
Why Are Some Cardiologists Not Concerned of Borderline Qtc?
Are you scratching your head wondering why your cardiologist is not the least bit concerned over your borderline QT prolongation?
This lack of concern is certainly not a rare event, in that it happens quite commonly. But we have to put it into context too. (more…)
Avoid Colon Cancer: Whole Grains, Exercise, No Processed Meat

The prevention of colon cancer begins with the big 3: Eat whole grains, exercise and avoid processed meats. (more…)

Why Do Heart Tests Look Normal When All Arteries Are Blocked?

A heart stress test can show a normal result despite the three major coronary arteries being blocked enough to put one at risk for a heart attack. (more…)

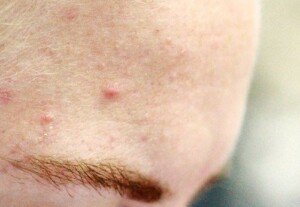
Sudden Acne Breakout in Healthy Adults: Causes & Solutions

Funny how acne commercials always show teens; sudden acne flares often strike adults including middle age; here are causes and solutions.
Causes of Adult Acne Flare-up (more…)

When Cancer Can Mimic an Earlobe Pimple: Know the Signs

The earlobe can be affected by all sorts of tiny bumps that can look like pimples, but bumps can also be caused by cancer: five kinds that have the potential to resemble pimples.
One of the hallmark features of a skin cancer that appears on an earlobe is that it doesn’t go away.
However, a benign lesion won’t always go away on its own, either.
Benign lesions such as an overgrowth of the epidermis (aka seborrheic keratosis) may continue to grow, as in, from one millimeter to the width of a pencil eraser, but will eventually stop – usually before they get to this width.
They also won’t crust, ulcerate or bleed – which is very possible with an ignored skin cancer.
How to Know when a “Pimple” on an Earlobe Is Actually Cancer
“Skin cancers that may resemble pimples or small pink-red bumps include basal cell carcinoma, squamous cell carcinoma and much less commonly, amelanotic melanoma,” says Emily de Golian, MD, a board certified dermatologist with Forefront Dermatology in Atlanta, GA.
“These may occur anywhere on the skin, but the most common area to develop basal cell and squamous cell carcinomas is the head/neck region, including the ear.” See top image: basal cell carcinoma.
Though what seems like a stubborn pimple can be a malignant growth, it can also be one of any number of benign conditions such as an inflamed hair follicle, clogged sebaceous gland, inflamed cartilage or cyst.
But don’t assume anything.
“A pimple-like bump that fails to resolve and/or grows over time, becomes tender or bleeds should be evaluated by a board certified dermatologist,” says Dr. de Golian.
Hopefully you will not convince yourself that the bump in question is a common pimple with an indefinite lifecycle just because it’s still there after several months.
If something won’t go away, no matter what it looks like, have a dermatologist inspect it.
“A wide variety of bumps on the skin may be normal, while others may represent skin cancer or precancer and require treatment,” says Dr. de Golian.
So if you’re afraid to hear what the doctor says, don’t let this stop you from making an appointment.
Telltale Signs You Have Cancer on an Earlobe
• Spontaneous bleeding
• Rapid growth—fast becoming increasingly nodular (bumpy or dome shaped) and/or dark
• Crusting, oozing, ulcerating
• Dark pigment “bleeding” out onto surrounding skin
Warning: Absence of these signs does not rule out cancer. Skin cancers always have an early stage, during which they may appear quite innocent—like a pimple.
Five Cancers that Can Look Like a Pimple on the Earlobe
Basal cell carcinoma. Typically presents as a tiny bump-like lesion with a pearly border or pearly overlay. See the next three images.

BCC. Shutterstock/Dermatology11

Shutterstock/Dermatology11

Shutterstock/Dermatology11
Location on an earlobe will make close inspection of this cancer’s classic pearly border very difficult, but from a further-out viewing, an early BCC can easily look like a harmless pimple.
A BCC can seemingly stay the same for several years, but eventually, if not treated, will invade surrounding tissue and become quite ugly.
BCC is the most common cancer of all, and 700,000 new cases a year are diagnosed in the U.S. Do not panic if you suspect a basal cell carcinoma.
Metastases to distant sites is exceptionally rare – and only in neglected cases.
Melanoma. Though melanoma is typically portrayed as looking like a “dark scary mole,” or a “black or purple mole with very jagged edges,” certain forms of melanoma can pass as a pimple.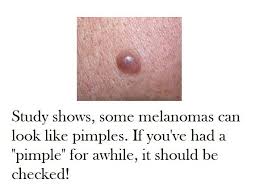
Amelanotic melanoma presents as flesh to pink colored, and nodular melanoma can start out pinkish.
Melanoma can appear anywhere where there’s skin, and that includes the earlobe.
Squamous cell carcinoma. Usually it doesn’t resemble a pimple, but it can.

