

Should Elderly People Bench Press?

Why do so few elderly people at the gym bench press?
More appalling is that so few personal trainers have their elderly clients bench pressing.
The bench press is one of the easiest exercises to perform. Geez, the person gets to lie down, for starters. Older people with bad knees will welcome this. (more…)

Why Women Think It’s Polite to Accept Rides from Strangers

It’s actually true that some women will accept a ride from a stranger because they think it’s the polite thing to do, that it’d be rude to decline. (more…)

What Does the Hunger of Prader-Willi Syndrome Feel Like?

“Never feeling full” is a poor description of the hunger of Prader-Willi syndrome.
We’ve all been hungry, but not hungry enough to eat dog food or cardboard. (more…)

Why Don’t We See More Plus-Size Women Doing Deadlifts?

When’s the last time you saw a plus size woman doing deadlifts?
I don’t mean baby deadlifts with a 40-pound short barbell, but hammering it out at the “cage”? (more…)
Why Don’t Most Grown Abused Kids Beat Up Their Parents?
Why is it that adults, who were abused by their parents, don’t beat up their parents, who may still be relatively young and healthy? (more…)

Why Do Women Love the Inner Thigh Machine?

Isn’t it amazing so many women love the inner thigh (adductor) machine, yet are still blind to the failure of this machine to trim big thighs? (more…)

Feel too Fat and Clumsy to Exercise? Solutions You’ll Love

If you feel too fat & clumsy to exercise & have NO idea where to start, there are several kinds of exercise where you won’t have to worry about falling or stumbling. (more…)

Is It Safe for Elderly Women to Try Pull-ups?

If you’re an elderly woman who’d like to learn to do pull-ups, then go for it!
Elderly age, in and of itself, does not make it harmful for a woman to train at pull-ups or chin-ups.
“There’s no specific contraindication for an elderly woman without shoulder issues to try chin-ups,” says D’Wan Carpenter, DO, a board certified physical medicine and rehabilitation physician with SIMEDHealth in FLA.
“If she has never tried any exercise like this before, it would be best to work her way up to it.
“She will have to understand she will be relying solely on her arms to be able to lift the rest of her body. As long as both upper extremities are injury-free she is safe to try chin-ups.”
Brittle Bones
In fact, if a woman over age 65 has osteoporosis (brittle bone disease), her contraindications are impact exercise like running, jumping and certain forms of other aerobic activity.
Pull-up/chin-up training is a non-impact activity that’s safe on the joints.
Built-In Safety of Pull-ups
And I’ve got news for you: It’s not easy to overdo it with pull-up training. It’s pretty much basically this: You either can or you can’t do it.
It’s not like, say, the bench press, where you can keep straining and straining with endless sets and countless repetitions because you can adjust the weight of the barbell. You can then end up hurting a shoulder joint.
But with chin-ups, once you begin fatiguing, you have no choice but to quit and recharge fully before your next set, since you can’t adjust your body weight like you can adjust a barbell weight.

