

Is Ejection Fraction a Predictor of Mortality?

A cardiologist addresses the question of ejection fraction being a predictor of mortality.
Ejection fraction is the amount of “squeeze” or force that a heart yields with each beat.
Can this actually be a predictor of mortality?
“If the ejection fraction (EF) is due to poor blood flow to the heart, due to coronary disease, it is a predictor of higher mortality especially if the EF is less than 35%,” explains Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Coronary artery disease (CAD) is characterized by plaque buildup inside the artery walls of the heart, which decrease blood flow through the cardiac muscle.
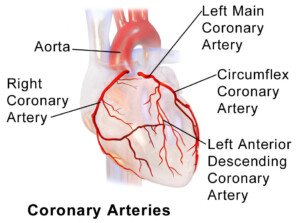
BruceBlaus, CreativeCommons
A diet full of trans fats significantly contributes to this or may even outright cause it.
“If the low EF is due to some unknown cause, perhaps a prior viral infection or just out of the blue, the heart itself is probably pretty normal, and usually the ejection fraction will recover, but until it does there is higher mortality than a normal person, but less than the first scenario I mentioned,” explains Dr. Sayeed.
“Regardless if the EF is less than 35% for more than three months on optimal medical treatment, these people all need defibrillators to prevent sudden cardiac death and decrease their mortality.”
Though ejection fraction then, indeed, plays a role in mortality prediction, it is not the greatest predictor of mortality. That goes to heart rate recovery (HRR).
“Slow heart rate recovery occurs in those people with coronary artery disease and blockages and with heart muscle damaged by this.”
Slow or low HRR also occurs in those who do not exercise sufficiently.

Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

Can a Marathon Runner Have a Low Ejection Fraction?

Marathon runners usually have strong hearts, but believe it or not, they can actually have a low ejection fraction, says a cardiologist.
You may have heard that it’s possible for a marathon runner to have an ejection fraction as low as 35 percent.
This is information that’s not easily forgettable, since a low ejection fraction is associated with people who have congestive heart failure or some acute process going on with their heart.
What Is an Ejection Fraction?
Ejection fraction is a measure of the amount of blood that is pumped out of the heart with each beat.
A low EF means that the heart does not pump as much blood as it should with each beat or squeeze.
• The heart’s chambers fill with a normal amount of blood, but the pumping action of this muscle is weak.
Therefore, an inadequate amount of blood gets pumped out for circulation throughout the body.
• Or … the pumping action is actually normal. The problem is that the chambers fail to fill with a normal amount of blood.
The result is a sub-optimal amount of blood going throughout the body.
• It is difficult to fathom that a marathon runner would have either of these situations.
Can marathon runners have a low ejection fraction?
“Yes, they could have a low EF, but it would be very rare,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“Only a rare person who was very well-trained or could handle the symptoms could actually have a low ejection fraction and complete a marathon, as they would likely have to stop running long before the end of the marathon due to shortness of breath and chest pain,” explains Dr. Sayeed.
If you have shortness of breath disproportionate to your physical activity; new-onset shortness of breath; chest pain or tightness; a faint feeling; or nausea, see a cardiologist/emergency room physician as soon as possible.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
THORACIC AORTIC ANEURYSM: Weightlifting & Cardio Guidelines

Top surgeons answer questions about just how much you can and cannot lift with a thoracic aortic aneurysm.
After all, information on sites like Mayoclinic.com is conflicting, generic and vague — open to much subjective interpretation.
For instance, just what exactly does “Don’t lift more than half your body weight” mean?
Does this apply to biceps curls? Seems that a 200 lb. person would strain a LOT more with trying to curl a 100 lb. barbell versus deadlifting it.
And if body weight is a criterion for how much a person with a thoracic aortic aneurysm can lift or should avoid lifting, then wouldn’t body composition play into this equation?
Does it make ANY sense at all that, according to the “Don’t lift more than half your body weight rule,” a 300 lb. person with 200 pounds of excess fat gets to bench press 150 lbs. — while a 200 lb. person who has way more muscle mass and upper body strength gets limited to lifting only a 100 lb. barbell just because they found out they have a thoracic aortic aneurysm?
What Are Your Questions About Strength Training with a Thoracic Aortic Aneurysm?

