

Causes of Dizziness While Eating in the Elderly

The probable cause of dizziness when an elderly person eats is related to the aging process, says a doctor.
Do you know of an elderly person who reports feeling dizzy when they eat (or shortly afterwards)?
Or perhaps you yourself, being over age 65, get a feeling of dizziness during a meal.
Eating should not make anybody feel dizzy or lightheaded.
What can cause this dizzy feeling while eating?
“I can see that happening in the elderly with poor head and brain circulation,” says Carolyn Dean, MD, ND – Medical Advisory Board Member of the non-profit Nutritional Magnesium Association at nutritionalmagnesium.org.
“Perhaps with carotid artery plaque. Then when they eat, blood is diverted to the stomach and less gets to the head and brain.”
Carotid artery plaque means “clogged” arteries, or a narrowed diameter of the interior of the arteries.
This means reduced blood flow to the brain. So when this blood flow is diverted due to the intake of food, this can be a tipping point as far as reduced blood flow to the brain — resulting in a funny feeling in the head.
With blood being diverted to the stomach to facilitate the digestive process, there’s less blood reaching the brain neurons in the elderly person.
This compounds the already-compromised circulation due to carotid artery disease.
Solutions to the dizziness?
Dr. Dean says, “First use high dose magnesium therapy and vitamin K2 to help dissolve the calcium in plaque before preceding with the standard therapy of surgical removal of carotid artery plaque.”
The best way to take a magnesium supplement, says Dr. Dean, is in powdered form, because it absorbs the best.
Magnesium aids with hundreds of functions in the body, and most people do not get enough of this mineral.
Powdered magnesium is readily sold online and at stores. It’s tasteless and mixes easily with water.
This is not the cure for carotid artery disease, but can be part of the overall management of the condition.
If your primary care physician is not able to tell you what can be causing a dizzy feeling when eating, you should see a cardiologist and inquire about carotid artery disease.

Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes

Morning Nose Crud: Causes & Solutions

Do you awaken every morning with your nose blocked up with hard goop or crud that can’t be blown out?
Even in the absence of a cold, a person can suffer from a blocked nose every single morning, and it can even interfere with the sense of smell and taste, and impair optimal oxygen flow through the nasal passages during breathing.
Causes of Morning Nose Gunk
Allergies can be a cause of a morning blocked nose, says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology. Allergies increase mucous production, blocking up the nose.
“This can be from poor nasal clearance, nasal blockage and nasal dryness,” says Dr. Silvers.
Chronic sinusitis can also be a culprit, causing greater mucus production overnight, leading to this most aggravating problem.
Solutions to a Morning Blocked Nose
Use a humidifier; this will moisten the bedroom air. By next morning, if you have any gunk up your nose, it should at least be softer and more easily blown out.
“Regular use of nasal rinses can prevent mucous buildup,” says Dr. Silvers. This is most effectively done with a neti pot, and this is sold at common drug stores.

Neti pot. Shutterstock/kavzov
“Use the neti pot with saline rinses designed just for irrigating the nose. If allergies are the cause then allergy medication can be helpful.”
Do not aggressively pick up through your nose to extract the hard mucus, as this can result in bleeding and possibly irritation to the nerves inside the nasal passages.
Too much irritation may even result in a headache.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/ReaLiia

Can Esophageal Spasms Come in Certain Patterns?

Find out the nature of esophageal spasms in terms of type of contraction…
Esophageal spasms are always of interest to those with health anxiety because they can cause severe chest pain.
And of course, chest pain really rattles those with heart health anxiety.
They may wonder what kind of different flavors such a spasm can present in.
Can esophageal spasms come in various patterns, waves or be interval-based?
“There are various patterns of abnormal esophageal contraction that are non-specific and include diffuse distributed throughout] esophageal spasm, hypertensive peristalsis or ‘nutcracker esophagus,’ and hypertensive lower esophageal sphincter,” says Steven Fleisher, MD, a gastroenterologist in Rosedale, Maryland, with 20+ years of experience.
“There is a disorder called achalasia in which the valve at the lower end of the esophagus, the lower esophageal sphincter, is almost permanently in spasm and relaxes poorly with swallowing.”
Can mental stress trigger an esophageal spasm?
Dr. Fleisher explains, “The relationship between stress and esophageal spasm is not clear.
“Indirectly, medications that are often helpful in these conditions include antidepressants, suggesting that stress does play a role.
“Furthermore, psychological symptoms are often associated with these disorders including anxiety and depression. Patients with these conditions often report feeling ‘stressed.’”
To calm your body from mental stress, get plenty of exercise.

