

Cause & Treatment of Small Itching Blisters on Your Fingers

Are small and itching “blisters” on your fingers driving you mad?
If you see “blisters” on your fingers and they itch, these may not be the typical blisters that result from a burn.
“Itchy small blisters on the fingers are often simply a condition called dyshidrotic eczema, a form of dry or irritated skin,” says Dr. Joel Schlessinger, MD, board certified dermatologist and cosmetic surgeon with a private practice in Omaha, NE.
“It is important not to pick at them or open them up, as that can result in more issues and prolonged irritation,” says Dr. Schlessinger.
“Instead, try to moisturize them or use a topical steroid if available such as 1% hydrocortisone.
“This can result in improvement, but if there is a continued irritant such as handwashing, detergents or a contact allergy to rings or clothes, these will have to be avoided to allow the area to improve.
“Many times I am asked what the ‘water’ or ‘fluid’ is inside of the blisters.
“This is only serum (a form of infection or trauma-fighting fluid) that is sent to heal the area.
“Opening up the area or washing it away delays healing, so it is best to avoid unroofing the blisters.”
And no matter how much they itch, do not scratch them.
Otherwise, the scratching breaks the skin, increasing infection risk and worsening the inflammation.
It can spread the rash, delay healing and lead to painful cracks or scarring.
More About Dyshidrotic Eczema
- Though it can affect children, it typically appears in people 20 to 40.
- Risk factors include family history and a personal history of contact dermatitis and hay fever.
Triggers of this itchy blister condition, which can also include flaking, are:
- Mental stress
- Pollen
- Excessive sweating of the hands
- Contact with the following items due to their nickel content: keys, cell phones, jewelry, metal buckles and buttons, zippers and eyeglass frames.
- Consumption of the following foods due to their nickel content: chocolate, almonds, oatmeal, soybeans and canned goods.
 Dr. Schlessinger, founder of LovelySkin.com, has 25+ years of experience treating many skin conditions including melanoma. He’s founder of the Advanced Skin Research Center, a clinical facility that investigates new medications and treatments.
Dr. Schlessinger, founder of LovelySkin.com, has 25+ years of experience treating many skin conditions including melanoma. He’s founder of the Advanced Skin Research Center, a clinical facility that investigates new medications and treatments.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Maslesha,CC BY-SA

Causes of Excessive Sweating on Face, Neck, Head

A dermatologist explains what might cause excessive sweating on your face, neck and head that doesn’t correspond to any intense physical activity or heat.
“Excessive sweating is usually caused by a certain type of nerve on the sweat glands that leads to sweating out of proportion to what is necessary to maintain our regular temperature,” says Dr. Joel Schlessinger, MD, board certified dermatologist and cosmetic surgeon with a private practice in Omaha, NE.
“Some sweating is absolutely necessary but there is a point where it becomes too much!
“Generally, this happens on areas such as arms, hands and feet (and underarms, of course), but some individuals have it all over,” including the face, neck and head.
Dr. Schlessinger adds, “This is a different type of sweating that can be caused by the same unregulated nerves, or other conditions such as menopause, obesity, diabetes, pregnancy, high thyroid levels, Parkinson’s disease, lymphoma, gout and various infections.
“If these are concerns or if you have uncontrolled sweating it may be a good idea to see your physician.
“The most common form that I see is when it is associated with menopause.”
When an woman has menopausal hot flashes, she can have excessive sweating on her face, head and neck, but usually, the flash of sweating will occur elsewhere as well, rather than only on the face, head and neck.
Also, says Dr. Schlessinger, menopausal sweating disappears shortly after the hot flash begins.
“Hyperthyroidism is also commonly associated with sweating,” he says, and a blood test can check for this condition.
Dr. Schlessinger, founder of LovelySkin.com, has 25+ years of experience treating many skin conditions including melanoma. He’s founder of the Advanced Skin Research Center, a clinical facility that investigates new medications and treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Burning in Stomach after Gallbladder Surgery: Doctor Explains

