
Is Laughing AT Children by Adults Harmful to Self-Esteem?

Ever notice how adults always laugh AT young children whenever the little kids are answering a question or explaining something?
Have you ever noticed that on any kind of talk show in which a child is being interviewed or asked questions, the audience laughs at the child’s response, or at the way they explain things?
This happens only when the youngster is under the age of 9 or so. I’ve never witnessed this phenomenon when the child appears to be older than 9.
Why do the adults in the audience laugh?
(I’ve also witnessed this phenomenon plenty of times in person, so I certainly don’t mean to imply it occurs only in live studio audiences.)
It’s one thing if the child is telling jokes and delivering punch lines as part of a comedy act, or obviously trying to elicit chuckles from listeners.
But this is not what I’m referring to.
The child is simply answering questions about a variety of topics, for whatever reason he or she is on the TV show for.
Why do adults feel a need or compulsion to laugh (and it often sounds “canned”) just because a young child is answering questions or explaining something?
- Yes, we all know that young children aren’t very articulate.
- Their vocal mannerisms and inflections can be quite quirky.
- Their voices may fluctuate among different tones and pitches.
- They may contort their faces and mouths while speaking.
But is this any reason to laugh at them?
Why is it so hard for adults to just sit tight and silently as young kids talk?
These same men and women wouldn’t dare laugh out loud AT another adult talking about the same topic!
Imagine what some 5-, 6-, or 7-year-old must feel like, hearing all this laughter erupt, after they explain something or answer some questions.
Might this reaction from adults make a little boy or girl feel inept, weird or like an oddball?
“The answer to this depends on several factors,” begins Stacy Kaiser, a southern California-based licensed psychotherapist and relationship expert with a special interest in the topic of bullying. They are as follows:
– The closeness of the relationship, if any, between child and adult
– Child’s maturity level and awareness of what’s taking place
– “Culture in the child’s family when it comes to humor,” says Kaiser
– Child’s self-esteem
– Intent behind the laughter
Kaiser explains, “Some children can be very perceptive and know what is underlying an adult’s laughter. The question is – is the child being laughed at or laughed with? If the child is able to determine the difference it could impact his or her self-esteem.”
This article, as already mentioned, deals specifically with laughing AT. Watch any talk show in which a boy or girl under age 9 is a guest.
But TV aside, you’ll see this phenomenon universally in any setting in which a young child is talking to adults — regardless of topic.
Again, I do NOT mean little kids deliberately hamming it up while wearing a crazy wig or while imitating a funny cartoon character.
I’m referring to when young kids are engaged in conversation with adults or answering questions.
I’ve witnessed hurt on the faces of ADULTS who are laughed AT by other adults.
I wonder if these same “hurt” adults laugh at little children who are merely answering a question or describing a situation.
Suppose adults engage you into conversation, and you quickly notice they are laughing AT you as you describe — without trying to be comical — your day or some event.
Chances are pretty high that the self-consciousness would begin kicking in.
If you already have a less-than-robust baseline of self-esteem, you’ll begin wondering what your shortcomings are in social situations that make people laugh AT you.
Other adults, with a stronger baseline, won’t give a hoot if listeners are laughing AT them.
And yet a third demographic will stop talking and snap, “What’s so funny?”
Adults who laugh AT children claim it’s because they’re cute, adorable and charming.
“No one likes to be laughed at,” says Kaiser.
“However, if a child has been raised in a family where people tease one another or laugh at one another, he or she is more likely to be able to withstand someone laughing at him.”
But if you laugh at kids you don’t know well, then you don’t know what kind of family structure they have, do you?
There are people who believe all of this laughing is perfectly okay; otherwise we’d be raising kids with weak backbones.
Ironically, it’s a fair bet that these very critics are often the first ones to become very defensive when someone gently criticizes them or even makes a little suggestion!
If you don’t want your child to grow up to be “weak,” then enroll them in martial arts, encourage them to speak their opinions (without swearing or yelling), and give them plenty of opportunities to figure things out for themselves and make choices (within age-appropriate parameters).
These three approaches are part of the recipe for becoming a very successful, self-confident, rock-solid adult.
“If a child is uncomfortable or self-conscious because they are being laughed at, it could impact their self-esteem, make them turn around and make fun of others, or make them withdraw and even isolate completely,” says Kaiser.
For those who believe it’s perfectly okay to laugh AT little kids, here’s a few questions:
- Why do you impose an age cut-off where you’d no longer do this?
- Is it because any child over the age of 9 can’t be adorable and cute?
Again, imagine you’re explaining something at a business meeting, and you begin hearing this chuckling and muffled laughter coming from several co-workers.
How would you feel? Imagine asking them why they were laughing at you, and they say it was because you were cute and charming. Would you buy this?
So why should a child be any better at processing being laughed at?

