d been diagnosed with some weeks prior.
Maybe he was getting older, even though only weeks before, he was bounding around like a puppy in the snow, and recently had gone for 40 throws.
Indoors we had a game: I’d stand by a particular door and kick a football-shaped chew toy across the kitchen walkway which was lengthy enough for the dog to bolt after the toy, then bring it back to me. He’d do this until his master had had enough.
I was noticing that he’d retrieve only a few times, then go to his pillow and plop down.
Or, he’d proceed to retrieve, but not follow through and instead veer off to his pillow. Again, I didn’t think much of it.
These were the earliest signs of a brain tumor that he’d be diagnosed with just a several weeks later a few days after his first seizure.
The brain tumor was insidiously changing the dog’s personality; I don’t want to say attitude or intelligence; this seemed mostly like a personality thing. By no means was the dog lethargic; he had plenty of energy.
He just didn’t want to maintain play. I realized that dogs eventually get old and tired, but this dog’s ninth birthday was several months off yet, and when the aging process slows canines down, it doesn’t happen this rapidly: from 40 throws in late January to just 10 or seven throws in mid February?
Another effect of the brain tumor was that the dog began coming back to me without the ball.
I’d have to keep telling him to go get it, walking towards it, pointing to it, sometimes getting it for him, as though he was either forgetful or simply lost interest, I couldn’t tell which. I thought he was just being stubborn.
Historically, fetching sessions included the dog retrieving the ball and then continuing on around a corner in the yard, ball in mouth, to relieve himself, then returning to me with the ball.
But now, he was not only relieving himself and returning to me without the ball, but he kept making that leftward excursion to the area where he’d normally relieve himself.
He kept wanting to go over there, but at the time, it didn’t occur to me that the “leftwardness” was the lure, not the actual relieving area.
(Several days preceding the brain tumor diagnosis, the dog kept circling around the kitchen leftward; and since then, had a persistent compulsion to circle leftward and make left turns in the house; the brain tumor was on the right side of the brain.)
The relieving area was hidden by the façade of the house, so I never knew what he was doing back there.
I’d approach and there the dog would be, just standing there, looking towards me, not in the act of any defecation, ball not in mouth.
I’d tell him to get the ball; he wouldn’t. He’d continue standing there or come to me, no ball.
Sometimes he’d trot up to the deck after I told him to get the ball; the ball was not on the deck.
It was in the yard either not touched after being thrown by me, or having been carried over to the defecation area by the dog, but then apparently forgotten that it had been deposited there.
The dog would be trotting around on the deck as though searching for the ball, looking down at me. Despite all this, it never dawned on me that a brain tumor was at work.
Though these were the earliest signs of the brain tumor, this didn’t mean that the brain tumor was small.
Often, by the time a brain tumor in a dog begins presenting with symptoms, the brain tumor is large.
Other than these lapses during playtime, which I called “disorientation” and “he seems to forget why we’re out there,” the dog was completely normal — for a few weeks, that is.
But then other symptoms began showing up, such as not showing interest in other dogs nearby, when normally he’d bark like crazy.
Really, who starts thinking brain tumor when subtle behavior changes in a dog start occurring? Some well-informed people actually do start suspecting a brain tumor.
But a brain tumor in our dog was the furthest thing from our mind.
Other symptoms started showing up over just a matter of days, and then he had the seizure, which led to a complete workup of his body, but not his brain (the vet clinic wasn’t equipped for a neurological exam).
When the vet called and said everything in the dog’s body was in magnificent shape (heart, lungs, liver, kidneys, blood work, chest X ray), my mother was thrilled.
Not me. I told her, “If everything in his body is healthy, that means the problem is in his brain!”
With his body being in perfect condition, this meant that the seizure could have only been caused by a brain tumor, or quite possibly another condition that the vet called “doggie dementia.”
Or possibly cerebral inflammation. Well, by then, I just knew the dog had a brain tumor.
The diagnosis a few days later was a “fairly large tumor” in the “thinking part of the brain.”
Within several days of the diagnosis, the dog had pretty much lost all interest in play sessions, and never recovered his enthusiasm for retrieving balls.
If your dog starts exhibiting behaviors that are peculiar, out of character, or cannot truly be explained by age, fatigue, a change in diet, or stress — it certainly wouldn’t hurt to get an MRI of the dog’s brain; an MRI is the only way to diagnose a brain tumor in a dog, and the earlier, the better.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Dog Keep Pushing or Rubbing Nose, Face Into Things? Warning…

Warning: If your dog has been pushing or rubbing his nose or face against things or into things for no apparent reason, have your pet examined by a veterinary neurologist.
This new behavior can signal a brain tumor.
Have you noticed lately that your dog seems to be pushing his nose into things like his pillow or against stationary objects like stairs or heavy furniture?