Squamous cell carcinoma. Shutterstock/Dermatology11
Keratoacanthoma. This slow growing cancer can morph into squamous cell carcinoma.

Keratoacanthoma. Shutterstock/Dermatology11
Merkel cell carcinoma. This is very rare, but it can spread so quickly that in general, prognosis is poor.
:205-209")
Merkel cell carcinoma. Source: Archives of Craniofacial Surgery 2018;19(3):205-209
There is nothing intrinsic about the earlobe that would make these tumors any more threatening, from a biological standpoint.
But the earlobes sometimes just don’t get the attention that more viewable portions of the body get.
The entire outer surface of the ear should always be included in skin exams. And so should whatever inner areas you can see.
Here are details on how to conduct a thorough exam of your earlobes for cancer.
If you notice a pimple, don’t wait 30 days to examine it again.
Don’t obsess over the new “pimple,” but take a look at least every several days for suspicious signs.
 Dr. de Golian focuses on the surgical treatment of skin cancer via Mohs surgery, cutaneous oncology (melanoma and basal cell carcinoma), surgical defect reconstruction and cosmetic dermatology.
Dr. de Golian focuses on the surgical treatment of skin cancer via Mohs surgery, cutaneous oncology (melanoma and basal cell carcinoma), surgical defect reconstruction and cosmetic dermatology.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Kelly Nelson, MD, NCI, cancer.gov

Examining the Earlobe for Cancer: How & What to Look For

The challenge with new earlobe bumps is that they’re difficult to closely inspect when doing a monthly skin cancer exam.
The first thing you want to do is remove any hair from the ears, and this includes stray strands. (more…)

Survival Time if You Have a 20 Percent Ejection Fraction

An ejection fraction of 20 percent is pretty bad, and if you know someone whose EF is this low, you’ll wonder how much longer their survival time may be.
Three Year Survival Rate of 20% Ejection Fraction
A report in the International Journal of Cardiology took a look at the survival of congestive heart failure patients with very low left ventricular ejection fraction.
Low LV EF means that the left ventricle does not pump properly, resulting in an inadequate supply of blood for the rest of the body.
The general rule is that a very low EF is a predictor of mortality.
The study by Niebauer et al looked at 99 patients who all had ejection fractions of equal to or less than 20 percent.
• 74 had ejection fractions of 11 to 20 percent.
• 25 had EFs of 10 percent or less.
The patients were followed up after three years – at which point mortality came in at 74 percent.
However, it was determined that left ventricular ejection fraction was not a predictor of survival rate for these patients.
So what was? Peak VO2 – which was measured at the beginning of the study. Peak VO2 turned out to be a strong predictor of mortality.
What is peak VO2?
This is the maximal oxygen consumption or uptake, as it is measured during exercise in which intensity is incrementally increased.
A common way to measure this is a treadmill test, in which the tread surface starts out as flat (zero incline) while the patient walks at a slow speed.

And while the speed remains the same, the tread is gradually inclined higher and higher until the subject reports that the workload is difficult.
Ejection fraction is the percentage of blood, relative to how much the heart chamber is filled with, that gets pumped out with each beat.
Blood is pumped through the aorta, which branches out with vessels that further branch out so that the entire body receives oxygenated blood.
VO2 will be very negatively impacted when someone with a very low EF is engaged in exercise with increasing workload.
The conclusion of the Niebauer study is that when ejection fraction is “very low,” three year survival is also low.
“However, once the ejection fraction is < or =20%, ejection fraction is no longer a predictor of mortality,” says the paper.
“These results suggest that it is unlikely that small increases in ejection fraction will be associated with a survival benefit in this group,” continues the paper, “and treatments aimed at increasing peak VO2 may be more appropriate.”
A study in the American Heart Journal by Gula et al says, “Among patients with ejection fraction less than 20%, there was no detectable relationship between survival and ejection fraction.
“Among patients with an EF between 20 and 35%, a 5% increase in EF was associated with a lower mortality.”
So the question then becomes, What is the survival time if you have an ejection fraction of over 20 percent but under 35?