Freepik.com
Find out the answers to these riveting questions and many more in the articles linked below.
Some are interviews with aortic repair surgeons. Trust me — I left NO stone unturned!
- Putting into context the fact that research into weightlifting with an aortic aneurysm is very scarce.
- Safe weightlifting practices.
- Are deadlifts really dangerous? Yeah, if we’re talking about one RMs, but what about for fitness?
- Are pull-ups potentially risky?
- Guidelines for barbell squats
- Safety guidelines for biceps curls
CARDIO
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Rotator Cuff Injury Pain vs. Biceps Tendonitis: Comparison

Symptoms of rotator cuff injury and biceps tendonitis overlap; a sports medicine doctor explains if there’s a way to tell difference.
Is there a way to tell the difference between the symptoms of a rotator cuff problem and that of biceps tendonitis?
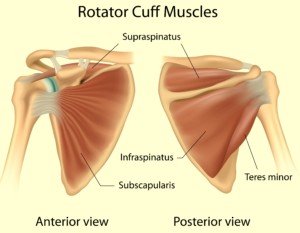
“The reality of rotator cuff and biceps tendonitis injuries is that they go hand in hand,” says Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
“It is rare to have them occur separately because the rotator cuff is comprised of four muscles, and the long biceps tendon attaches in the shoulder in between the first and second rotator cuff muscles,” continues Dr. Galland.
“One of the functions of the biceps tendon is identical to that of the rotator cuff, so when the rotator cuff is not healthy, the biceps tendon, under extra pressure, follows suit and can easily become unhealthy as well.”

Biceps tendonitis. Shutterstock/ilusmedical
Certain weightlifting exercises are more likely than others to injure the rotator cuff, namely chest and shoulder work.
The biceps tendon can also be injured with these exercises, and that includes the bench press.
Shutterstock/Alila Medical Media
You may be wondering how the biceps can be injured doing chest work when the biceps isn’t even involved in pressing motions.
But actually, the short head of the biceps does indeed play a minor role in pressing motions because chest pressing involves shoulder flexion. The biceps attaches to the shoulder joint.
“It is difficult to distinguish whether you have a rotator cuff or biceps tendon injury, since many of the symptoms overlap,” continues Dr. Galland.
“The truth is that there is so much connection between the two, to try to distinguish them is really an exercise in futility.
“If you have biceps tendonitis, you likely also have rotator cuff dysfunction.
“Again, while it is difficult to tell for sure because of the similarity in the symptoms, you can do this exercise to test for biceps tendonitis:
“First, bring your arm straight ahead and then try to raise it while pushing down on the arm with your other arm.
“If pain is present, you likely have biceps tendonitis.” That pain will be in the shoulder.
“Biceps tendonitis and rotator cuff injuries can both be treated with injections and subsequent physical rehabilitation.
“This is not something to ignore – if you have pain that you believe to be your rotator cuff and/or your biceps tendon, see your orthopedic specialist immediately.”

Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/KlaraBstock

Can Sore Neck Muscles from Weightlifting Cause Headache?

Not only can sore neck muscles from working out with weights cause a headache, but don’t underestimate what bad sitting posture can do, either.
A headache can be an alarming symptom, but remember, the head is like any other part of the body, in that if it’s the site of aggravation, a headache can often result.
And that site doesn’t necessarily have to be on the head itself; it can be nearby.
And this includes from lifting weights; the neck muscles are located in close enough proximity to the head to cause a radiating pain or ache that travels upward.
Let’s first look at lifting weights.
“Weightlifting can certainly cause headaches, especially when neck muscles are overworked, causing hypertrophy and sometimes muscle spasms,” says Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
These muscle spasms can register over 5 on the 1 to 10 pain scale.
Strength training moves that involve the neck muscles include shoulder shrugs, the deadlift and other pulling exercises.
But now another question is triggered…
Just what is the mechanism for these headaches that are induced by lifting weights?
Dr. Galland puts it this way: “Overworked muscles = spasm = tightness—which causes direct pain of scalp muscles or indirectly by pinching occipital and other scalp nerves.”
Nerve pain can really hurt, even if it’s a spasming muscle and lactic acid encroaching upon the nerve.
What about poor sitting posture?
Dr. Galland says, “One of the most common causes of headaches are muscles that are made sore from tension and the constant hunching over computers.
“When we do not sit up straight, our heads have to extend backward, which causes spasm and strain.
“Occipital neuralgia, which is quite rare, can cause very sharp, intense pain, can occur when your neck muscles are in spasm and contracted.”
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/iambasic_Studio

