

Cause of Dry Mucous Chunks in Nose Every Morning

Learn the cause and solutions to dry mucous chunks in your nose every morning.
Regarding what causes chunks of dry mucous to build up in one’s nose overnight and cause a blockage in the morning, the expert source is Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
“Nasal dryness is a more frequent issue in high altitude and colder climates,” says Dr. Silvers.
“If the nose is dry then mucous will dry, causing it to get stuck in the nose.”
The mucous becomes thick and sticky, becoming trapped in the nasal passages.
Dry nasal conditions can result from various factors, including low humidity, certain medications or medical conditions like allergies or sinus infections.
When mucus dries and becomes sticky, it can make breathing more difficult and may lead to discomfort or congestion, or simply like something’s stuck and compacted up the nostrils.
Fiercely blowing your nose is often ineffective with dry chunks of gunk because they’re so stuck into the nasal passages.
Using a humidifier, staying hydrated and using saline nasal sprays can help keep the nasal passages moist and prevent all that yucky gunk from becoming too dry and stuck.
Sinus Congestion
“Chronic congestion and nasal obstruction causes oral breathing; this can dry out the mouth and the nose especially at night,” adds Dr. Silvers.
“Dry membranes lead to dried mucous and ‘dry mucous chunks’ in the morning.”
If the problem is related to structural blockage in the nasal passages, the buildup of dry mucous will likely be greater on one side of the nose than in the other.
“Patients actively suffering with a cold or with nasal allergies may have higher mucous production that does not clear.”
Dr. Silvers recommends a morning sinus rinse to clear out the accumulation of the unpleasant substance.
Using a neti pot every morning can help prevent this problem.

Neti pot. Shutterstock/kavzov
A neti pot is a small, teapot-shaped device used for nasal irrigation to help clear nasal congestion.
It works by delivering a saline solution into one nostril and allowing it to flow through the nasal passages and out the other nostril, effectively rinsing away gunk and goop, allergens and other debris.
Use of a neti pot also adds moisture to dry nasal passages.
It’s important to use clean water (boil it first for five minutes) and thoroughly wash the neti pot after each use.
When finished, you’ll find that if you give your nose a good blow, a little more mucous should come out.
A humidifier overnight may also be helpful at reducing chunks of gunk in your morning nose. Give it a try.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Cause of White Slimy Stuff on Inside of Lips

A physician explains where the white slimy gunk on the inside of lips comes from…
Have you experienced a white, slimy, goopy substance on the inside of your lips?
“The slimy substance in the mouth is the oral mucosa that is peeling,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
“Oral mucosa is like skin cells, will slough off as newer mucosal or skin cells develop.
“This can be exacerbated by certain mouthwashes and toothpastes, especially if the toothpaste or mouthwash is in the mouth for an excessive period of time. This is similar to exfoliating the skin.”
If you’ve noticed a slimy white substance on the inside of your lips, switch oral care products and see what happens.
Dr. Silvers says that this problem can also be caused by side effects of certain medications.
These medications include:
• Antibiotics
• Anticholinergic medications
• Antihistamines
• Cortiscosteroids that are inhaled
• Chemotherapy agents
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/massimofusaro

Herniated Disc: Can Excessive Bed Rest Make It Worse?