Or perhaps it seems more like the dog is rubbing his nose against things — not to sniff them out, but almost like a compulsion to just rub or push.
It may also appear that your dog is pushing his face, not just the nose, against or into things (again, like his bed, or perhaps a bush outside).
My parents’ dog was diagnosed with a brain tumor.
I wondered, in hindsight, if there had been earlier, more subtle signs of the brain tumor that — at the time, we overlooked. It seemed that the symptoms of the brain tumor came on suddenly … seemed.
…The German shepherd went from always being normal to one day he didn’t want to play with one of us; this was highly abnormal because he always wanted to play ball.

A few days later he was making gagging and retching sounds, and actually vomited.
And he suddenly began restless circling around the kitchen island. A few days later he had a seizure.
But could there have been signs long before that very first symptom (not wanting to play) that we missed?
Nobody missed the fact that the dog had suddenly started shoving or pushing his nose into his pillow — one of those large doggie pillows you see at pet supply stores.
The dog would keep pushing his nose into the edge of the pillow, making the pillow travel across the hardwood floor.
We thought he had an unresolved itch. We also spotted the dog pushing his nose into the bottom stair of the staircase. Again, we thought he had a stubborn itch.
Something having to do with the dog’s nose was really annoying him.
At one point we took him to the general veterinarian for a follow-up regarding an injured knee, and I mentioned the nose-rubbing behavior.
The veterinarian simply grabbed the dog’s muzzle, felt around and visually inspected it and the gums, then said everything looked fine. We bought that.
When the dog was diagnosed with a brain tumor a few months later, I didn’t make the connection — until I saw the printed report by a veterinary neurologist: the diagnosis was a nasal caudal frontal mass.
I also recalled the day before over the phone with the neurologist; he mentioned that the brain tumor was extended into the nasal cavity.
It hit me: That’s why our dog had been pushing his nose against the pillow and stairs!

©Lorra Garrick
And perhaps that’s why he had suddenly taken an interest in rubbing his body up against the pine trees while he circled them — or maybe it was his nose, and it only seemed like his entire body?
Those trees had been there since the nearly 9-year-old dog was a puppy, so why only at age 8 and a half was he suddenly interested in rubbing against the trees, the rubbing seemingly beginning at his nose?
After visiting some reputable websites about brain tumors in dogs, I am convinced that this nose rubbing and pushing behavior was the earliest symptom of the brain tumor.
So if your dog has been doing any kind of pushing, rubbing or shoving with his nose against various objects, get your pet to a veterinary neurologist.
Keep in mind that it’s normal for canines to nudge their nose against their food bowl before eating, but sudden nose rubbing or pushing elsewhere warrants a neurological exam.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources:
vetinfo.com/dog-brain-tumor-symptoms.html
natural-dog-health-remedies.com/canine-brain-tumors.html
natural-dog-health-remedies.com/missing-my-dog-spanky.html

Fast Acting Antidepressant May Already Be on Market

Here’s why it’s actually possible for a prescription antidepressant to work within 24 hours like a charm.
Antidepressants typically take a while before their effects begin kicking in, sometimes several weeks.
In fact, drugs.com says that it may take “up to four weeks” for Cymbalta.
When I urged my father to convince my mother to take an antidepressant, he said, “It’ll take two weeks before it starts working, and by then, she’ll be fine.”
Being a believer in that possible exception to the rule, I persisted, and finally, after six weeks of bantering with my father, he relented.
And I’ll never forget how I felt when I was walking in the parking lot of the medical clinic towards my car, holding the little bag with the bottle of Cymbalta in it.
I just knew that this antidepressant would start working within 24 hours.
And I was right. The next day, my mother had a look of life in her eyes that I had not seen for almost two months.
She said she “felt human again,” and was talking about baking bread, when just the day before, she could barely get out of bed and spoke of “going into the woods to die.”
And this was no momentary spike in mood; the effect was sustained, though (as predicted by my brother, a pharmaceutical chemist) she ultimately required a few dose increases when the effect began wearing off (this is typical with the induction of an SSRI drug).
So never let the “It will take several weeks to kick in” mantra influence your judgment.
“Typically, SSRI’s take days to weeks to take into effect, depending on their chemical structure and half-life,” says Natasha Fuksina, MD, an internal and integrative medicine specialist who combines traditional, integrative and functional medicine to restore health and function.
“The only plausible explanation beyond placebo for the SSRI to work ‘literally overnight’ would be if your family member used the SSRI with a very short half-life.”
For some individuals, an antidepressant that would normally take a few weeks to start working (like Cymbalta and other SSRI’s on the market) might just, strangely, work like a charm literally overnight.
Though ultimately, my mother’s depression may have been caused, or at least, exacerbated, by hypothyroidism (low thyroid was eventually confirmed with a blood test), we will never know to what extent it was independent from the thyroid disorder.