With over 100 TV appearances on major networks including CNN, NBC, CBS and ABC, Stacy Kaiser brings a unique mix of provocative insight to many topics such as anger management, office relationship issues and parenting.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Causes of Red Spots on Your Inner Thigh

Red spots on the inner thighs are annoying, whether you’re at the beach in a bikini or even at home lounging around by yourself.
There are four causes of red spots on the inner thighs that deserve some attention, says Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
Irritation of Hair Follicles — First Possible Cause
“If your thighs rub together, your red spots could be irritated hair follicles,” says Dr. Prystowsky.
Weight loss will help remedy this problem.
Here is the wrong way to trim “fat” inner thighs: inner thigh machine at the gym.
Please, don’t bother. When used correctly, this apparatus (also called seated hip adduction) will firm the muscles of the inner thigh.
But it will not shear off fat and thus, it will not alleviate the rubbing.
The only way to lean out the inner thighs is to lose overall body fat.
And the best way to do that is a combination of portion control, interval cardio and compound strength training.
Strength training exercises such as the deadlift (shown below), squat variations, overhead press with kettlebells, dumbbells or a barbell, the seated row and various chest press routines will trigger fat burning throughout your entire body.
This will include the excess fat between your thighs that causes them to make contact and lead to those red spots and irritated hair follicles (you may not necessarily be able to see actual hairs in that area).

Freepik..com
Molluscum Contagiosum
Dr. Prystowsky continues, “You can get rashes from molluscum contagiosum (a virus). A viral wart can look red.”
Molluscum contagiosum is caused by a viral spread through skin contact, shared objects or sexual contact, leading to small, painless bumps.
Insect Bites or Poison Ivy
Insect bites or poison ivy, says Dr. Prystowsky, are the next two possible causes of red spots on your inner thighs.
With insect bites, it’s not likely that there will be a peppering of red spots, but rather, just a few here and there.
The aforementioned four causes of red spots can also occur elsewhere.
For instance, hair follicle irritation can occur under the arms.
Red spots on the inner thigh have additional causes, such as angiomas — which can occur nearly anywhere, are harmless and don’t itch.
Here is a large list of possible causes (including cancer) of red spots, dots or specks on any part of your body.

In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/GBALLGIGGSPHOTO

Red, Itchy Bumps All Over Your Body Come from WHAT?

A dermatologist gives five possible causes of itchy red bumps all over your body…
Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience, describes five possible causes, in no particular order.
She explains, “Hives are an outbreak of pale, red, itchy bumps caused by an allergic reaction.
“Contact dermatitis, like the rash you get from poison ivy, occurs when you touch something that you are allergic to as well.”
It may prove to be challenging to figure out just what it is you’re allergic to, if this is the cause of your symptoms.
Dr. Prystowsky continues, “Erythema multiforme is an immune reaction to an infection, drug, or hormones.
“A form of cutaneous T cell lymphoma can cause red, itchy bumps. Widespread red itchy bumps would rarely signify cancer. However, in the case of cutaneous T cell lymphoma, this does represent cancer.”
Finally, bug bites can cause this symptom, but more likely than not, you’ll know if you’ve been bitten by bugs, such as during sitting outside in the evening, you have to keep swatting away mosquitos and feel them “biting” you.
Most Common Causes
“Most common causes of red bumps are allergy reactions to medications, plants or insects,” says Dr. Prystowsky.
In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/pathdoc
4 Causes of Black Spot on Lower Lip, Says Doctor