Warning: Lying down in the name of herniated disc pain is not a smart decision.
Pain in the back (or radiating down the buttocks and/or the leg) from a herniated disc?
It may seem logical to just lie down whenever the pain becomes aggravating, even if this is on a frequent basis.
In fact, this is the advice by medical professionals in years past. And it seemed to make sense. After all, if something hurts, give it some rest by not moving it, right?
And the best way to keep a body part, especially the back, immobile is to get a lot of bed rest.
However, this way of thinking is being overhauled.
Just what are the guidelines for bed rest in those with a painful herniated disc?
“Two to three days of bed rest or recumbency are recommended for a patient with an acute disk herniation,” says Stephen T. Onesti, MD, a neurosurgeon specializing in the spine, with Neurological Surgery P.C. of Long Island. Acute means sudden-onset.
“After this, it is recommended the patient be mobilized and get into therapy and pain management quickly.
“If there are neurological deficits [e.g., leg weakness] or extreme pain, consultation with a spine surgeon is recommended.”
Excessive Bed Rest Will Worsen Symptoms of a Herniated Disc
“It is important that patients do not spend too long on bed rest,” says Dr. Onesti. “Recumbency results in negative metabolic effects and is psychologically debilitating.”
One may begin feeling as though they are on the disabled list from all that time in bed being unproductive.
Furthermore, unwanted weight gain can easily result over time, fueling the feeling of powerlessness.
Dr. Onesti adds, “Also, it is usually not necessary to see a spine surgeon right away.
“Rehabilitation doctors, chiropractors, neurologists and pain management specialists are also effective providers.”
 Dr. Onesti is a board certified neurosurgeon specializing in spine surgery and surgical treatment of chronic pain. He has published many articles in peer-reviewed journals and has given numerous presentations at local and national meetings.
Dr. Onesti is a board certified neurosurgeon specializing in spine surgery and surgical treatment of chronic pain. He has published many articles in peer-reviewed journals and has given numerous presentations at local and national meetings.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Photographee.eu

How to Take Aleve for Herniated Disc Pain Relief

A spine doctor explains how to take Aleve for pain relief from a lumbar herniated disc.
After all, many people actually do wonder just how to take Aleve to combat the discomfort of a herniated (bulging disc).
The instructions on a bottle of Aleve state to take once every 12 hours; it’s a “12 hour relief” pain pill. This is commonly advertised in TV commercials.
Because Aleve is also an anti-inflammatory drug, a person with pain from a herniated or bulging disc may be advised to take this drug to reduce inflammation.
For how many days should a person be consistently on Aleve (or other similar NSAID) before it becomes effective for reducing pain from the inflammation of a herniated disc?
“Regular NSAIDS should be taken three times a day; a minimum of three days should be tried before the effects of the medication can be evaluated,” says Stephen T. Onesti, MD, a neurosurgeon specializing in the spine, with Neurological Surgery P.C. of Long Island.
Is three times a day safe, even though the directions for Aleve state take once every 12 hours?
Dr. Onesti explains, “Most regular NSAIDS are prescribed three times a day. Certain ones like Celebrex are indeed only used twice a day. It will be noted on the prescription.
“Also, patients with kidney problems may not be able to take NSAIDS at all.”
Causes and Risk Factors for a Herniated Disc
Source: myupchar. com
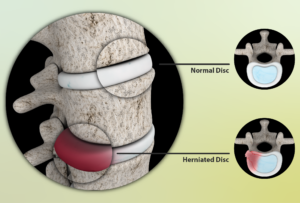
Degenerative disc disease is the most common cause of the gradual wear and tear that leads to pain.
The aging process makes the discs lose some water content, making them less flexible, more vulnerable to tearing or even rupturing — very painful. A minor twist or strain can be all it takes.
Most patients are not able to pinpoint a time and event that caused the herniation.
But some indeed recall an acute event, such as trying to move a heavy item.
Being overweight or lack of physical fitness are risk factors to a disc herniation.
So is an occupation that involves lots of lifting or twisting, along with a genetic predisposition.
Dr. Onesti is a board certified neurosurgeon specializing in spine surgery and surgical treatment of chronic pain. He has published many articles in peer-reviewed journals and has given numerous presentations at local and national meetings.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes

Safety of Chiropractic Manipulation on a Herniated Disc

Find out the truth about chiropractic manipulation on a herniated disc in the low back.
Some people are scared to see a chiropractor regarding their herniated (bulging) disc.
This is understandable, since many men and women believe that the only way to treat low back pain is with drugs, surgery, hot packs, cold packs, ergonomic chairs, physical therapy and avoidance of lifting more than 20 pounds.
Perhaps you’ve even heard that chiropractic work on someone with a lumbar herniated disc can be potentially harmful or risky. Well, let’s get to what the truth really is.
“Chiropractic treatments for patients with lumbar disk herniation are safe and effective,” says Stephen T. Onesti, MD, a neurosurgeon specializing in the spine, with Neurological Surgery P.C. of Long Island.
“I have often referred patients to chiropractors, and in my experience they have had excellent results.”
Why would a medical doctor deem chiropractic treatments risky?
Dr. Onesti says, “The risk of neurological or vascular injury due to chiropractic manipulation is basically only when it is applied to the cervical spine.” This is the neck area.
“Experience of the chiropractor is essential–a good chiropractor will not offer manipulation therapy when it’s contraindicated, and will perform it correctly when it is [indicated].
“It should be noted that chiropractors also perform many other type of therapy than just traditional manipulation.”
This includes the strategic use of hot and cold packs.
The Atlantic Spine Center is an example of a conventional treatment enterprise that endorses chiropractic treatment as an option for those suffering from herniated disc pain.
Their site states: When used in conjunction with standard or conventional care, complementary and alternative treatments, such as seeing a chiropractor for herniated disc treatment, can be beneficial to some people with a herniated disc.
Dr. Onesti is a board certified neurosurgeon specializing in spine surgery and surgical treatment of chronic pain. He has published many articles in peer-reviewed journals and has given numerous presentations at local and national meetings.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: atlanticspinecenter.com/spinehealth/conditions/herniated-disc/faq/

Melanoma Detection Technology Catches Cancer Super Early

Yes, there is technology that can catch melanoma very early — much earlier than what a dermatologist’s handheld scope can detect.
The waiting game with moles is over; you do not have to wait till a mole starts looking “scary” or “funny” to peg that spot as something needing medical evaluation.
An early detection program for melanoma goes way beyond simply examining your skin at home and having a dermatologist look it over in the exam room (which often takes only minutes).
“The importance of enrolling in an early detection program is to identify melanomas when they are shallow and have not metastasized, requiring only a simple incision or treatment,” says Richard Bezozo, MD, President of MoleSafe, the world’s most advanced melanoma screening program.
“To the naked eye early melanoma can be mistaken for a mole or lesion. The changes that occur with a melanoma may not be visible for some time.
“For people at high risk for melanoma it is essential that these lesions be identified as early as possible and that action be taken. The best available program for these people is MoleSafe.”
Serial digital dermoscopy is superior to a clinical exam by a dermatologist for detecting melanoma.
“The MoleSafe procedure utilizes a combination of high resolution dermoscopy imaging technology that uses painless, high intensity light to penetrate through the surface of the skin to show the structure of moles,” explains Dr. Bezozo.
“The results are digital, and in high resolution and are quickly interpreted by some of the world’s leading experts in dermoscopy.
“These experts flag hundreds of melanoma cases each year, compared to a dermatologist who will only see a handful.”
Who should undergo serial digital dermoscopy?
Though people at particular risk for melanoma should do this, the technology is open to anybody who wants to get a head start on the earliest melanoma detection.
I myself am in a serial digital dermoscopy program (have had my second imaging), and this gives me great peace of mind.
This technology is also ideal for people who simply cannot inspect their moles due to their location on the body.
Who’s especially at risk?
“The majority of people at risk include those with multiple moles (dysplastic nevus syndrome), people who have had more than one blistering sunburn, people who have had melanoma before, and people on an immunosuppressive agent,” says Dr. Bezozo.

Richard Bezozo, MD
There are more new cases yearly of skin cancer than breast, prostate, lung and colon cancers combined. The MoleSafe system produces high-resolution diagnostic images and creates a profile for your skin that’s monitored for any changes in moles.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: molesafe.com

Actinic Keratosis Prevention with Retin A ?