An antidepressant drug may be the only option left when the patient requires 20 minutes of prodding to simply sit up in bed in the morning, refuses to eat, has frequent sobbing spells and has become non-functional.
You can’t snap someone out of severe depression by denying the problem.
What does “half-life” actually mean?
Dr. Fuksina explains, “For example, venlafaxine (Effexor) has a half-life of four to seven hours.
“Let us look at the basics of pharmacokinetics. A half-life of a medication is the time it takes to eliminate its concentration by 50%. Same time goes for accumulation of the drug.
“It takes four to five half-lives while continuously taking the medication to reach its steady state.
“So if a person took one dose of Effexor, in about four to seven hours after the first dose, the concentration of the drug in the blood would reach 50% of the steady state.
“Sometimes, even half of the needed dose can be effective to help with someone’s symptoms.”
 Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/traveliving
Sources:
drugs.com/cymbalta.html
sciencedaily.com/releases/2014/04/140430161301.htm
Why a Positive D-Dimer Is Not Always a Blood Clot

Here’s why you shouldn’t panic if you learn an elderly loved-one’s D-dimer test came back positive and indicates a blood clot.
The D-dimer blood test is to screen for a blood clot, and doctors routinely order this test when a patient presents to an ER with symptoms that a blood clot in the lung can cause. I learned this firsthand with my mother’s ER visits.
A D-dimer result is more likely to be a false-positive in a person over age 50.
That’s potentially a lot of CT scans (the standard follow-up to a positive D-dimer) and hence, a lot of unneeded radiation, for all those false-positive results.
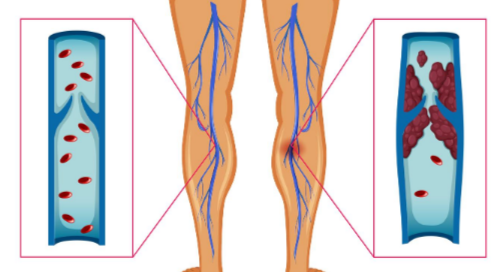
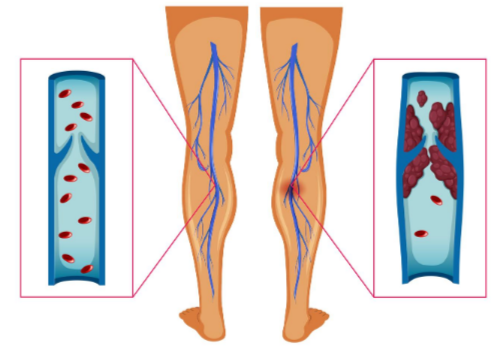
What is a pulmonary embolism?
“A pulmonary embolism occurs when an artery in the lungs becomes blocked by something that travels through the circulatory system and lodges in the lung,” explains Christopher J. Hanifin, PA-C, who was previously a physician assistant in open heart surgery with Cardiothoracic Surgery of South Bend in South Bend, IN.
“The most common culprit is a blood clot that forms in a large vein in the leg – a deep vein thrombosis – and then breaks loose and is carried to the lungs,” continues Hanifin.
“Depending upon the amount of lung involved, this is usually associated with some degree of shortness of breath.
“PE is also commonly associated with chest pain, which can be vague and difficult to distinguish from other causes of chest pain.”

Shutterstock/michaelheim
Even if you go to the ER with ONLY chest pain, you’ll get a D-dimer test — which is done from a blood sample.
It makes sense that older age is included in the screening, as was in a study that appears in the March 19, 2014 issue of JAMA.
Age of the Patient
The report in JAMA says that using a person’s age to raise up the threshold for an abnormal D-dimer result appeared to be safe, and it led to fewer healthy people getting a diagnosis of a pulmonary embolus.
A blood clot causes a breakdown product called D-dimer.
A negative blood result means you don’t have a pulmonary embolism. But with increasing age comes an increased likelihood of a positive result, even if there are no blood clots.
This makes the test less reliable for elderly patients when compared to younger.
Dr. Marc Righini’s study redefined the test value by multiplying the participant’s age by 10 if the patient was at least 50, and using this numerical result with the blood test result.
The team was able to safely exclude a pulmonary embolus diagnosis in elderly patients who were suspected of having a PE.
Over 3,300 participants with suspected PE were involved.
When a patient’s age with a multiplication by 10 was factored into the blood test result, the PE diagnosis was safely excluded.
Some years ago while at the health club, minutes before I was scheduled to train my next client, I called my father to see how my mother was doing, as he had taken her to the emergency room because she was having shooting pains in her upper abdomen.
He told me that the doctor suspected a blood clot in her lung.
This scared the willies out of me and I had difficulty pretending everything was alright while I trained my bubbly client.