Shutterstock/ Africa Studio
And, as a general rule, without taking into consideration the very small Niebauer study, how long can a person with an ejection fraction of about 20 percent be expected to survive?
“It is difficult to predict survival in patients with very low ejection fractions because comorbid conditions play a major role,” begins Waqar Khan, MD, who’s been providing state-of-the-art cardiology services to the Houston area for over 20 years, and is author of “Be Heart Smart: Understand, Treat, and Prevent Coronary Heart Disease.”
“However, we can say that patients who have ejection fractions below 35% do not live as long as patients with normal ejection fraction.
“Broadly speaking, survival in such patients is less than 50% at about 10 years.
“And it’s much worse in patients who have ongoing coronary heart disease or other comorbid conditions that are not stable.
“Such conditions may include uncontrolled diabetes or kidney failure or other medical conditions.
“Such patients may also be placed on a waiting list for heart bypass.”
Dr. Khan discusses options for increasing the survival odds of people with ejection fractions as low as 20%.

Waqar Khan, MD, has a private practice and serves as an affiliate faculty member at Baylor College of Medicine in Houston, TX.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sources
ncbi.nlm.nih.gov/pmc/articles/PMC2644051/
ncbi.nlm.nih.gov/pubmed/10501338
heart.org/HEARTORG/Conditions/HeartFailure/AboutHeartFailure/Types-of-Heart-Failure_UCM_306323_Article.jsp#.WbXXxbKGPxM
Causes of Jaw Pain Other than Heart Attack Include Cancer

Causes of jaw pain other than heart trouble include cancers affecting the jaw—of which there are quite a few types.
If you’ve been experiencing jaw pain lately, perhaps you’re scared out of your wits that this means an impending heart attack or very clogged arteries.
So in an attempt to reassure yourself, you’ve sought out what can cause jaw pain other than heart troubles.
Cancer may be the furthest thing from your mind when it comes to jaw pain.
But the reality is that different kinds of malignant tumors can affect the jaw and thus cause pain.
But does this mean that your jaw pain, if not from a heart attack or other heart problem, is most likely from cancer? Of course not.
Causes of Jaw Pain Not Related to the Heart or Cancer
• Temporomandibular joint (“TMJ”) disorder
• Gum disease
• Abscess
• Cavity
• Gaps between teeth (pain occurs when chewing)
• Hairline fracture from impact trauma
• Pregnancy (which softens joints body-wide)
• Bone infection
• Cyst
• Benign tumor
• Trigeminal neuralgia brought on by vascular pressure on the trigeminal nerve
Cancers Affecting the Jaw
• Ameloblastoma (usually benign but in rare cases is malignant)
• Osteosarcoma
• Ewing’s sarcoma
• Multiple myeloma
• Metastatic cancer
• Malignant tumor pressing on the trigeminal nerve
Overall, cancers that affect the jaw are rare. Heart problems are extremely common.
Most of the other potential causes for jaw pain are also pretty common.
Thus, there is no need to panic, but do see a doctor right away, if for no other reason than to seek pain relief.
Jaw pain that occurs when the mouth is at rest or that’s accompanied by other symptoms is particularly concerning.
This is worrisome especially if those other symptoms are chest/back/arm pain, sweating, nausea, fatigue (indicates heart trouble) or a sensation of a stuffed nose, nasal discharge not related to a cold, or lump near the nose or eye (suggestive of a tumor near the jaw affecting the sinus area).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Damir Khabirov
Sources:
colgate.com/en/us/oc/oral-health/conditions/temporomandibular-disorder/article/jaw-pain-causes-why-you-might-be-feeling-pain-0613
medicinenet.com/jaw_pain/symptoms.htm
webmd.com/pain-management/guide/trigeminal-neuralgia#2-4
rarediseases.org/rare-diseases/ameloblastoma/