Actinic keratosis is a so-called precancerous lesion caused by sun damage.
Can these lesions be prevented with application of retin A?
Retin A is also known as retinoic acid.
To find out if retin A could have a preventive effect against actinic keratosis, I consulted with dermatologist Richard Bezozo, MD, President of MoleSafe, the world’s most advanced melanoma screening program.
Dr. Bezozo’s answer is: “No.”
Just what is actinic keratosis?
“AK is also known as solar keratosis,” says Dr. Bezozo.
“They are scaly crusty growths that develop slowly.
“Typically an eighth to one-fourth inch in size and caused by sun damage, AK indicates a risk for skin cancer.”
Actinic keratoses are extremely common in people over 40.

Actinic keratosis on the ear. Future FamDoc, CreativeCommons
Just what does “precancerous” mean for this condition?
Dr. Bezozo says, “Ten percent will advance to squamous cell cancer.”
However, you need to keep this information in the proper context:
The advancement occurs in 10 percent of untreated cases; and many times, a person fails to seek treatment — giving the lesion ample time to get worse.
Sometimes, the patient is unaware of the presence of a developing lesion (it may be, for instance, on their scalp).
Squamous cell carcinoma kills about 3,500 Americans a year and grows slowly, and many people just don’t realize something sinister has been slowly growing on their face, neck and other sun-exposed areas for a long time, and may shrug the lesions off as benign signs of aging skin.
Preventing Actinic Keratosis
Dr. Bezozo says: “Prevention techniques include using a broad spectrum UVA/UVB sun protection. By the time you get them the damage has been done. Retin A is typically used to treat acne.”
Though most patients are over 40, younger people are not immune to actinic keratoses.
Application of retin A may help manage other conditions, but this is not one of them.
Richard Bezozo, MD
There are more new cases yearly of skin cancer than breast, prostate, lung and colon cancers combined. The MoleSafe system produces high-resolution diagnostic images and creates a profile for your skin that’s monitored for any changes in moles.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Dermatology11

Melanoma Risk in Blondes Who Tan vs. Always Burn

Does melanoma risk differ in blondes who always tan and blondes who always burn?
If you’ve heard that blonde hair is a risk factor for melanoma, perhaps you’ve wondered about olive skinned people who have naturally blonde hair, or natural blondes who simply tan easily but don’t have olive skin.
“We do not segregate blondes who never tan as a particularly vulnerable group,” says Richard Bezozo, MD, President of MoleSafe, the world’s most advanced melanoma screening program.
“We discuss melanoma risk regarding fair skin individuals (people with freckles, light blonde or red hair and blue eyes as well). All of these people fall under the category of a Fitzpatrick 1.”
Dr. Bezozo explains, “Thomas Fitzpatrick was a Harvard dermatologist who came up with a scale in regards to individual’s skin types in 1975.
“It is a useful tool for identifying people at risk for various skin diseases, for example, how likely you are to get skin cancer.
“The scale can also be used by dermatologists to recommend facial treatments.”
Dr. Bezozo describes this system as follows:
Fitzpatrick 1- a person with light skin, light hair, blue eyes and who burns easily and often.
Fitzpatrick 3 – a person with cream white skin, fair with any eye or hair color who sometimes burns and gradually tans.
Fitzpatrick 6 – a person who is dark skinned and never or rarely burns.

Melanesian children. Their hair color is natural, due to a gene mutation in their population.
He adds, “The lighter the skin the more the damage from the sun’s rays. Since skin damage is cumulative, blondes who always burn (Fitzpatrick 1s) have a higher risk for melanoma.”
Dr. Bezozo says the following individuals should get early melanoma detection screening:

“Blondes who never tan and always burn, people who have had more than one blistering sunburn in their lifetime, people who have more than 10 moles, people with a family history of skin cancer, people who have previously had skin cancer or people with a weakened immune system.
“Light skinned people should also avoid excessive UV exposure (tanning beds).”
Richard Bezozo, MD
There are more new cases yearly of skin cancer than breast, prostate, lung and colon cancers combined. The MoleSafe system produces high-resolution diagnostic images and creates a profile for your skin that’s monitored for any changes in moles.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Stage 1 Melanoma Look Like a Normal Mole?