If that black spot on your lower lip is scaring you, a dermatologist explains four possible causes including cancer.
Keep in mind that what appears to be black may actually be a deep dark purple, or, if the speck is small enough, you may notice upon very close inspection that it’s actually medium brown.
The benign melanocytic macule can be medium brown, but so can the dangerous melanoma.
Dr. Janet Prystowsky is a board certified dermatologist in New York, NY, with 30+ years’ experience.
Dr. Prystowsky explains, “A black spot on the lower lip could be a freckle, a mole, a melanoma, or a blood vessel lesion such as a venous lake.”
Melanoma is the most serious form of skin cancer. Lips are part of the skin.
A “freckle” or “mole” that starts appearing on your lower (or upper) lip in later adulthood is more concerning than if it begins appearing if you’re under age 25, and especially under age 18.
“It is worth getting a professional’s opinion of the spot because a melanoma would be important to diagnose and treat,” says Dr. Prystowsky.
“Even though it is uncommon for a black spot on the lower lip to turn out to be melanoma, lip cancers metastasize more readily than other skin cancers.
“That means a melanoma on your lip has a much higher risk of causing death. An experienced dermatologic surgeon can do a lip biopsy without leaving you with a terrible mark/scar.”
Are there tell-tale signs of a black spot on your upper or lower lip that are more indicative of cancer (melanoma) vs. a benign lesion?
Dr. Prystowsky says, “Things to make you worry about having a melanoma on your lip include:
1) is it a new lesion?
2) has it been growing or changing in some way?
3) does it bleed readily? 4) does it have an irregular appearance or border?
4) is it large – over a few millimeters in diameter?
5) does it have multiple colors in it? i.e., white, blue, black, red.”
Scab on Lip that Won’t Go Away
This can be a type of cancer called squamous cell carcinoma. Though it may not look like a “black spot” in the true sense, it can still be dark and appear like a scab or tiny smudge, as shown below.

Squamous cell carcinoma cancer on the lip. Coronation Dental Specialty Group, CC BY-SA 4.0/creativecommons.org
What about this venous lake?
“For the lesions that are caused by a blood vessel, removal usually improves your appearance significantly,” says Dr. Prystowsky.
The venous lake is a benign cause of what appears to be a black spot on the lip.
If a dermatologist identifies the black speck as a freckle, be sure to keep an eye on it, says Dr. Prystowsky, in case it begins getting bigger, changing in size, shape, color or texture.
In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why Your Legs Keep Itching: 4 Reasons by a Doctor

Find out by a doctor why your legs are ALWAYS itching and driving you mad.
Having itchy legs can drive you up a wall, especially if you’re at a desk and need to get work done.
The itchiness and the scratching that comes with this situation is distracting and aggravating, to say the least.
Dr. Janet Prystowsky is a board certified dermatologist in New York, NY, with 30+ years’ experience.
She says there are four possible explanations for why your legs are itching all the time or frequently on a chronic basis.
“This is usually due to dry skin,” begins Dr. Prystowsky. “Our lower legs produce very little natural oil, so bathing with soap can strip that little bit of natural oil off, leading to dryness.
“This is usually the worst during the winter, when air has low humidity.
“Another cause for itching is if the lower legs/ankles are chronically swollen due to poor circulation,” says Dr. Prystowsky.
“This causes water to accumulate in the tissue, making the skin have to stretch to accommodate the increase in volume.
“It occurs in the lower legs, ankles and feet because gravity pulls excess tissue water down.
“The skin reacts by getting small cracks in the surface which leads to itching, redness, and scratching causes further damage, increasing the symptoms.
“If this is not addressed in a timely fashion, cellulitis, a soft tissue infection, may set in requiring antibiotics and sometimes a hospital admission.”
If you have poor circulation in your legs, there’s one of multiple causes; see your primary care physician for an initial assessment.
Poor circulation in your legs, also known as peripheral artery disease (PAD) or peripheral vascular disease, can result from narrowed or blocked blood vessels that restrict blood flow.
Symptoms may also include pain, cramping or heaviness in the legs during physical activity, which often improves with rest.
Other signs can include numbness, tingling or coldness in the legs, as well as sores or ulcers that heal slowly.
The tingling may also feel like itching.
Poor circulation can be caused by various factors, including atherosclerosis (buildup of plaque in the arteries), diabetes, high blood pressure and smoking.
Over time, reduced blood flow can lead to more serious complications such as infections or tissue damage.
Dr. Prystowsky continues, “Lower legs may also chronically itch because of a fungal infection.
“A fungal infection from your toenails can get on your foot skin and gradually creep up your leg.
“A proper diagnosis is required so that antifungal creams and/or pills may be prescribed.
“Flat warts may also lead to itching on a chronic basis, as they are hard to get rid of.”
In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Kittima05