“A laboratory test – the D-dimer – can also suggest the presence of a clot in the body, but this test becomes less reliable in older patients,” says Hanifin.
Too bad I hadn’t known, at the time, that being over age 65, in and of itself, can yield a positive D-dimer result in the absence of a blood clot.
Turned out my mother’s lungs were just fine.
Several years later, my mother would end up having at least three more emergency room D-dimer tests, all coming back positive! (Again, lungs just fine each time.)
The second time my mother’s D-dimer was positive, I didn’t have the fear that I’d had several years prior at the gym.
That’s because I knew that it would probably be another false-positive (and it was).
The third time the D-dimer was positive? I thought, “Here we go again, another CT scan and unnecessary radiation.”
Hanifin explains, “A patient presenting with chest pain or shortness of breath with risk factors for PE should generally have a CT scan performed.
“A CT scan can usually identify the presence and extent of any clots fairly reliably.
“A further benefit of the CT scan is that it can often identify other pathology in the event a PE is not the cause of the symptoms.”
The fourth time the D-dimer was positive, my mother was deemed unsuitable for the CT scan due to mild kidney dysfunction, so she was advised to have a “VQ” scan of her lungs.
Chest pain and difficulty breathing can have many causes.
My mother’s fourth D-dimer test was ordered because she complained of trouble breathing (which later was determined by a pulmonologist to be from panic attacks).
 Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University,
Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University,
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image source: vecteezy.com
Source:
sciencedaily.com/releases/2014/03/140318162919.htm
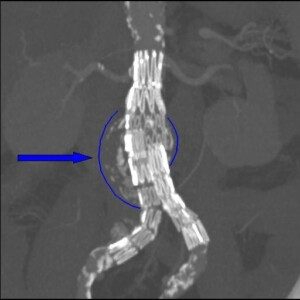
How Often Should a Small Abdominal Aortic Aneurysm Be Followed?
Your doctor will want your small abdominal aortic aneurysm to be followed with a watchful-waiting approach: serial imaging to see if the bulge is getting bigger.
This means imaging at fixed intervals to track any increase in size of the vessel dilation.
But how often should this occur? This depends on the size of the bulge and its growth rate over time.
The smallest abdominal aortic aneurysms often do not get significantly bigger over a course of many years.
But this doesn’t mean a small AAA shouldn’t be imaged with regular intervals of time in between.
Serial imaging is crucial. The survival rate of an abdominal aortic aneurysm rupture is about 20 percent.
Risk Factors
- Smoking
- High blood pressure
- Family history
- Being male and over 70
- Women are by no means immune to an abdomincal aortic aneurysm, and a large study showed that for women, high blood pressure was the leading risk factor,
Though most of these bulges grow at a slow rate, the rate varies from one patient to the next.
Though there’s no one-size-fits-all standard for time intervals between surveillance, there are general guidelines.
Time Intervals for Following an Abdominal Aortic Aneurysm
“Abdominal aortic aneurysms (AAA), defined as ≥ 1.5x the patient’s normal abdominal aortic diameter, should begin to be followed once they have reached 2.5 cm in diameter,” says Brett Mollard, MD, a board certified diagnostic radiologist who specializes in abdominal imaging and nuclear medicine.
“Recommended follow-up frequency is dependent on aneurysm size, with larger aneurysms requiring more frequent follow-up, as they typically have faster rates of growth and higher rates of rupture compared to smaller aneurysms.
“For example, aneurysms in the 2.5-2.9 cm range should be followed at either five year (Journal of the American College of Radiology) or 10 year intervals (The Society for Vascular Surgery); while aneurysms in the 4.0-4.4 cm range should be followed in one year intervals; and aneurysms greater than 5.5 cm in diameter or rapidly enlarging (≥ 5 mm in six months) should typically be treated.”
Conclusions
Cost effectiveness of following an abdominal aortic aneurysm needs to be assessed, as well as different types of surveillance policies.
Reducing imaging frequency would cut surveillance costs, yet also increase patient anxiety and rupture rates. In turn, costs related to emergency surgery would rise.
 Brett Mollard, MD, completed his residency in diagnostic radiology and nuclear medicine at the University of Michigan where he served as Chief Resident. He subsequently completed a fellowship in abdominal imaging at the University of California, San Francisco (UCSF). He currently works in private practice.
Brett Mollard, MD, completed his residency in diagnostic radiology and nuclear medicine at the University of Michigan where he served as Chief Resident. He subsequently completed a fellowship in abdominal imaging at the University of California, San Francisco (UCSF). He currently works in private practice.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus
Source: jamanetwork.com/journals/jama/fullarticle/1656254
Endovascular Aneurysm Repair vs. Open Surgery Survival Rates
How much better is the survival rate of an endovascular repair of an abdominal aortic aneurysm when compared to open surgery?