There are MANY causes, says a gallbladder surgeon, of stomach burning after the surgery, and thus, many treatment approaches.
Sometimes, a person who had gallbladder removal surgery reports a burning in the stomach.
This has many causes and is called post-cholecystectomy syndrome.
“Post-cholecystectomy syndrome (PCS) is a complex of heterogeneous symptoms including persistent abdominal pain and dyspepsia (burning sensation) that recur and persist after cholecystectomy,” explains Akram Alashari, MD, a trauma surgeon at Geisinger Medical Center in PA, and author of “THE POWER OF PEAK STATE.”
“PCS is defined as ‘early’ if it occurs in the postoperative period and ‘late’ if it occurs months or years after surgery.”
What causes the burning in the stomach?
“The symptoms of pain and dyspepsia referred to as PCS can be caused by a wide spectrum of conditions, both biliary and extra-biliary.
“About half of the patients with PCS are found to have biliary, pancreatic or gastrointestinal disorders, while the remaining patients have extra-intestinal disease.”
The term extra refers to beyond the intestines, or beyond the bile ducts for “extra-biliary.”
Dr. Alashari says that the biliary causes of PCS include:
Biliary injury, retained cystic duct or common bile duct stones.
“Late PCS can be due to recurrent common bile duct stones, bile duct strictures, an inflamed cystic duct or gallbladder remnant, papillary stenosis or biliary dyskinesia.
“Biliary dyskinesia refers to motor forms of sphincter of Oddi dysfunction. Sphincter of Oddi dysfunction can be evaluated with sphincter of Oddi manometry.”
Dr. Alashari names the following causes for extra-biliary PCS:
Irritable bowel syndrome, pancreatitis, pancreatic tumors, pancreas divisum, hepatitis, peptic ulcer disease, mesenteric ischemia, diverticulitis or esophageal diseases.
Extra-intestinal causes, says Dr. Alashari, are: intercostal neuritis, wound neuroma, coronary artery disease or psychosomatic disorders.
Treating Stomach Burning after Gallbladder Surgery
Dr. Alashari explains, “Treatment for PCS is tailored to the specific cause of the symptoms.
“Diagnosis of the underlying problem causing PCS usually requires imaging to look for retained or recurrent stones or identify a bile duct leak, stricture or transection.
“This can be accomplished in most cases with ultrasound and/or computed tomography (CT) scanning followed by direct cholangiography or magnetic resonance cholangiopancreatography (MRCP).
“MRCP provides a noninvasive alternative to direct cholangiography for evaluation of the biliary tract.”

Dr. Alashari was formerly with Grand Strand Regional Medical Center in SC as an abdominal and critical care surgeon.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/sebra

Prevent Gallbladder Attacks with Five Food Types

A gallbladder disease expert recommends five foods in particular that will help prevent gallbladder attacks.
“There is often a history of fatty food ingestion one hour or more before the initial onset of pain,” begins Akram Alashari, MD, a trauma surgeon at Geisinger Medical Center in PA, and author of “THE POWER OF PEAK STATE.”
“The episode of pain is typically prolonged (greater than four to six hours).”
Five Dietary Changes (Foods) that Can Help Prevent a Gallbladder Attack
Dr. Alashari explains, “The observation that deficiency of ascorbic acid (vitamin C) is associated with the development of gallstones in guinea pigs prompted investigation of the relationship between ascorbic acid levels and gallstones in humans.
“The benefit of ascorbic acid may be related to its effects on cholesterol catabolism.”
#1. Right away you may be thinking whole oranges, but the following fruits have higher vitamin C levels: raw acerola juice (1,600 mg per 100 g serving), raw guava, orange juice, grapefruit juice and raw kiwi. Green and red peppers are loaded with vitamin C.
#2. Dr. Alashari explains, Coffee; moderate coffee consumption was associated with a reduced risk of symptomatic gallstone disease in a cohort study involving 46,000 male health professionals who were followed for up to 10 years.
“Subjects who consistently drank two to three cups of regular coffee per day were approximately 40 percent less likely to develop symptomatic gallstones during follow-up.
“The benefit was even greater in those who drank four or more cups per day (relative risk 0.55). In contrast, decaffeinated coffee was not protective.
“A similar benefit from regular coffee was noted in a cohort study involving 81,000 women.”
#3 and #4. Dr. Alashari says, “Vegetable protein and nuts. The Nurses’ Health Study identified increased consumption of vegetable protein in the context of an energy-balanced diet as a protective factor for cholecystectomy.
“Comparing the highest with the lowest quintiles of intake, the risk was reduced by about 20 percent (relative risk 0.79, 95% CI 0.71 to 0.88), with a significant dose-response relationship.
“There has also been an association of reduced risk of gallstone disease in men associated with the daily consumption of nuts.”
Examples of high protein plant foods besides nuts:
Green peas, quinoa and beans.
#5. Dr. Alashari says to help prevent gallbladder attacks, eat more foods with poly- and monounsaturated fats.
He points out that these beneficial fats “inhibit cholesterol gallstone formation in animals.
Whether diets rich in these fats reduce the risk of gallstone disease was evaluated in the Health Professionals Follow-up Study, a large cohort study of male health professionals begun in 1986.
“After 14 years of follow-up, the relative risk in those in the highest compared with the lowest quintile of polyunsaturated and monounsaturated fat consumption were 0.84 (95% CI 0.73-0.96) and 0.83 (95% CI 0.70-1.00), respectively.
“This suggests that a high intake of polyunsaturated and monounsaturated fats in the context of an energy-balanced diet is associated with a reduced risk of gallstone disease in men.”
To help avoid gallbladder attacks, eat such foods as salmon, albacore tuna, cod and halibut, and olive oil and avocados.
Dr. Alashari was formerly with Grand Strand Regional Medical Center in SC as an abdominal and critical care surgeon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/KDdesignphoto