Twinlab Omega-3 Cardio Krill Oil Review: Bad Fish Odor

Warning Review: Twinlab’s Omega-3 Cardio Krill Oil has a really bad fishy smell!
The fishy odor of Twinlab’s Omega-3 Cardio Krill Oil is REALLY BAD. I advise against buying this product because the capsules reek of old fish you might find in the trash. Even just opening the bottle releases the smell of garbage-can fish.
There is no excuse for this, because at least one other brand (NOW) carries a krill capsule supplement that’s odorless. Yes, odorless.
The reason I didn’t buy the NOW brand is because I can’t find it at any of the Whole Foods stores in the city, and I had run out of the supply I had bought online.
So I decided to go the cheaper and more convenient route when I spotted the Twinlab Omega-3 Cardio Krill Oil at a Sprouts store.

I figured, Okay, it’s right here in front of me, no hassle with online ordering. But boy, was I in for a very disappointing surprise when I opened the bottle and took out one of the very stinky capsules.
These krill capsules smell so bad that I threw out the bottle after taking about 15 of the capsules (one a day).
Shame on Twinlab for not using the technology that the NOW brand uses. I will be buying the NOW krill capsules from now on.
Do not buy Twinlab’s Omega-3 Cardio Krill Oil capsules unless you want a whiff of dead beached fish every time you take one of the capsules.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/pathdoc

Neurological Cause of Numb Toes when on the Elliptical Machine

Here’s a neurologist’s explanation for what causes numb toes when you use the elliptical machine.
What a nuisance: One or more toes go numb whenever you pedal on the elliptical machine at the gym.
The numbness may have tingling and persist for a while after you get off the machine.
If you suffer from health anxiety, you may be apt to wonder if this means multiple sclerosis.
“This is not very scientific, although several factors probably play a role,” begins Bonnie Gerecke, MD, director of the Neurology Center at Mercy in Baltimore.
“When on the elliptical machine, there is more pressure placed on the toes and forefoot compared to the hindfoot,” she continues.
“There are small digital nerves in the toes that are likely being compressed when the feet are on the pedals, and this in part causes the toes to go numb.”
This does not mean anything is wrong with your nerves or muscles.
The mechanics of this are akin to wearing a tight pair of high heeled shoes, cramming in your toes; your toes will probably go numb pretty quickly.
Dr. Gerecke continues, “There is also increased swelling in the feet during exercise, and this can also cause numbness. Tight fitting shoes are probably also contributory.”
How to Prevent Toes from Going Numb on the Elliptical Machine

Freepik
“One can wear slightly larger shoes than normal, although too much room could cause blistering,” says Dr. Gerecke.
“Pedaling backward intermittently for brief spurts can also help. Alternating with other exercises is also helpful.”
In addition, place your feet a bit away from the edge of the pedaling platform so that the toes don’t jam up against it when you pedal.
“While experiencing toe numbness while using the elliptical is common, if there is prolonged or severe numbness or tingling, one should seek the attention of a health care provider for an evaluation.”