Depositphotos.com
Though sets can be overdone in terms of volume if a woman uses a gravity-assist machine, I strongly urge against this device, as it’s a poor way to learn to do a chin-up or pull-up. (More on that coming up)
So the issue isn’t the safety of pull-up and chin-up training for an elderly woman. The issue is her fitness level at the time she decides to pursue this goal.
Another issue is her body weight. If she’s overweight, learning chin-ups will be a lot more difficult than if she’s, say, 125 pounds.
Requirements for an Elderly Woman to Learn a Chin-Up
“Elderly” literally means over age 65, though the senior citizen discount at retailers begins at age 55; and age 55 and over is what often applies to senior housing. But you get the point.
A woman over age 55 or 65 who has a base fitness level from long-term strength training, and who’s not overweight, is an excellent candidate to learn chin-ups.
She is more likely to injure her elbows playing golf or tennis, by the way.
Next, she needs a healthy pair of stable shoulders; no rotator cuff issues or painful bursitis.
A requirement is the ability to dead hang from a bar for 20 seconds. This can take a while to build up to.
Once a senior woman is able to dead hang for 20, maybe 30 seconds, she will be that much closer to developing the strength to pull herself halfway up.
Assist Machines
Stay away from these. Though this article is about whether or not chin-up training is safe for the elderly woman, I’m going to briefly explain why assist machines are useless.
They skewer the position that the body naturally hangs in when hanging from a bar without the feet touching anything below.
If you’re doing pull-ups or chin-ups while your feet are connected to a moving platform that subtracts body weight, this will fail to mimic the natural hanging position.
In order to develop sufficient strength to pull yourself up with your feet dangling in the air, you must train with your feet dangling in the air.
So how do you train if you can’t even pull up one inch?
I’ll end up with a 2,000-word post if I explain everything, but suffice it to say that you must develop strength with cable pull-down motions, rowing motions and core-strengthening activities like pushups, kettlebell swings and planks.
And then practice your dead hanging.
At some point you’ll feel ready to attempt a pull. Have a partner place their hands on your waist to help you. You can also practice with tension bands.
Another way to practice is to have a stool at your feet so that you can pull up while your feet are still on the stool to help subtract body weight.
Unlike the assist machine, this subtraction won’t skewer your body’s natural hang position enough to thwart your training.
It is perfectly safe for an elderly woman, under the aforementioned circumstances, to learn how to do chin-ups and pull-ups.
 Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: ©Lorra Garrick