Advantages to Having A-Cup Breasts

I have very small breasts (A-cup) and never wanted them to be bigger.
An A-cup bra is actually a tad too big for me; my breasts do not quite fill out the cups, and the cups end up having some crinkles in them because my breasts aren’t big enough to expand out the fabric.
If I go braless, you can’t tell. Breast augmentation is one of the most popular cosmetic surgeries; and the women having this surgery don’t necessarily have A-cup breasts; many are B-cup and want to go to C-cup.
There are many advantages to having small breasts. It’s too bad there are women who are obsessed with getting bigger breasts, who cry every day because their breasts are “too small,” and who are bitter and depressed because they can’t wear low-cut outfits.
When I see a nice top and then see that it’s low cut, instead of hating my breasts for this, I instead curse the manufacturer.
Advantages to Having A-Cup Breasts
#1 Concealment of Double Mastectomy
If you ever have this disease and must have a double mastectomy, nobody will ever suspect you had this terrible illness if you’re small enough (unless there are other tell-tale signs such as suddenly wearing a wig due to chemo).
But many mastectomies are done electively to prevent recurrence or the cancer from developing in the non-cancerous breast.
I can’t imagine the emotional hardship it would be to have to explain to people what happened to your breasts.
With small breasts, the only person who’d know you had the double mastectomy would be your lover, but family members, close friends and co-workers would never, ever know, and you’d be spared the dread of having to tell people you had a life-threatening disease.
#2 Breast Self-Exams
A self-exam is so much easier when the area you’re examining is small.
#3 Minimal Sagging
Small breasts can only sag so much with old age. Their “saggability” is severely limited. When I look at my sub-A-cup breasts, I can’t imagine where they could sag to. They are naturally firm and perky.
#4 Brains
My breasts will never be distracting to a man whom I’m discussing something monumental with.
In other words, I’d like to think that small-breasted women will be taken more seriously, from an intellectual standpoint.
I’m not saying that women who are “well-endowed” can’t be smart. It’s the men who are often the variable here.
Some men can be prone to paying more attention to big breasts than to the brainy woman who is speaking to him.
When I speak to a man, all his attention is focused on what’s coming out of my mouth, not my chest (hopefully).
#5 Sports
Small breasts will never impede athletic performance. I can’t imagine what a detriment the big bosom would be during competitive volleyball, with all the jumping at the net and lunging for the ball. Big breasts would flap around like mad unless tightly bound.
I also run and do jumping drills at the gym. I’ve taken karate and have been smacked in the chest with kicks. This would have more-so hurt with big breasts.
I have done rock-wall climbing. Climbing technique involves keeping the body as flat against the climbing surface as possible to minimize falling backwards.
Big breasts would get in the way. But small ones allowed me to press my body up super-close to the wall.
#6 Rape and Assault
Because I’m so “flat,” I can look quite tomboyish or masculine, depending on my attire. This less-than-classically-feminine appearance will make a man think twice before picking on such a woman.
Small breasts are associated with masculinity or with being a jock. If a man perceives a woman on the street as a jock type or masculine, he is less likely to tangle with her.
But at the same time, small breasts can allow a female to look like 100 percent woman, because instead of fretting about being “flat,” she could focus on her other attributes, such as shapely firm legs and shoulders. And her crowning glory: hair.
Not all men are “breast men.” Some men are “leg men.” Some go for the hair! Glowing skin and sultry eyes will often snag a man’s attention before anything else.
It’s not all about the mammary glands. If you have an A-cup, it’s time to embrace it!
Update: The author of this article eventually had an elective (prophylactic) double mastectomy after learning that her sister had breast cancer. And of course, nobody — not even family members — noticed.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ tugol