Dr. Gerecke has a special interest in ALS, myasthenia gravis, myopathy/muscular dystrophy, peripheral neuropathy and radiculopathy. She is board certified in general neurology and neuromuscular medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com/jcomp

Stop Examining Your Tongue for Bulbar ALS

Here is why you have to STOP, once and for all, inspecting your tongue for bulbar-onset ALS. This destructive obsession has got to go.
Do you realize how rare bulbar-onset ALS actually is? It’s about 0.1 per 100,000 people. That’s one-tenth of one in 100,000.
But maybe that doesn’t matter to you, because you’re going by what you see in the mirror every time you examine your tongue—and this obsessive inspecting consumes a lot of your time…every day.
“Bulbar onset ALS is rare,” says Bonnie Gerecke, MD, director of the Neurology Center at Mercy in Baltimore.
“Moreover, patients who develop this condition experience dysarthria (slurred speech), dysphagia (trouble swallowing) and potentially other symptoms such as emotional lability, dyspnea (shortness of breath) and facial weakness.”
Some people who obsess about their tongue and ALS also begin believing they have slurred speech. They may hear or sense that they are slurring their words.
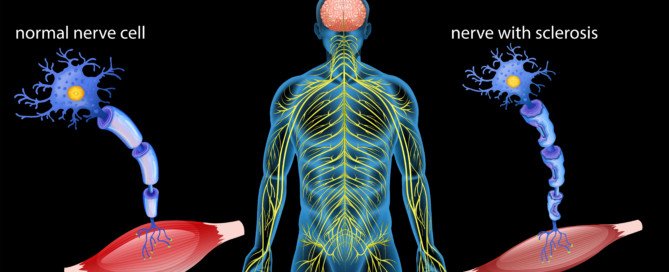
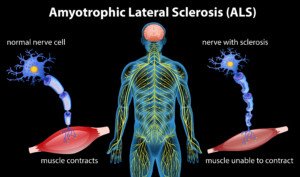
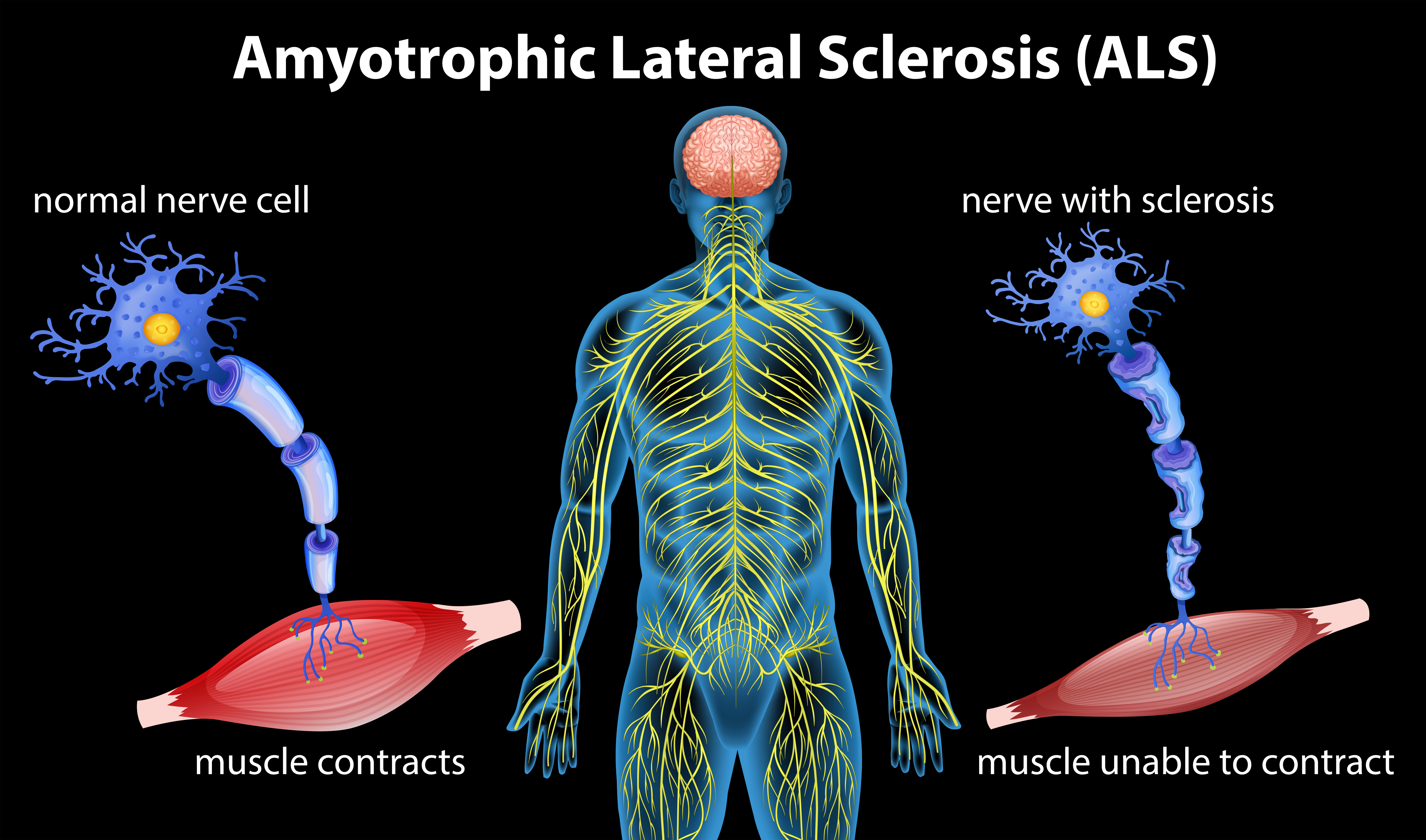
Slurred speech in bulbar ALS is the result of inadequate electrical conduction of nerve cells; the muscle fibers that these cells fire to receive impaired signals; hence, slurred speech (speech is controlled by muscles).
This nerve damage does not come and go. Once a person with bulbar ALS develops slurred speech, this symptom is there to stay.
So if what you perceive as slurred speech comes and goes…this heavily points away from bulbar ALS.
“Examining one’s tongue in the absence of any symptoms is not helpful, as there is no reason that the tongue should be affected clinically in the absence of any symptoms,” says Dr. Gerecke.
But what if you’re thinking that the twitching that you see in your tongue is only the first symptom of bulbar ALS, and that soon, more will follow? After all, wouldn’t there have to be a first symptom?