An endovascular repair of an AAA isn’t as complicated when compared to the more invasive, open surgical treatment.
On the other hand, stented grafts can fail, and this procedure requires lifelong CT scans (radiation) for monitoring.
A Johns Hopkins professor has determined that the four-year survival rate between both repair procedures for abdominal aortic aneurysms is similar.
This means that elderly patients, who might have been considered too frail to undergo the invasive open repair, didn’t fare better with the endovascular version – when four-year survival rate was considered.
This is very compelling information for an elderly person who’s afraid to have the open procedure.
No Survival Rate Advantage
For patients over age 70, this study showed that the minimally invasive endovascular grafting did not result in a higher survival rate.
Study leader Julie A. Freischlag, MD, points out in the paper that it’s questionable that very old patients should have any repair to their abdominal aortic aneurysm.
The repairs did not prolong life because these elderly patients were “dying of the diseases of old age,” states the paper.
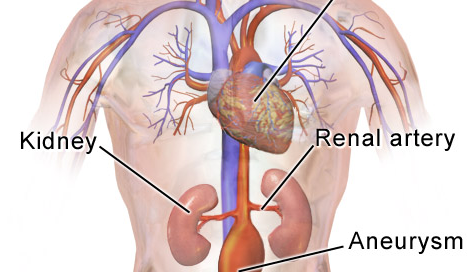
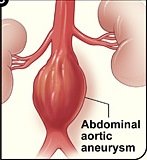
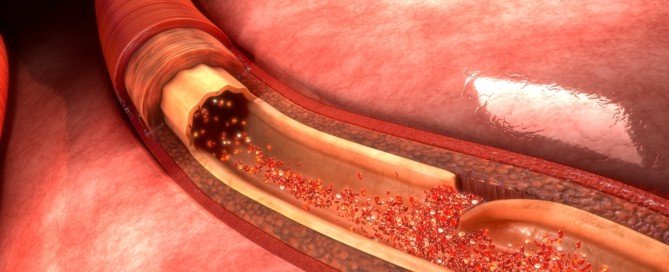
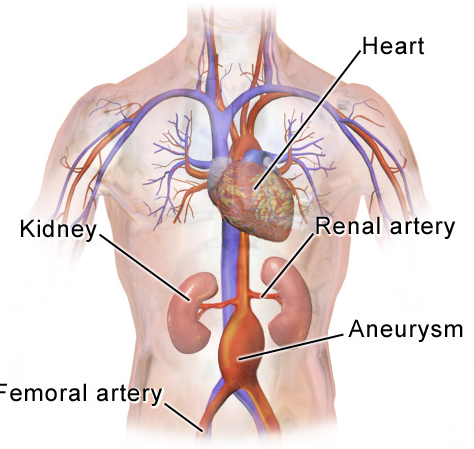
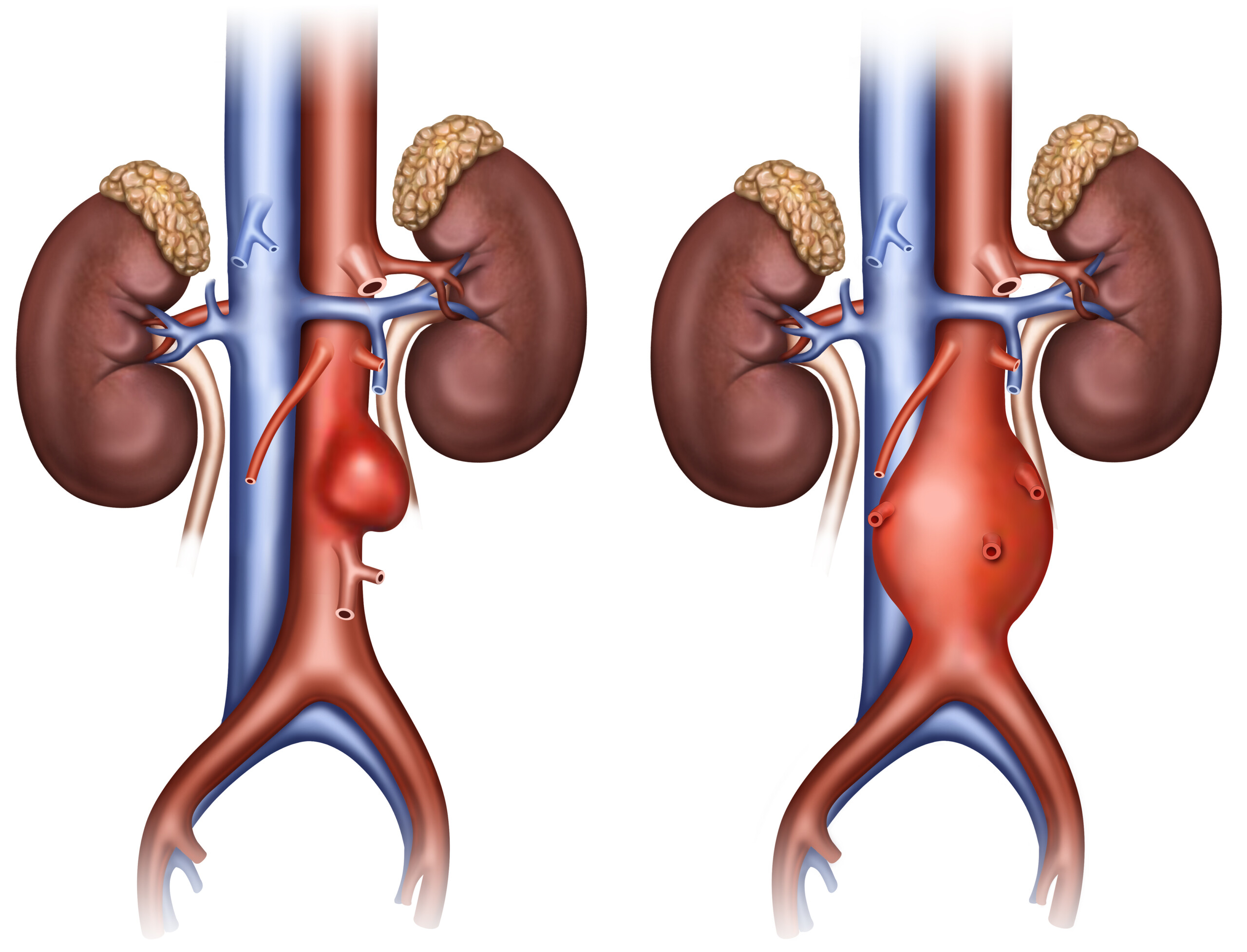
What is an abdominal aortic aneurysm?
An aneurysm is when a portion of a blood vessel wall becomes weak, causing it to swell, dilate or “balloon.”
Think of a balloon filling with air; as it enlarges, its “walls” become thinner and more prone to rupturing.
An AAA can rupture if it gets big enough, causing fatal internal bleeding. They typically cause no symptoms.
People usually learn they have an AAA when it’s accidentally discovered upon imaging for an unrelated concern.
The Johns Hopkins study concluded in 2012, which means that consideration of survival rates for open surgery vs. endovascular repair may be outdated, as advances in repair techniques are always underway.
So as of 2019, I asked Michael Fiocco, MD, about this.
“EVAR has a lower mortality rate than open surgery at 30 days — but the mortality rates converge at three to four years, due to the need for additional procedures, graft migration and potential aneurysm rupture due to migration in the EVAR group,” explains Dr. Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