Can a CT Scan Detect Colon Cancer?

If you have colon cancer, would a CT scan show it?
“CT scans are adept at locating pathology IN the abdomen or outside of the bowel,” says Sander R. Binderow, MD, FACS, FASCRS, with Atlanta Colon & Rectal Surgery.
Dr. Binderow continues, “CT is very good for solid organ disease — liver, spleen, kidneys. It can show metastatic colon cancer that has spread to the liver.
“Colon cancer, however, starts inside of the bowel. CT is notoriously unreliable for polyps or early stage tumors. It can show large, more advanced cancers or masses.”
So for instance, my father went to the ER complaining of significant lower abdominal pain and a persistent feeling of constipation.
The doctor ordered a CT scan and at some point, she commented that it would be good news if the scan did not show an “obstruction,” as this could possibly be a malignant mass — having originated as colon cancer but having infiltrated outside of the colon where a CT scan would pick it up. (Turned out my father had diverticulitis.)
And even if a mass does indeed show up on a CT scan…this doesn’t mean it’s malignant.
Dr. Binderow explains, “If a CT is suspicious for a colorectal cancer, the next immediate step would be a colonoscopy — which again is the best test to evaluate the colon and find colon cancer.”

Colonoscopy
In the absence of a CT scan, if you’re just wondering about colon cancer and would like to get some initial screening for it, you may consider Cologuard, which is a non-invasive screening test for this disease.

Cologuard kit
Cologuard uses the latest advances in stool DNA technology — detecting the altered DNA from abnormal cells in a stool sample which could be associated with cancer or precancer.
Symptoms of Colon Cancer
Symptoms of this disease are as follows: After having a bowel movement, you feel as though the movement was incomplete and that there’s still more to void — but nothing more is eventually voided.
Unexplained constipation — struggling and straining to void, despite increased fiber and water intake and even the use of stool softeners.
Unexplained diarrhea is another sign. The diarrhea may alternate with the constipation.
Stools that are shaped like ribbons or pencils.
Blood in your feces. This can present as red or maroon stools, as well as tar-black stools.
Abdominal or back pain, or unexplained loss of body weight.
The above symptoms can also have benign causes such as irritable bowel syndrome (except for the blood) and Crohn’s disease.
Crohn’s disease can actually be detected by a CT scan, but remember, colon cancer cannot.
 Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She is also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Tyler Olson
Colon Cancer Diarrhea vs. IBS Diarrhea: Is There a Difference?
Hemorrhoid Blood vs. Colon Cancer Blood: Is There a Difference?

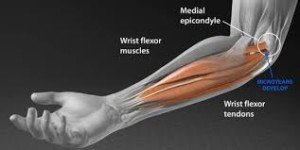
Cure Golfer’s Elbow with Two Simple Exercises

Here is how I cured stubborn golfer’s elbow: just two exercises.
I had golfer’s elbow for many months and months that didn’t respond well to rest, avoidance of offending activities or massage.
“Golfer’s elbow is layman’s terms for medial epicondylitis, which refers to pain and inflammation of the common flexor tendon of the forearm where it inserts on the inner portion of your elbow,” says Dr. Logan Thomas, a physical therapist in Parker City, IN.
I cured my golfer’s elbow with the following two exercises: the farmer’s walk and the deadlift.
My golfer’s elbow was such that if I deadlifted only 60 pounds, I could feel the aggravation in the tendon. So I started at 40 pounds—which felt “clean.”
I began farmer’s walks with just 10 pound dumbbells, because at 15 pounds, I kind of began “feeling it.”
The Deadlift
Before employing the deadlift for your therapy, make sure your form is PERFECT. Practice with a light bar or even a wooden pole.