By the time a person with bulbar ALS sees their tongue twitching from the disease, the patient already has the symptoms (or some of) that Dr. Gerecke pointed out already.
And the tongue fasciculations of bulbar ALS look more like a bunch of worms squirming under the tongue, not the “twitching” that a healthy person sees in the mirror.
Dr. Gerecke has a special interest in ALS, myasthenia gravis, myopathy/muscular dystrophy, peripheral neuropathy and radiculopathy. She is board certified in general neurology and neuromuscular medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sirtravelalot
Can ALS Twitching Come Before Muscle Weakness?
A neurologist says that ALS twitching CAN come BEFORE muscle weakness.
There is information on the Web stating that in ALS, muscle weakness comes before twitching (fasciculations).
To know that muscle weakness begins appearing prior to any twitching can be a big source of reassurance to people who are literally trembling with fear that they may have the incurable motor neuron disease known as amyotrophic lateral sclerosis.
In the research I’ve done for my articles, I was not satisfied with the information I was finding pertaining to whether or not the muscle twitching in ALS preceded the weakness.
So I decided to ask a neurologist this simple question:
Can the twitching (fasciculations) of ALS precede the pathological weakness in the muscles?
“Muscle weakness and cramps can either precede twitching or twitching can precede muscle weakness and cramps,” says Bonnie Gerecke, MD, director of the Neurology Center at Mercy in Baltimore.
To read that is a blow to men and women who spend inordinate amounts of time ruminating that they might have this devastating condition.
“There is no absolute paradigm for the disease,” says Dr. Gerecke. “A patient can experience muscle twitching (fasciculations) as an initial sign or symptom of ALS, although weakness usually follows shortly thereafter in this case.
“It should be kept in mind that many individuals who experience muscle twitching do not develop ALS, as muscle twitching can be benign.”
ALS is a very rare illness, whereas benign fasciculations are part of being human; they are exceedingly common and have many harmless causes such as:
Health Anxiety