The Youngest Age You Can Teach Children to Deadlift

What’s the youngest a child can learn how to deadlift?
There is no research on this, so any fitness expert’s take on this is going to be based on anecdotal evidence. (more…)
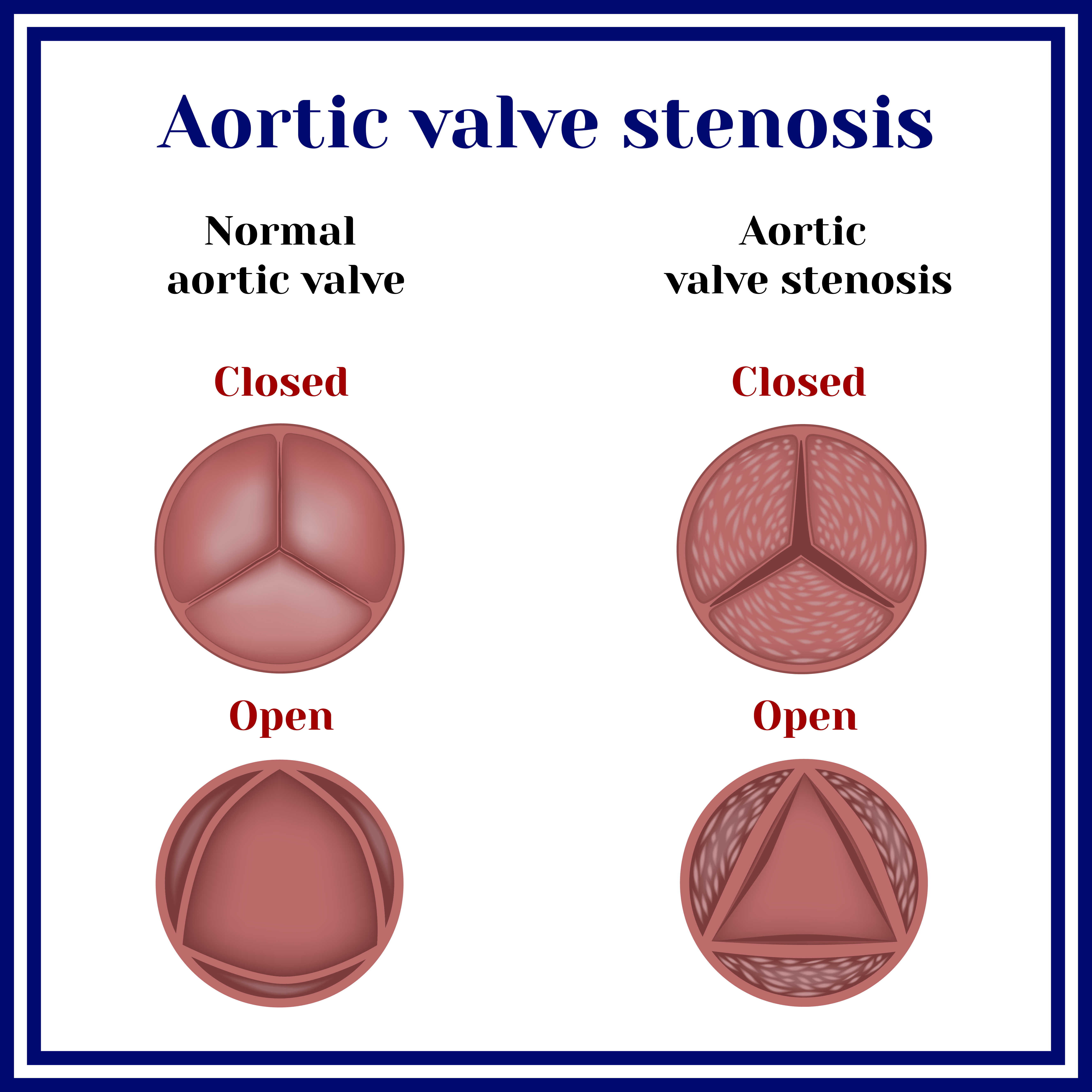
TAVR without General Anesthesia Has Better Results
Before you have TAVR, you should find out if your surgeon is set on using general anesthesia, because moderate sedation has benefits that general does not have.
Many people fear “not waking up” after undergoing general anesthesia, and sometimes they automatically assume that this type of sedation is the only option for the surgery that they’re planning on — even TAVR.
General anesthesia requires a breathing tube while moderate sedation does not.
General anesthesia is sometimes used for TAVR.
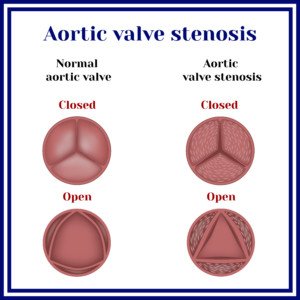
Researchers at the Perelman school of Medicine at the University of Pennsylvania showed that moderate sedation was equally or better overall than general anesthesia for TAVR (transcatheter aortic valve replacement).
“I agree that conscious sedation is better for TAVR, as most of the patients treated with TAVR are elderly and at increased risk of cardiorespiratory complications and post-operative delirium with GA,” explains Asim Cheema, MD, who’s board certified in internal medicine, cardiovascular diseases and interventional cardiology by the American Board of Internal Medicine. Dr. Cheema is with Your Doctors Online, an online doctor chat site.
“In addition, TAVR is a minimally invasive procedure with percutaneous access and ideally managed with sedation for patient comfort and a plan for quick recovery with early ambulation post-procedure,” says Dr. Cheema.
“The multicenter 3M study has shown that in a selected population, a minimally invasive approach with conscious sedation and an expedited recovery plan allows most patients to be discharged within 24-48 hours post-TAVR.”
So why would there ever be a need for general anesthesia?
The researchers relied on the STS/ACC TVT RegistryTM — a database of TAVR patients in the U.S.
They looked at elective cases of femoral artery approach minus an incision to compare general anesthesia with moderate sedation.
This meant nearly 11.000 patients, with 1,737 having received moderate sedation.
Advantage of Moderate Sedation in TAVR
• A lower rate of mortality within 30 days of the procedure
• A lower rate of stroke within 30 days
• A shorter hospital stay
The conclusion was that moderate sedation is safe, effective and potentially the choice approach for TAVR.
This conclusion applies to all kinds of TAVR patients, not just the relatively healthy and younger ones.
What are the three levels of “moderate sedation” anyways?
• Isolated local anesthetic at the site of catheter entry
• Twilight sleep (conscious sedation) in which the patient is lightly asleep but responsive
• Monitored anesthesia—an unconscious but arousable state. In general anesthesia that patient cannot be aroused and not responsive to any external stimuli.

Your Doctors Online offers a free 7 day trial where you can ask a doctor questions online and get answers in minutes from anywhere 24/7. Learn more here. Dr. Cheema teaches and provides supervision to graduate students at the Institute of Medical Sciences, University of Toronto.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}