This may make you wonder if younger patients, who in general are in better shape than those over 70, might be better candidates for open surgery.
“Younger healthier patients may be better served with open repair, but many factors are involved,” says Dr. Fiocco.
“Youth may not always convey health, and anatomy is just as important. If the aneurysm extends above the renal arteries, or down into the iliac arteries, this can be very challenging to overcome with EVAR, although techniques and equipment continue to improve.”
For endovascular repair the patient must have the appropriate anatomy to “land” the graft.
Stent graft on an abdominal aortic aneurysm. Dr Haudebourg, Public domain, via Wikimedia Commons
As mentioned previously, EVAR requires lifelong CT monitoring — every six months — to check for graft shifting (migration).
An intriguing detail in the Johns Hopkins study, which involved 881 patients with an average age of 70, is that the only post-repair aneurysm ruptures occurred in the endovascular group who did not get their regular CT scan follow-ups.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: hopkinsmedicine.org/news/media/releases/long_term_survival_rates_after_less_invasive_repair_of_abdominal_aneurysm_the_same_as_with_open_procedure
Best Time to Have Aortic Dissection Surgical Repair

An aortic dissection can kill you in two minutes; certainly there has to be a best time to suffer this life-threatening rupture of the heart’s great vessel.
Unfortunately, you don’t get to decide when an aortic aneurysm starts rupturing.
A study has linked specific time periods with increased survival rates following repair of aortic dissection, and with reduced hospital stays following the procedure.
A report in the online Interactive Cardiovascular and Thoracic Surgery states that when repair of an acute aortic dissection was performed during the period of a waning full moon, odds of death were reduced.
When the surgery was performed during a full moon, hospital stay was reduced. The study was done at Rhode Island Hospital and the paper published in 2013.
“We focused the study on patients having aortic dissection,” says Frank Sellke, MD, senior author, in the paper, “and found that the odds of dying following this procedure were greatly reduced during the waning full moon.”