Freepik.com/pressfoto
General Anxiety

Shutterstock/T.Den_Team
Dehydration

A Hard Workout

Freepik.com
Mineral Imbalance

In fact, it may very well be that anxiety causes the twitching to gear up the body for a fight or flight.
In a sense, the muscle fibers are on standby to fight or flee—kind of like engines revving up for the big race.
But if that fight or escape never comes…but the anxiety persists, the muscles may remain in a twitching or revving-up mode for extended periods.
Dr. Gerecke continues, “Conversely, a patient with ALS may develop muscle weakness and cramps prior to the onset of twitching, and not all individuals with ALS develop twitching.
“Muscle weakness and cramps can also be due to many other conditions.”
Fact is, a hefty number of conditions cause weakness in the muscles.
And the weakness can manifest in different ways.
It can be gradual; it can be rapid or sudden; it can be accompanied by severe pain or be painless; it can come only after intense exercise and be temporary.
Cramps in the legs are often caused by dehydration, but can also come from an assortment of non-neurological conditions, such as inflammatory bowel disease.
Bottom line: There is no rule that the twitching in ALS necessarily comes before or after any muscle weakness (or cramps).
Dr. Gerecke has a special interest in ALS, myasthenia gravis, myopathy/muscular dystrophy, peripheral neuropathy and radiculopathy. She is board certified in general neurology and neuromuscular medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

School Bullying vs. Sibling Rivalry: Same or Different?
The only difference between school bullying and sibling rivalry may be their names.
Parents sometimes toss out that term, “rivalry,” to soften their perception of a truly bullying situation.
“Sibling rivalry and bullying at school can have the same impact on both the victim and perpetrator,” says Stacy Kaiser, a southern California-based licensed psychotherapist and relationship expert with a special interest in the topic of bullying.
“In both cases, the victim feels helpless, powerless, intimidated and out-of-control. He or she can be left with low self-esteem, depression, anxiety, a drive towards drugs or alcohol, and even suicidal thoughts.”
When this dynamic occurs, it’s not rivalry. Yes, sibling rivalry exists, but bullying is a different kind of behavior. Denying it by slapping on the label “rivalry” won’t make the problem go away.
“The perpetrator feels powerful, superior and a feeling of inappropriate pleasure,” continues Kaiser.
“He or she can be inspired to continue to bully both the sibling and the people at school, and that desire can escalate to bullying or physical violence in other environments.
“It allows the perpetrator to feel entitled, to have inappropriate boundaries and to develop a sense of grandiosity.”
Whether you wish to label the hostile behavior between siblings as rivalry or not, one thing is for sure:
Hostility between siblings brings a unique component that’s absent in the classroom between classmates:
The victim can’t get rid of the sibling. The victim lives with the bully. Even in the middle of the night, the bully might strike. School may even be something of a sanctuary, even if the victim is bullied there too.
“Sibling rivalry can actually be worse than bullying at school, because the siblings often spend more time together, and because of family obligations or loyalty, the victim is often less likely to tell the parents about the excessiveness or significance of the bad behavior,” explains Kaiser.
Furthermore (and very unfortunately), it’s not unheard of for the bully in the home situation to actually be favored over the victim.
In such a case, the parents tend to believe the bully’s version of events, even going as far as accusing the victim of “starting it” or “bringing it on,” or not being mature enough to stop complaining about it.
On the other hand, “bullying at school can be more intense, because the bully is attempting to get attention from an audience of their peers, whereas on the home front, the sibling is often doing it for their own gratification or revenge and not for attention.”
With over 100 TV appearances on major networks including CNN, NBC, CBS and ABC, Stacy Kaiser brings a unique mix of provocative insight to many topics such as anger management, office relationship issues and parenting.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}