Shutterstock/G-Stock Studio
Physical activity helps reduce stress hormones like cortisol and stimulates the production of endorphins, which are natural mood lifters.
Exercise also improves sleep, boosts self-esteem and provides a healthy distraction from daily worries.
Whether it’s a brisk walk, a workout at the gym or a yoga session, incorporating exercise into your routine can make a significant difference in how you handle stress.
You should work out hard to soothe a harried soul. Nothing does this quite like panting and sweat.
You should not consider housework as a form of structured exercise to combat stress, especially since cleaning the house often has a built-in component of stress to begin with.
Dr. Fleisher says that the best test for diagnosing a spasm of the esophagus — which can sometimes be very painful — is the esophageal motility study, “performed with a catheter inserted through the nose while the patient is awake and unsedated.
“It is seldom performed in clinical practice secondary to poor patient tolerance.”
 Dr. Fleisher was named a 2015-2018 “Top Doc” by Baltimore Magazine for gastroenterology.
Dr. Fleisher was named a 2015-2018 “Top Doc” by Baltimore Magazine for gastroenterology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/siam.pukkato

Why a Spin Class Can Cause Anal/Rectal Bleeding

A doctor explains why a spin class or similar can result in blood all over your panties from anal bleeding.
Have you ever gone to the restroom following a spin class, pulled down your underpants, only to nearly have your eyes pop out at what you saw—fresh blood smeared all over your underwear?
“Spin class or intense prolonged use of a stationary bike may cause anal bleeding through direct and indirect mechanisms,” explains Steven Fleisher, MD, a gastroenterologist in Rosedale, Maryland, with 20+ years of experience.
“Direct mechanisms would include irritation to the anal, and peri-anal skin through prolonged pressure, especially if one remained in the saddle for prolonged periods of time.”
Anal bleeding once happened to me.
It wasn’t a spin class, but I was on a stationary bike doing high intensity interval training.
By the time I was done, the bike had moved a few feet along the floor.
I hadn’t used a stationary bike for an extremely long period of time. I made a trip to the john, pulled down my white panties, and lo and behold…red blood stains all over the inner portion of the garment. I immediately connected the dots.
This is the only time I’d ever experienced anal bleeding from cycling, and I believe it was due to a combination of not having been on a stationary bike for a very long time, and the fact that this particular machine jostled quite a bit as I pedaled.
Prevention of Anal Bleeding from Cycling
Dr. Fleisher explains, “Here, using the correct apparel such as riding briefs with a chamois may be important.
“In addition, any pre-existing peri-anal conditions such as warts, or hemorrhoids, may be further inflamed, and bleed.
“Indirectly, prolonged sitting is one of the factors that predispose to hemorrhoid formation, which in turn may cause bleeding.
“There are several theories about how hemorrhoids actually form that include changes in tissue integrity, increased anal tone, and swelling of the hemorrhoidal cushions (veins).”
Dr. Fleisher was named a 2015-2018 “Top Doc” by Baltimore Magazine for gastroenterology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Does All Your Food Taste Fishy? Possible Causes

What could be the reason everything you eat tastes like fish?
More people than you think suffer with the problem of tasting something fishy every time they eat.
But what could make “everything you eat” have a fishy taste?
I posed this question to Carolyn Dean, MD, ND – Medical Advisory Board Member of the non-profit Nutritional Magnesium Association at nutritionalmagnesium.org.
Dr. Dean says this:
“I just know of this metabolic disorder. Fish odor syndrome (trimethylaminuria) is a rare metabolic disorder caused by a specific gene (FMO3) mutation.
“This gene mutation is caused by an autosomal recessive trait.
“It is estimated that approximately 1 percent of the population has this recessive trait, but it takes two copies of the gene to actually have the symptoms of the condition.
“If the mother and father both have one copy of the mutated gene, the child can develop the condition.
“This disorder is characterized by the inability to metabolize a compound (a byproduct of protein digestion) in the body called trimethyamine.
“As a result of this metabolic disorder, the breath, sweat and urine have a very strong odor of fish.”
If someone has this disorder, and much of the food they eat takes on a fishy flavor, it may be due to their trimethylaminuria – which they probably have not been diagnosed with, since it’s a rare condition.
On the other hand, it may very well be possible to experience a fishy taste in your foods when you don’t have this strange metabolic disorder.
See if you can rule out fish contamination when you prepare foods.
For instance, was a bowl that someone in the house used to make tuna salad thoroughly cleaned before you put your fruit salad in there?
If you can rule out fish contamination, it may be very enlightening to have a thorough workup with an ear, nose and throat doctor, as well as with a gastroenterologist.
Acid reflux can cause unpleasant persistent tastes in the mouth, which can affect the taste of food — and may even be perceived as “fishy.”
Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Fish Freepik.com, brgfx