The deadlift. Shutterstock/Vladimir Sukhachev
Once you know exactly what you’re doing, then find the amount of weight that enables you to do eight repetitions without feeling any hint of the golfer’s elbow—none of it even tapping on your door, so to speak.
Yet at the same time, this weight should be close to that threshold in which you would begin feeling the tendon problem tapping at your door. If you can “feel it” at all, reduce the amount of weight!
Do five sets, eight reps, with two minutes of rest in between.
And during the course of this therapy, you must avoid all offending activities, whether it’s golf, certain weightlifting exercises, certain household tasks, yardwork and what-have-you.
Do the deadlifting twice a week, with three days separating each session. Every few weeks, add 10 pounds.
If the golfer’s elbow taps at your door, back down on the weight load — go back to what you’ve been doing. Never increase by more than 10 pounds.
As you can see, at this rate, it will be a LONG time before you’re deadlifting 135 pounds. Do not let this discourage you.
When I had realized I had golfer’s elbow, I could not deadlift 60 pounds without “feeling” this damage.
However, as a result of sticking to this careful program that requires a lot of patience, I was eventually pulling 225 pounds for eight reps WITHOUT feeling any hint of the golfer’s elbow.
I’ll admit, it had seemed like forever that I was using a barbell of less than 95 pounds, but I’m sure glad I just stuck it all out.
I increased the rest time to three minutes once I got over 100 pounds.
Farmer’s Walks
Because 10 pounds in each hand is so light for this exercise, I did it nearly every day.
Once I got up to a 25 pound dumbbell in each hand, I reduced it to three times a week.

The farmer’s walk. Shutterstock/DisobeyArt
Simply walk for about two minutes. If you can “feel” the golfer’s elbow, use lighter weights.
Increase the dumbbell weight no more frequently than once a week, and do so with two and a half pound increments.
I went from 10 to 12 to 15 to 17 to 20 to 22.5 to 25.
It took a long time to get up to 25, because — and I can’t say this enough — you must use a weight load that’s below the threshold, but close to it.
Eventually I was carrying a 70 pound dumbbell in each hand without feeling the slightest hint of the golfer’s elbow.
Ancillary Exercises for Curing Golfer’s Elbow
Don’t rely on just the deadlift and farmer’s walk once you begin feeling the injury really improving.
At some point, you’ll want to reintroduce other offending exercises, such as the lat pull-down and the seated cable row.
START LIGHT. If you’re deadlifting 135 for reps, don’t assume you can just jump into a 100 pound seated cable row or 135 pound lat pull-down.
The motions of these two new exercises involve a different pattern of muscle recruitment, and thus, even if you can deadlift 150, a lat pull-down of only 75 might aggravate your golfer’s elbow.
Do not use a wide grip on the lat pull-down. Use a medium overhand and underhand grip with the long bar, as well as using a V attachment.
Apply the same principle outlined earlier: Work below the threshold, and very, very gradually increase weight — and I mean gradually. Do eight reps, five sets, a few minutes in between sets.
For the cable row, use a V attachment and apply the same principle.
Be patient and your golfer’s elbow will likely be cured. If over time, there’s no improvement, then you’ll want to seek professional intervention.
 Dr. Thomas a physical therapist, and strength and conditioning coach who is passionate about patient education. He believes the most important and often overlooked step in the process to becoming pain-free is understanding the anatomy and biomechanics of your body.
Dr. Thomas a physical therapist, and strength and conditioning coach who is passionate about patient education. He believes the most important and often overlooked step in the process to becoming pain-free is understanding the anatomy and biomechanics of your body.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/wutzkohphoto
Can Microscopic Colitis Spontaneously Go Away?