Two groups of patients were studied:
1) Patients undergoing repair of an ascending aortic dissection, and
2) Those having an aortic dissection plus either coronary bypass surgery, aortic valve surgery or both.
When the repair of an aortic dissection was done during the full moon phase, patients had a substantially shorter hospital stay when compared to the other two moon phases.
This comes down to full moon cycle (10 days) vs. other moon phases (14 days).
What does the moon have to do with aortic dissection repair outcome?
Aortic dissection. Shutterstock/sciencepics
“Although this study was small, it showed clear advantage to those operated on during the full moon,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Is the moon affecting the patient? The surgeon?
No one really knows, but I don’t discount any of these reports.
“There have been for years doctors who swear that the ER is always busier during the full moon; all the crazies come out during the full moon, etc.
“Unfortunately, dissection of the ascending aorta has a mortality of 85-90% within the first 24 hours of diagnosis if left untreated, so you are stuck having surgery during whatever moon phase you are in at diagnosis.”
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources:
mayoclinic.com/health/aortic-dissection/DS00605
sciencedaily.com/releases/2013/07/130715141816.htm

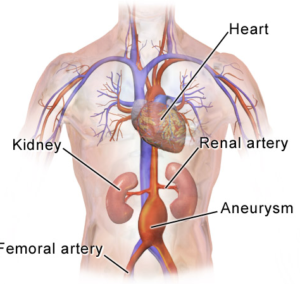
Abdominal Aortic Aneurysm Near Renal Artery: Endovascular Repair
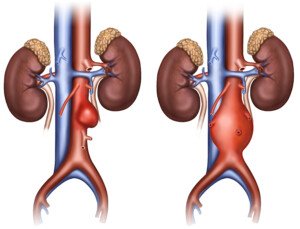
Innovative technology makes endovascular repair possible for an abdominal aortic aneurysm when it’s close to the renal arteries.
Have you been told you can’t have endovascular repair of your abdominal aortic aneurysm because the defect is too close to the renal arteries, and that your only option is the invasive, open surgery?
There’s been a breakthrough in stent-graft “landing,” in that now, the stent-graft can be customized to accommodate the patient’s anatomy.
The projection is that this will eliminate a lot of open surgeries, allowing these patients to undergo endovascular repair of their abdominal aortic aneurysm.
One of the first U.S. hospitals to provide this new technology is Johns Hopkins Hospital.
Historically, the open surgery has been performed in some patients because endovascular repair is not possible; the stent-graft would get in the way of the renal arteries because the abdominal aortic aneurysm is located too close to these vessels.
In stent-grafting (which is done by feeding a catheter through the groin to the abdominal aorta), room on either end of the graft is required to “land” it. This room isn’t there if the aneurysm is close to the renal arteries.
Though the open surgery is cheaper, it’s also much riskier (e.g., higher risk of kidney failure or heart attack) and can require up to eight weeks for recovery.
Prior to this new technology, the grafts used for endovascular repair were pulled off the shelves; not tailor-made for the patient.
“We need at least 5 millimeters to 10 millimeters of length between the renal arteries and the aneurysm in order to secure the stent-graft in place in most patients,” says surgeon James Black, in the report, from Johns Hopkins.
Dr. Black is one of only a few dozen surgeons in the U.S. who’ve been trained to make endovascular repairs of abdominal aortic aneurysms with this new graft technology, which was FDA-approved in April of 2012.
Traditional endovascular grafts are made of polyester fabric that’s encased in a stainless steel scaffold.
The newest development is similar, except that it has fenestrations: two little holes or openings fabricated into the graft, allowing accommodation of the renal arteries. These tiny holes help keep the device in place.
The graft must be “engineered correctly to match the patient’s individual anatomy,” explains Dr. Black.
Pre-surgical planning includes using a CT scan to create a 3-D image and model of a patient’s aorta. The construction of these grafts takes around five weeks.
Dr. Black says that every year, Johns Hopkins performs about 100 open surgeries for abdominal aortic aneurysms in patients who do not qualify (due to location of their aneurysm) for the minimally invasive endovascular repair.
But with the new fenestrated device, says Dr. Black, “We will be able to spare many of those patients a big operation and a long recovery.”
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/ilusmedical
Source: hopkinsmedicine.org/news/media/releases/customized_device_tailored_to_patients_individual_anatomy_now_used_to_repair_abdominal_aortic_aneurysm_without_surgery__
Why Is Melanoma So Hard to Treat?
All advanced cancers are difficult to treat, but one of the most difficult metastases to manage is melanoma skin cancer.
Melanoma is one of the most difficult cancers to treat. However, researchers are closing in on this mystery.
The news is from UC Irvine’s Chao Family Comprehensive Cancer Center; researchers there have figured out a major reason why melanoma is so resistant to chemotherapy treatment and thus exceptionally hard to treat.