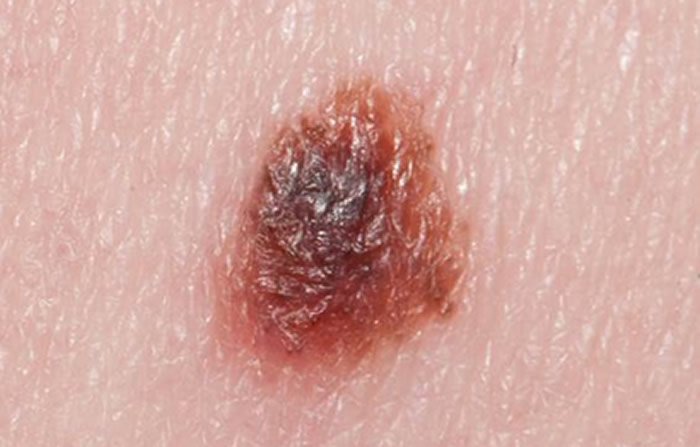
Can a TCA Peel off a Melanoma?

Find out if it’s possible for a TCA to peel off a melanoma…
You may be wondering if even the thinnest melanoma can be peeled off with a TCA treatment.
“Melanoma will not be affected by peeling since it’s within the second layer of the skin (dermis), and it would have to be surgically removed,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
But what about very early (superficial spreading) melanoma in the top layer of skin?
“Melanocytes reside between the basal layer of epidermis and superficial layer of dermis,” explains Dr. Gabriel.
“A peel [TCA] should never go that deep; otherwise, would cause a second-degree burn with exposed dermis.
“Peels take off the stratum corneum and maybe the second layer, but not any deeper (at least TCA used appropriately). So someone with melanoma, you can still see it after the peel.”
If you had brown spots prior to a TCA peel, and they’re still there, these aren’t necessarily melanoma.
Dr. Gabriel explains, “The brown spots (sun spots) are dead keratinocytes [a particular type of cell] that have the melanin pigment trapped in them.”
Simply put, the TCA procedure will not “peel off” a melanoma.
The cells of this cancer are pretty tough and will not budge from a cosmetic treatment.

Melanoma. Cancer.gov
If you suspect you might have a melanoma or other skin cancer on your face (or anywhere, for that matter), you should hold off on any TCA procedure and instead have your dermatologist inspect the suspicious spot.
Your doctor may decide to remove the spot and have it biopsied.
A complete removal includes the underside of the suspected melanoma, not just the portion that you can see.
Even if it’s removed strictly for cosmetic purposes, it still should undergo a biopsy — just to play safe!
 Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Causes of Piercing, Stabbing Chest Pain: Get to ER Fast

If you’ve been having ripping, stabbing or excruciating chest pain out of the blue, even if it comes and goes, get to the ER immediately.
You may have minutes to live…
“Stabbing or ripping chest pain always raises the specter of what we call ‘aortic dissection,’ says Dr. John A. Elefteriades, MD, William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
“Aortic dissection means internal tearing of the aorta, separating the inner from the outer layers of the aorta.”
It’s not hard to understand why many people die within minutes of an aortic dissection — the aorta is the body’s largest blood vessel.
Blood that’s pumped by the heart goes into the aorta to be distributed to the rest of the body.
This great blood vessel has several branches that lead out from it, through which blood flows, and this includes to the brain.
What is an aortic dissection?
“This is exactly a ripping apart of the layers of the aorta, just as the term implies,” says Dr. Elefteriades.
“This is a very serious condition that usually requires an immediate operation.”
This situation never goes away on its own; it’s a ripped blood vessel!
It only gets worse; the course of it will lead to death unless it is promptly treated—and treatment is always surgery.
Aortic dissection results in massive internal bleeding. Some patients will die within minutes, while others have delayed the ER visit, not realizing how serious their situation was, and because the dissection was of a slower nature, they survived despite delaying the ER visit by up to a few days.
A “slower” dissection, however, will ultimately lead to death if it is not surgically repaired.
So if you or someone you know has been complaining of agonizing or ripping chest pain, don’t wait another second in getting to the ER.

Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
,
Top image: Shutterstock/ Robert Kneschke

Intestinal Gas Bubbles: Sharp, Stabbing Rib Pain Explained

Here’s information on why gas bubbles in the intestines can cause so much pain, including in the rib area.
It can stop you dead in your tracks: sudden, stabbing pain in a specific region of your abdomen, and when it’s in the rib area, it can really take your breath away.
Why can a gas bubble in the intestines be so painful?
“Intestinal gas causes pain because of distension of the intestine,” says Michael Blume, MD, a gastroenterologist at MedStar Good Samaritan Hospital, Baltimore.
“When your intestinal wall becomes abnormally distended, this usually results in discomfort.
“It usually resolves when the distension resolves, mostly by either passing gas or belching, depending on where the distension is.”
Keep track of when this nasty symptom strikes you. You should become acutely aware that within a rather brief time from the onset of this symptom, you’ll start passing gas (or burping).
In fact, don’t be surprised if you have more flatulence than usual, or if it’s frequent over the next few hours or more.
Rib Pain
“Most of the time, intestinal gas is from swallowed air,” says Dr. Blume.
“One can get abdominal distension from structural or functional problems in the gastrointestinal tract.
“However, if one has significant abdominal distension, it can cause discomfort around the rib area as a result of this.”
 In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Anus Wax Buildup: Causes and Solutions

Find out what a doctor says about the causes of anus “wax” buildup…
Many people want to know what can cause a buildup of “wax” in their anus.
Now, what’s really interesting about this question is that what an individual perceives as a wax-like substance, in fact, isn’t wax at all.
Wax, like the type of substance that accumulates in the ears, does not accumulate in or near the anus.
What does a person actually see, then, or even feel, if it’s not similar to the wax that collects in the ears?
“If you mean passing mucous per rectum, these are usually normal secretions,” begins Michael Blume, MD, a gastroenterologist at MedStar Good Samaritan Hospital, Baltimore.
“Your colon normally secretes mucous to function as a lubricant for helping with bowel movements.
“When one’s colon becomes somewhat irritable for whatever reason, it often secretes more mucous, and one sees it in the stool.
“As a rule, it looks scarier than it actually is, and most of the time does not require specific intervention.”
As this mucous squirts out of the anus as you strain with a bowel movement, or even with an easy bowel movement, it may have a slimy feel to it as it passes through.
You look in the toilet and see white or whitish-clear gobs of something. Don’t panic; think lubricant. Let it be.
In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ANN PATCHANAN

Doctor Explains Cause of Chest Burning from Running

Find out why hard running causes a burning sensation in your chest.
What causes “burning” in the chest (or lungs) from running?
“From a digestive point of view, hard running may cause burning in the chest through various mechanisms,” begins Steven Fleisher, MD, a gastroenterologist in Rosedale, Maryland, with 20+ years of experience.
“Unfortunately, most research associating chest pain, burning or discomfort and exercise focus on the heart.
“And since the heart and the esophagus share a common nerve supply, distinguishing between cardiac and esophageal chest discomfort may prove difficult since exercise may provoke both.”
Nerve Involvement
“The sensation of ‘burning’ implies a nerve, or inflammatory (nerve irritation) cause of the pain.
“In my opinion, the following are the three most likely esophageal mechanistic causes of chest burning that may be exacerbated by hard running.”
#1. Reflux
“Gastroesophageal reflux tops the list and is responsible for causing chest discomfort in upwards of 30% of patients complaining of chest pain at baseline.
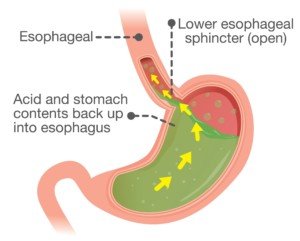
Acid reflux. Shutterstock/solar22
“Hard running after a large meal or eating while running may predispose to reflux and chest burning through mechanisms that include increased abdominal pressure associated with the respiratory effort of hard running, as well as the type of food consumed before or during running.
“Food types that are spicy or high in fat concentration may lower the pressure in the valve at the end of the esophagus and predispose to regurgitation, irritation and chest burning.
“Other factors promoting reflux include delayed emptying of the stomach secondary to reduced blood flow, impaired secretion of protective factors by the stomach and esophageal lining.”
#2. Esophageal Hypersensitivity
“Secondly, patients may have baseline esophageal hypersensitivity with lower threshold for esophageal burning in response to normal secretions; this may be exacerbated by exercise.”
#3. Dysmotility
“Thirdly, and more speculatively, hard running may induce abnormal contraction (dysmotility) of the esophagus that is often associated with chest discomfort.”
Other Causes
“Chest burning can also be associated with non-digestive causes including airway irritation particularly in cold weather, or when hard running is undertaken when not physically fit or accustomed to the respiratory effort associated.”
For some people, they may find that over time, as they improve their cardiovascular condition, the burning sensation in their chest (or lungs) will disappear.
Consistency with running is key.
Realize that you may become quite adapted to a particular cardio mode such as running fast on level courses or running up hills.
But then, for the first time in ages you decide to do “sprints” on an elliptical machine.
Don’t be surprised if this change in mode shocks your body and produces that chest or lung burning sensation.
Dr. Fleisher was named a 2015-2018 “Top Doc” by Baltimore Magazine for gastroenterology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}