If you’ve been diagnosed with microscopic colitis, you’re no doubt wondering if this inflammatory bowel condition can go away on its own, or spontaneously resolve.
After all, half of all cases of microscopic colitis present with sudden onset diarrhea; diarrhea is the hallmark symptom of this benign condition.
I was diagnosed with microscopic colitis some years ago, not long after a bout of sudden-onset, watery diarrhea that didn’t seem to want to go away.
Diagnosis of microscopic colitis is confirmed with a tissue sample of the large colon, obtained via colonoscopy, and then examined under a microscope, hence the name “microscopic colitis.”
My gastroenterologist told me that the condition would “resolve on its own in a few weeks.”
Less than three weeks after the diarrhea and changed stool appearance began, I started noticing that my stools began looking less abnormal, and that the diarrhea was less frequent. I attributed this to consumption of a probiotic, kefir.
I also speculated that I had had the microscopic colitis for quite a while and never knew it (this is possible, as the symptoms of a very mild case can be masked by a high fiber diet, since a high fiber diet can cause near-daily and even daily bouts of diarrhea, and I had had a high fiber diet).
However, enormous anxiety, triggered over the diagnosis of a brain tumor in my parents’ beloved dog, was the suspect in what triggered the flare-up of the pre-existing, low-grade microscopic colitis — if that’s indeed what I had had all along.
I just can’t believe this was a coincidence; the anxiety and stress (I loved that dog!) was horrendous.
This included battles with my mother and brother over how to properly feed the dog during his alternative treatment, and sleepless nights as I lie awake in my parents’ house, heart racing as I dreaded hearing the tell-tale sounds of yet another seizure.
(I was taking care of the dog because my parents, let’s just say, weren’t exactly a prime choice for this, which included frequent injections.)
My gastroenterologist’s nurse, prior to my colonoscopy, told me he had diarrhea for two weeks as a result of his divorce.
Diarrhea doesn’t necessarily mean microscopic colitis, and again, microscopic colitis must be confirmed via large-colon tissue biopsy.
In the few weeks following my colonoscopy (which was a few days after the dog was euthanized), my symptoms diminished and everything returned to normal.
And I kept drinking the probiotic. (I had moved back home a few days after the colonoscopy.)
However, I stopped drinking the probiotic when I moved into my parents’ home again to help take care of my father after his back surgery.
Seven days after his back surgery, I took my mother into the emergency room for shortness of breath and vomiting; she was discharged with a diagnosis of gastroesophageal reflux disease (GERD).
Two days later she was back with chest pain, and was admitted to the hospital because a blood test showed a slight elevation of the heart-attack marker troponin.
The next day she underwent a quintuple bypass surgery with mitral valve replacement after an angiogram showed extensive coronary blockage.
And if the stress from suddenly being told your mother will be undergoing a 7-hour surgery because a heart attack was imminent isn’t enough, then imagine the stress of what happens after coronary bypass surgery: the possibilities of complications and the arduous recovery process.
Did all this stress bring back my microscopic colitis?
I had one bout of diarrhea, but nothing else out of the ordinary. And I continued not drinking the probiotic.
The emotional stress was unspeakable, as there were bumps along the post-operative road, and my father’s back surgery didn’t seem to have resolved his problems.
Over the weeks following my mother’s coronary bypass surgery and all the stress it brought me, my microscopic colitis never recurred.
Seems as though the microscopic colitis spontaneously went away, so far away that even this new era of stress was not able to resurrect it.
So perhaps my doctor was right when he said that the microscopic colitis would “resolve on its own.”
However, many people with microscopic colitis who post in online forums report that the condition is ongoing, chronic, and for many patients, there is no truly effective treatment.
For some individuals, microscopic colitis is more than just an annoyance.
Episodes of diarrhea can be numerous throughout the day, immediately follow meals, and the condition can also be accompanied by abdominal cramps or pain.
So, can microscopic colitis go away on its own? Can it spontaneously resolve? In at least one case, yes. In other cases, it can be chronic.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

How to Cure Feeling Old from Menopause
There is ONE thing that women in menopause can do to cure the feeling of “getting old” as a result of this change in life.
Hey, I just don’t know how a woman can feel old due to menopause when she can step into a gym and deadlift 225 pounds for reps.
Now — that amount of weight may seem as far from you as the moon is, but I can say the same thing about deadlifting 135 pounds:
How can menopause make a woman who can deadlift 135 feel old?
The deadlift is one of the most effective strength training moves, regardless of one’s goal.
It’s fantastic for fat loss, shrinking the stomach, toning the legs and arms, strengthening the back, curing certain kinds of back pain, improving overall neuromuscular function and so much more.