Learn more about stage 1 melanoma and its appearance.
It’s a smart question: Can stage 1 melanoma look like a normal (benign) mole?
“A stage 1 melanoma can look like a normal or featureless mole even to a trained naked eye,” says Richard Bezozo, MD, President of MoleSafe, the world’s most advanced melanoma screening program.
“The changes that occur with a melanoma may not be visible for some time.
“Stage 1 melanoma is when melanoma is in the outer layers of the skin and has not spread to lymph nodes.
“Stage 1 varies, but for melanomas that are less than 1 mm in depth the risk of metastasis is almost zero.”
Just because a stage 1 melanoma may look normal to the naked eye, doesn’t mean that it looks the same as it did a month ago.
This is why it is so vital to get to know your moles and other “spots” (and this includes where they’re not), so that you can tell if one’s been changing in appearance, or if a spot or “freckle” is brand new.
Sometimes a very tiny scab can pass for a “new” mole if its location prevents an up-close visual inspection by the patient.
It’s important to realize that a new spot or lesion isn’t necessarily a mole or malignant.
Dr. Bezozo says, “Dermoscopy as used in the MoleSafe program can identify melanomas in stage 1. Dermoscopy can reveal subtle changes to your skin that’s not visible to the naked eye.”
How does this skin cancer detection technology work?
“MoleSafe incorporates the total body photography, digital dermoscopy, serial monitoring and risk assessment procedures to diagnose melanoma at the earliest possible stage,” explains Dr. Bezozo.
“Using the system, a patient’s images can be evaluated by the dermoscopist (a dermatologist who specializes in reading dermoscopic images) quickly and effectively, often reducing the number of unnecessary biopsies.”
Richard Bezozo, MD
There are more new cases yearly of skin cancer than breast, prostate, lung and colon cancers combined. The MoleSafe system produces high-resolution diagnostic images and creates a profile for your skin that’s monitored for any changes in moles.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

How Common Is a Blue Melanoma?

Maybe you’ve heard that melanoma can be blue, but how often is this?
What is the answer to how common or often is a melanoma blue?
“Not common. They are rare, aggressive and often lethal,” says Richard Bezozo, MD, President of MoleSafe, the world’s most advanced melanoma screening program.
Dr. Bezozo adds, “They are also known as malignant blue nevus.”
A nevus (pronounced knee-vus) is the medical term for mole.
“These are melanomas arising in association with a blue nevus or those arising spontaneously in the skin which resemble a blue nevus,” he continues.
“If you see something new or changing on your skin, have it checked out by your dermatologist. Blue nevi tend to be large, 1-3 cm in diameter and they can be elevated or smooth.
“Typically they are greyish-blue to blueish-black. They are often solitary and can be found on your buttocks, your lower back, or your hands and feet. Still, they are very uncommon.”
A blue appearing mole isn’t necessarily a melanoma. In a benign mole of this color, the pigment cells are deeper in the skin.
“Often solitary” does not mean, however, that blue melanomas can never be clustered, as in the metastatic melanomas below.

Keep in mind that a condition such as this does not develop overnight.
- You should check the skin on your entire body on a monthly basis for anything that looks suspicious, including a new blue color to a previously brown mole.
- Get to know your moles so that if changes begin happening, you will be aware of this.
The patient pictured above obviously either failed to regularly examine their skin and thus was unaware of the changes in their skin early on, or, was aware of the ongoing development of all the blue lesions but failed to seek medical intervention.
Melanoma as it progresses eventually becomes visually alarming.
Richard Bezozo, MD


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}