While melanoma is highly curable when caught early, says Mayoclinic.com, this cancer yields a very poor prognosis once it spreads, because historically, it evades chemotherapy so well.
The American Cancer Society says that once this disease spreads, the five-year survival rate is 15-20 percent.
Why is melanoma so hard to treat?

Laurence Meyer, MD. cancer.gov
There is a genetic pathway in this cancer that inhibits a cellular mechanism.
This cellular mechanism’s job is to detect damage to DNA. This DNA damage is caused by chemotherapy.
When the cellular mechanism fails, the melanoma cells build up a resistance or tolerance to chemotherapy — which is supposed to kill cancer cells. The researchers targeted this pathway.
The pathway consists of the genes RhoJ and Pak1. UCI dermatologist Dr. Anand Ganesan aims to figure out a way to shut off this pathway.
Dr. Ganesan explains that if the pathway is turned off, “melanoma tumors would suddenly become sensitive to therapies we’ve been using for the last 20 years.”
What exactly is RhoJ and why does this make melanoma so difficult to treat?
It’s a gene that’s involved in the growth of blood vessels. Dr. Ganesan’s team noted that RhoJ does something peculiar when a cancer cell gets hit with chemo drugs.
The gene activates Pak1, another gene. In the study, Pak1 then triggered a molecular chain reaction that suppressed the melanoma cell’s ability to “feel” the damage from the chemo drug.
Think of it this way: The cancer cell gets spanked, but can’t feel the spanking, so the spanking (chemotherapy) does no good. The objective is for the chemo drugs to cause melanoma cancer cells to commit suicide.
Well, they don’t because they don’t sense the drugs’ effect, and as a result, the melanoma cells run amok.
“Being capable of rapid adaptation and change is a hallmark feature of this challenging form of cancer and makes it very difficult to treat,” says Dr. Ganesan.
The team has discovered the why, but has not figured out how to make the spankings hurt (i.e., shut off RhoJ).
However, identifying the “why” is the first step in making melanoma easier to treat.
The researchers are now investigating methods that will suppress these wayward genes so that the cancer cells can sense the DNA damage from chemo.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources:
sciencedaily.com/releases/2012/09/120917132351.htm
mayoclinic.com/health/DiseasesIndex/DiseasesIndex

Is There a Way to Detect Melanoma Extremely Early?

There IS a way to detect and diagnose melanoma when it’s in a very early stage — and hence, highly curable with an excellent 10-year survival rate.
Just how early can melanoma be detected? First of all, some exciting news:
The chief reason why melanoma cells are so resistant to chemo has been discovered by researchers at UC Irvine’s Chao Family Comprehensive Cancer Center.
However, researchers are a long way off from applying this discovery to melanoma treatment. This is why very early detection of melanoma is crucial.
Those who fear this skin cancer and/or are at elevated risk need to know about a technology called serial digital dermoscopy.
Malignant lesions can be missed by the layperson during monthly skin checks and even by a dermatologist, simply because the naked eye cannot always detect changes.
“Monitoring your moles for change or irregular features is one of the best ways to detect melanoma skin cancer early,” says Adam J. Mamelak, MD, a board certified dermatologist and founder of Sanova Dermatology in Austin, TX.
“In the doctor’s office, dermatologists often use handheld microscopes called dermatoscopes to evaluate the features and patterns of a mole or pigmented lesion on the skin.
“Just like the A, B, C, D, E features of atypical moles that we look for with the naked eye, there are a number of characteristics that we look at with the dermatoscope to determine if a spot on the skin is benign or malignant.
“Newer dermatoscopes allow you to connect a phone or camera to the magnifying lens and take pictures of the dermatoscopic image.
“Just as we look for changes in a mole with the naked eye, serial dermatoscopic images can be compared to make sure no irregular features are visible or become visible over time.
“DIgital dermoscopy, just like high resolution digital photography, has become a useful tool in the dermatology clinic.”

Serial digital dermoscopy
A dermatologist will examine your skin and then select the moles for the serial dermoscopy.
In my case, I requested that the moles on my back — even though typical — get imaged since I can’t easily inspect them.
Selected moles were indicated with a marker so that the nurse knew which ones to image.
Soon after, the dermatologist sat with me at the computer and reviewed the magnified images.
Serial digital dermoscopy involves comparing the images to a database of images of normal and melanoma moles.
Some computer systems will rate the images according to a color spectrum.
Other computer systems don’t do any rating, and instead, dermatologists use their naked eye to inspect the blown-up images on the computer screen for any signs of abnormalities.
When melanoma is caught very early, the 10-year survival rate is 99 percent.
 Dr. Mamelak
Dr. Mamelak
































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}