Deadlift. Freepik.com

Freepik.com
So how does this relate to feeling old from menopause?
The thing about this multi-joint or compound exercise is that it enables you to lift a LOT of weight as you progress over time.
Not only that, but it does NOT require balancing or other movements that can put a self-conscious woman on edge — such as trying to steady oneself on a balance board or coordinate pushing dumbbells overhead while stepping onto a bench and sticking out the other leg.
The deadlift is as basic as can be. ANYONE CAN DO IT — barring those with spinal structural problems (ask your doctor about the deadlift if you’ve been diagnosed with spinal stenosis or some other vertebral issue).
It’s not like the pushup, in which women struggle and become discouraged, or the pull-up, where women rely on spotters to help them up and then feel defeated.
ANY WOMAN CAN DEADLIFT
But don’t let the simplicity of this exercise fool you. It’s one of the most effective exercises for crushing calories, improving fitness, strengthening the back and knees and improving the ability to do other exercises.
Because the deadlift involves simply that of picking a barbell off the floor and then straightening, then lowering it with control, the potential to pick up impressive amounts of weight is very real — even if menopause has you feeling downtrodden and “old.”
The ability to pick something very heavy off the floor simply contradicts that of feeling old — even if you’re suffering from other symptoms of menopause such as thinning hair, hot flashes and fat gain.
There’s just something magical about knowing you can hoist heavy objects off the floor that makes you feel YOUNG and VIBRANT, not old and haggard.
Deadlifting heavy amounts of weight has the startling ability to carry over to everyday tasks of daily living.
- Picking up and carrying babies, even heavier preschoolers, will no longer be tiring.
- Housework and yardwork will be a breeze.
- Helping someone move will no longer make you ache the next day. Nor will shoveling snow.
The best cure for feeling old from menopause is to become proficient with the deadlift.
Start out with a light bar and do not get discouraged if your wrists, forearms, legs or low back ache the next day.
Should you use gloves?
Don’t use gloves; they’ll cheat you of developing maximal grip strength. They’re a crutch and won’t allow your hands and forearms to achieve optimal strength for real-life situations.
MASTER CORRECT FORM FIRST.

Freepik.com
There are different ways to deadlift—too much information to go into for this article — but the bottom line is that you will find out what style works best for you.
However, it’s a universal phenomenon that the “mixed grip” makes handling the barbell more efficient for anybody, so you’ll want to get used to that:
One hand is an overhand grip, and the other is an underhand.
I’ll say it again: It’s impossible to feel old when you know you can lift heavy things off the floor.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Caregivers to Elderly: How to Lift Mother off the Floor

When I was a caregiver to my elderly mother, I was always easily lifting her 130-pound body off the floor.
Following quintuple bypass surgery, mitral valve replacement and a pacemaker implant, my mother developed a mysterious condition that disrupted her blood pressure and/or blood vessels (none of the doctors had an answer).
This condition caused her brain to gradually begin losing oxygen (blood flow) whenever she exited a chair (or bed) to be on her feet.
Within seconds to about two minutes, she’d begin passing out, but the passing out was gradual, rather than the sudden fainting that “drops” someone in an instant.
Because it was gradual, there was time for cognitive changes to manifest over the seconds to few minutes, stripping her of insight into what was happening.
This was combined with general non-compliance (refusing to alert me every time she exited a chair).
As a result, I couldn’t let her out of my sight or else she’d ultimately lose consciousness and fall—risking catastrophic head injury. I had to walk right behind her.
The gradual passing out was inevitable, and my mother, becoming increasingly disoriented and belligerent (from the oxygen deprivation to her brain), would eventually show signs of imminent loss of consciousness.
At this moment, I’d place my arms snug under her armpits, as I was always behind her during these incidents.
The junction of my upper and lower arms was up against her armpits. Feet about shoulder width apart, I’d then “sink” her butt to the floor (keeping my low back arched and dropping into a half squat).
At this point she was out of it, unable to contribute to the “sinking.”
Often, this bizarre malady caused her legs to stiffen, so instead of her legs bending as I “sunk” her, they remained rather straight and stiff as I placed her on her butt. If we were in crowded corners, this was tricky.
If you’re wondering why I didn’t just hold her upright till the spell passed, it’s because these slow-motion orthostatic hypotensive episodes were determined to run their course.
Had I held her upright, she would have completely lost consciousness, and I’d have to then sink her anyways. Why wait till complete loss of consciousness?
Sinking my mother to the floor had to be done gently and with control…the way a weightlifter controls the lowering of a barbell.