Six Reasons You Have Joint Pain at Night

Are you plagued by joint pain at night?
Joint pain at night is no picnic, and it can be caused by one or more of several factors.
Nighttime Joint Pain vs. Muscle Aches
“The first thing to determine is whether what you are feeling is really joint pain, rather than a muscular ache,” says Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
A distinguishing factor between pain in a joint and pain in a muscle is that the former seems to be coming smack from the joint itself.
The ache of a muscle, on the other hand, seems to originate in the fleshy area of the muscle — between joints.
“If the discomfort you are feeling truly is joint pain, it will most commonly be caused by arthritis, carpal tunnel syndrome, rotator cuff dysfunction or joint degeneration,” says Dr. Galland.
“If you are experiencing joint pain – not just muscle soreness – this discomfort should warrant a visit to an orthopedic surgeon.”
Make sure that any joint pain that you’ve been experiencing at night is not related to premenstrual syndrome (PMS).
A woman can also get mid-cycle joint pain. However, this can occur during the day as well.
Surprising Causes of Joint Aches at Night
There are more causes of joint discomfort overnight that deserve some mentioning: microscopic colitis, as well as Crohn’s disease and ulcerative colitis.
Add lupus and Sjogren’s syndrome to this list. However, as with mid-cycle joint pain, this symptom can occur any time of the day.
I had a bout with microscopic colitis (confirmed via colonoscopy), and this benign condition can present with one or more of several symptoms, including joint aches and dehydration.
These two symptoms I definitely had, along with the hallmark diarrhea.
If you have microscopic colitis, you’ll know something’s up: It causes watery, painless diarrhea, though the diarrhea may also be more “formed.”
This condition causes release of prostaglandins, the same hormones that are released during PMS that cause aching joints!
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes
Source: raskov.org/en/patient-information/microscopic-colitis

Cause of the Ache in Your Tailbone when Sitting

Here’s what can cause the ache in your tailbone when you’ve been sitting. And what to do.
Does your tailbone hurt after you’ve been sitting for a while, even though you haven’t recently fallen on it?
“Although there is not one single answer to this question, the most common cause is coccydynia,” says Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
“This is a condition in which the smallest segment of the spine, the coccyx or tailbone, is irritated or inflamed,” continues Dr. Galland.
“This type of inflammation can be caused by arthritis, or post-traumatic or repetitive stress. This is a condition that is seen more commonly in slender people who do not have very much tissue in that area of their body.”
Does this mean gain weight if your tailbone is hurting or aching from sitting?
If you’ve always felt you were underweight, then perhaps it’s time to increase your caloric intake by eating more “clean” whole foods such as chicken, turkey, lamb, grass-fed beef, nuts and whole grains. Take up strength training to add muscle.
A physically fit person, or to put it another way, a person with a well-trained body, should not experience tailbone from sitting as long as the seat is comfortable rather than a hard slab of wood.
But if you’ve made sure the seat is comfortable and padded, and if people often call you “thin,” then maybe some healthy weight gain is in order.
Eating more junk food to add more fat is not a good solution to eliminating the hurt of a tailbone from sitting.
Make it a point to avoid sitting for long than 30-45 minutes at a time; get up every so often and walk around. Make sure your posture is correct when sitting.
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/fizkes

Why Your Grip Can Be Causing Elbow Pain when Bench Pressing

There’s a specific reason why your elbow hurts or feels “funny” when you bench press.
The tweaky kind of pain may occur the most as you remove the bar from the rack, then lessen a bit as you lower, then return more as you press up.
Elbow pain is caused by the grip.
If you have golfer’s elbow, chances are it hurts to grip things regardless of hand position (e.g., underhand, overhand).
Golfer’s elbow is an inflammation of the tendon that’s located at the inner portion of the elbow (medial to the body).
As a result, perhaps you’ve backed off on grip-and-pull exercises like lat pull-downs, rows and deadlifts. However, does your golfer’s pain kick up when you bench press?

Depositphotos.com
Perhaps the distinct discomfort is most pronounced when you lift off the bar, but subsides during the actual bench pressing. Or maybe it persists throughout the entire set.
Bench pressing itself won’t cause golfer’s elbow (however, it can cause tennis elbow: inflammation of the lateral epicondyle tendon, whereas golfer’s affects the medial or inner epicondyle tendon).
However, the bench press can stimulate the medial epicondyle tendon.
“Pain that is transmitted to the elbow during a bench press usually means that one is putting too much pressure on this joint as the force is transmitted down from the wrist to the arms and then shoulder,” says Dr. Moshe Lewis, MD, board certified in physical medicine and rehabilitation.
“Since the common flexor tendon attaches this muscle (the flexor muscle) to the interior of the elbow joint or medially, if it is already inflamed then a forceful grip during a bench press is likely to increase pain.
“One can decrease the grip — keeping the palm open and the bar balanced — and/or lower the amount of weight being pressed to help minimize further damage.”
 Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Syda Productions