Hard Pimple that Won’t Go Away After 2 Months May Be Cancer

The warning is real: A hard “pimple” that’s still there after a few months with no sign of going away may be a deadly cancer.
“The most concerning things that can present in this manner are skin cancers: melanoma, SCC and BCC,” says Erum Ilyas, MD, a board certified dermatologist who performs adult and pediatric medical dermatology, cosmetic dermatology and skin cancer treatment with Schweiger Dermatology Group.
• Nodular melanoma — above image (very deadly if not caught early; fast growth). It’s hard.
• Nodular squamous cell carcinoma (growth not as fast as NM; but can still metastasize and kill)
• Basal cell carcinoma (very slow growing, usually never metastasizes; death is exceedingly rare)
“A harmless ‘pimple’ should last about two to three weeks,” says Dr. Erum.
A typical pimple — which contains oil, bacteria and harmless debris — will not stay on your face for two months when left alone.
Common harmless pimple
“It will go through natural stages of first ‘developing,’ then ‘coming to a head’ or to its peak size, then healing,” explains Dr. Erum.
“It may remain pink or discolored after this point for a few more weeks, but in general should be flat and no longer palpable.”
Two Months and You Still Have the Same Hard Pimple?
“Concerning ‘pimples’ are ones that do not naturally proceed through these stages,” says Dr. Erum. They develop and appear as though they will come to a head or to their peak size. Then, they do one of a few things.
“They either persist as they are without healing, they continue to enlarge, or they progress through stages where they appear to be attempting to heal only to recur again and not quite go away.
“The most common to present in this manner, the classic ‘blind pimple’ that doesn’t heal, would be a basal cell carcinoma.
Basal cell carcinoma. Shutterstock/Dermatology11
Basal cell carcinoma. Shutterstock/Dermatology11
“In their initial stages they can be difficult to distinguish from benign lesions. Many times patients tell me they tried to pop it, but just couldn’t seem to get anything out of it.
“Or, they say they thought it was going to heal but it kept growing back.
“Squamous cell carcinoma can present this way as well.” SCC’s can really look like pimples , as in the one below.

Squamous cell carcinoma
Since when does melanoma look like a pimple?
Few melanoma pamphlets warn of a growth that looks like a zit. Dr. Ilyas explains, “Nodular melanoma is a very aggressive form of melanoma that can develop rapidly.
“I have had patients tell me they watched what looked like a pencil dot develop into the size of a grape in less than three weeks.
“These do not always have a ‘core’ — they can often be smooth or dome shaped. The key that tells you it should not be there is just how quickly it develops.”

Nodular melanoma. Source: pcds.org.uk

Nodular melanoma
Features that Make a “Pimple” Highly Suspect for Skin Cancer
1 After a few months it hasn’t budged.
2 Especially, after two months it’s bigger.
3 Very firm and hard.
4 Upon close inspection you realize it doesn’t quite look like other pimples you’ve had.
If you’ve seen photos of basal cell carcinoma, they may have been of very invasive forms – in which patients ignored the progressing growth for many years.
When ignored, BCCs can invade neighboring tissues and cause a gruesome situation. But in their early form, a basal cell cancer can look like a pimple. It can even seem to heal, but it will come back if this happens.
So if you’ve had an untouched pimple for two months that finally “went away,” but then it returned…have a dermatologist inspect it.
No need to panic. BCC is the most common overall cancer in the world but extremely rarely fatal – and in fatal cases the patient ignored it for many years.
A BCC may initially appear as a little pimple with a blackhead that you could squeeze out, but then it doesn’t heal like a pimple should.
Should you panic over a hard pimple that you still have after two months? Don’t lose sleep tonight, but next day book an appointment with a dermatologist.
As far as incidence rates, it’s far more likely to be a basal cell carcinoma, as this is diagnosed in 750,000 Americans every year according to the Skin Cancer Foundation.
 Dr. Ilyas has practiced dermatology in the Philadelphia area and Boston for 15+ years and has served as Assistant Professor of Dermatology at Drexel University College of Medicine.
Dr. Ilyas has practiced dermatology in the Philadelphia area and Boston for 15+ years and has served as Assistant Professor of Dermatology at Drexel University College of Medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can You Get Angina Chest Pain Several Months After CABG?

Chest pain from angina can come back after a seemingly successful CABG procedure.
When angina returns or occurs a few months or so after CABG, it’s called late recurrent angina. (more…)


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}