Shutterstock/Everyonephoto Studio
Once she was on the floor, she’d regain her wits, but was too weak to get up on her own. I had to lift her back up to her feet.
In case you’re wondering why I didn’t just sink her into a chair instead of the floor, this is because her mental state was too altered to respond to a directive to sit in a chair — her mental faculties were impeded.
Due to the stiff, unbending legs, getting her butt square into a chair was difficult.
I’d actually tried this initially, but had trouble aiming her butt into the nearest chair, so I decided, why not just sink her to the floor — wherever we were when one of these episodes occurred.
They occurred outdoors frequently when she got out of the car. I’d sink her on grass, cement and inside stores, then lift her back up.
As a caregiver, how did I easily lift my elderly mother from the floor?
She’d be sitting on the floor, back and head resting against my legs for some moments while the blood was restored to her brain.
But despite regaining her wits, she was too weak to get up, so I’d position my arms under her armpits and be in a position that resembled a fusion of the start of a deadlift motion (see photo above) and a half squat.
My legs and glutes powered me up, but so did my middle and lower back, though the lower back contributed only in terms of stabilizing my spine rather than force production.
I kept an arch in my lower back, making sure my back did not round, and simply straighted up, like performing a barbell “back” squat and deadlift hybrid.
Once my mother was on her feet, she could be up on them as long as she liked; the orthostatic hypotension would occur only one time after every time she rose from a seat.
I just described technique, but what about the strength to lift an elderly person from the floor without much effort?
I did this all day long and in the middle of the night, and once found myself straddling the toilet, my back facing the wall, my mother sitting on the seat in front of me, after she began passing out while on the seat (the result of exiting a chair to use the bathroom; I had followed her, anticipating the slow-motion passing out).
I never knew when I’d have to sink her and then lift her off the floor, but I was always physically prepared.
Effortless lifting of an elderly person off the floor will come to anyone who’s been training heavy with weights for a good amount of time.
Though 130 pounds doesn’t seem like much, this is entirely too heavy for most female caregivers, and even some men would struggle with this — possibly straining their back in the process and/or experiencing exhaustion.
I felt I could lift her off the floor even if she weighed 150, because my body had pre-existing training with the deadlift exercise.

Shutterstock/sportpoint
“The sumo deadlift [above] would be THE exercise I would recommend to caregivers to be prepared for situations that would require the possibility of getting someone off of the floor,” says Dr. Chris Hardy, DO, a former Navy physician and NSCA certified strength and conditioning specialist.
“The wide stance and body mechanics of this exercise make it the most applicable and valuable for this type of situation to allow effective and safe lifting of a person from the floor.”
An alternative is the standard stance, as depicted below.

Anastase Maragos/Unsplash
If you don’t train with weights and currently are not a caregiver to an elderly mother (or father), I urge you to take up the deadlift, back squat (or dumbbell squat) and leg press — so that if one day you do become a caregiver to an elderly parent, you’ll be ready.
Go heavy and hard once you master proper form.
Additional exercises that will prepare you to lift an elderly person off the floor include the bent-over dumbbell row (shown below).

Shutterstock/Catalin Petolea
If you’re currently a caregiver to an elderly parent and don’t train with weights or have been lifting only light weights, then start lifting heavy and take up the aforementioned exercises, particularly the deadlift.

Shutterstock/The Faces
Being an lot taller than the elderly parent, whom you’re a caregiver to and trying to lift off the floor, is not a pass on training with heavy weights.
Though being taller adds a degree of biomechanical assistance — it’s pretty much worthless if your “posterior chain” muscles are out of shape (middle and lower back, butt and hamstrings).
 Dr. Hardy merges his expertise in nutrition, strength and conditioning, and in clinical/preventive medicine into a comprehensive approach to treat chronic disease.
Dr. Hardy merges his expertise in nutrition, strength and conditioning, and in clinical/preventive medicine into a comprehensive approach to treat chronic disease.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}