Cause of Sudden Severe Shoulder Pain that Comes and Goes

Find out why you get sudden “pain attacks” in your shoulder that can stop you in your tracks.
You’re just sitting there, maybe watching TV or eating, when suddenly, it strikes out of the blue: yet another pain attack of your shoulder, biting down hard on you.
You must stop what you’re doing and try to bear the pain without loudly moaning.
Let’s assume you’ve had your heart, aorta and lungs examined to rule out any conditions with these structures, as problems with these can indeed radiate discomfort to the shoulder.
So where can this intense, sudden shoulder pain come from, if you haven’t recently fallen on this joint, been hit there by a baseball or broken a bone there?
“Here too, making sure there is not a muscle or ligament tear is important, i.e., clinical exam and MRI,” says Dr. Moshe Lewis, MD, board certified in physical medicine and rehabilitation.
But let’s assume you’ve already had an exam and MRI, indicating no tear.
“If this is negative, presumably, the pain still has to be minimized or else therapy will only flare things more.
“Options include an anti-inflammatory or icing for acute pain, heat for chronic pain.”
So what’s causing your sudden, severe shoulder pain?
It’s likely arthritis or shoulder impingement.
Impingement is when the top of the humerus bone of the upper arm impinges upon one or more of the tendons of the rotator cuff, literally fraying it. See the image below.
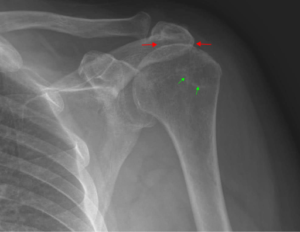
Even if you think you’re sitting still, tiny, subtle movements in your position could shift the humerus against the inflamed edges of a rotator cuff tendon. This really hurts.
Another possible cause of sharp pain in the shoulder that comes and goes:
“Sometimes a cervical pinched nerve can masquerade as shoulder pain,” says Dr. Lewis.
“A good exam is in order.” This would likely be an MRI of the neck.
Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/SpeedKingz

Will Surgical Tibia Lengthening Improve Back Squat Leverage?

More and more people are having their tibias or shins surgically lengthened strictly for cosmetic purposes: that of being taller.
Surgical techniques for tibia lengthening have improved over the years, and people who desperately want to be taller are undergoing this painful procedure.
As a former personal trainer, and lifelong fitness buff, I am acutely aware of anthropometrics, particularly limb leverages as they apply to the back squat exercise.
I’ve already written quite a few articles on “long femurs,” meaning a femur longer than torso length will put a person at a biomechanical disadvantage in the back squat.

Short shin, long thigh
However, those whose femurs are equal in length to their torso, rather than longer, will still have a biomechanical disadvantage in the back squat — if their shins are disproportionately short for their whole leg.
The reason is that in order to keep from toppling backwards in a back squat, one must align their shoulders over their midfoot.
To put it another way, the foot has to get under the buttocks while squatting. The more under the buttocks the feet are, the less the athlete needs to lean forward.
Short Tibias Are a Disadvantage in the Back Squat
People with relatively short tibias can’t get their feet well under their butt. (Note “relatively” here; having “short shins” has NOTHING to do with overall body height; a tall person can have relatively short shins, and a short person can have relatively long, pedestal-like tibias),
To compensate in a back squat, they must lean far forward: not an efficient position for a back squat. Imagine someone with shins much shorter than their femurs.
Picture a profile of them squatting. Now “grow” their tibias to be longer than their femurs.
What happens? Long tibias act as support pedestals for a back squat.
So would surgical tibial lengthening enhance one’s ability to do a back squat?
Well, from a biomechanical standpoint, the answer is yes if recovery is complete; longer tibia relative to femur means better leverage.
But does this mean it’s a smart idea to undergo surgical limb lengthening if both your limbs are the same length, your legs are straight (no bone deformity) and all you want is better anthropometrics for the back squat?
Doctor’s Perspective on Tibia Lengthening
“As you know, many MDs frown on back squats because people tend to get carried away and put too much strain on this often weak or conditioned set of muscles,” says Dr. Moshe Lewis, MD, board certified in physical medicine and rehabilitation.
“I don’t know too many orthopedic surgeons who recommend tibial lengthening sheerly for cosmetic reasons or being able to do squats.
“The patients I have who had these procedures typically have more than 2 inches leg length discrepancy, typically having had a fracture or hip surgery.”
Bottom line: Don’t even think of having your tibias surgically lengthened to improve your back squat.
You’d need to avoid weightlifting for two years following this procedure for complete recovery! And complete recovery isn’t even guaranteed.
Plus, the cost is astronomical and not covered by insurance.
Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}