

Aortic Aneurysm: Safe Weightlifting Techniques

Dr. Allen Stewart, aortic repair surgeon, comments on safe weightlifting techniques for people with aortic aneurysm.
Aortic aneurysm: safe weight lifting techniques – there are several.
When a fitness enthusiast is told he or she has an aortic aneurysm, the physician may warn the patient that it’s not safe to continue lifting weights.
Safe weightlifting techniques are mandatory.
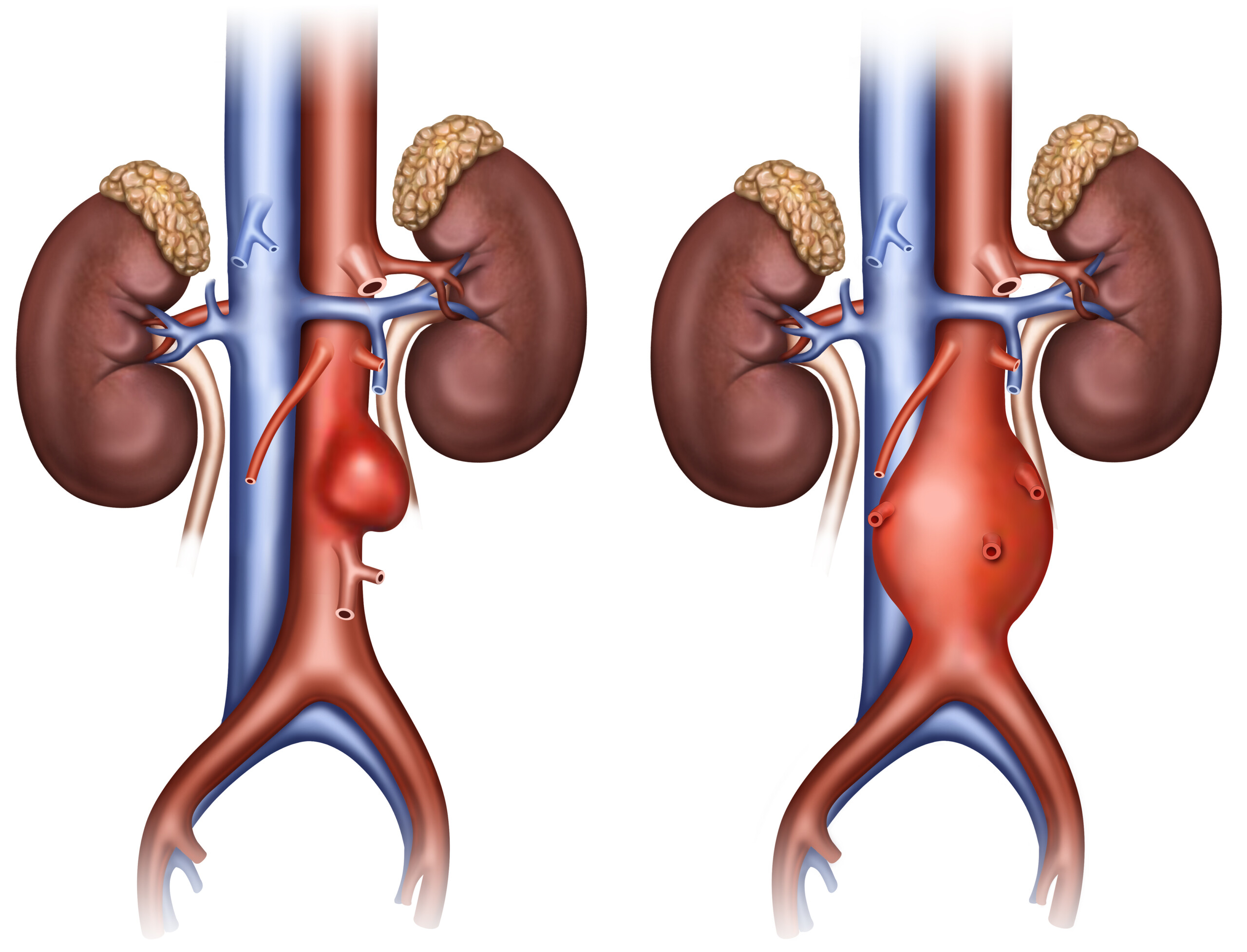
Lifting weights increases blood pressure. High blood pressure, even momentarily during lifting weights, can tear the already-weakened inner wall of the aneurysmal aorta, causing fatal internal hemorrhaging.
Safe strength training techniques include avoiding straining.
“Don’t lift heavy weights” is a common admonition for those with aortic aneurysm. But what does “heavy” mean? It’s all relative.
If bench pressing a 60-pound barbell is difficult, then this is heavy for you.
If you warm up with a 180-pound barbell to prepare for 300-pound bench presses, then 180 pounds is light for you (for this particular exercise).
Let’s look at a situation in which a man strains to complete 12 chin-ups. He begins with some effort, but past half-way, things get hairy.
He begins grunting at rep # 10. He barely cranks out the last rep: a 12 rep max with a compound exercise.
Safe weightlifting means no 12 (or fewer) rep maxes.
But what about percentage (of reps) of the 12 RM, using the same resistance?
This man is diagnosed with aortic aneurysm; would it be safe to stop at just half the reps of chin-ups?
Another example is a woman, newly diagnosed with aortic aneurysm, who normally does 12 RM Smith machine squats (135 pounds).
Thirteen reps are too difficult. How about if she just does around seven reps at 135 pounds?
“Yes, a percentage of maximal effort is a good way to look at exercise,” says Allan S. Stewart, MD, a cardiothoracic surgeon at HCA Florida Mercy Hospital in Coconut Grove.
Maximal effort is exactly that: With all your might, you cannot do one more repetition.
“The amount of recruitment of additional muscle groups is what causes the increase in catecholamine surge and consequently, the increase in blood pressure delivered to the weakened aorta,” continues Dr. Stewart.
“Working to failure is better accomplished with dumbbells than with a straight bar or with pull-ups (places where it is difficult to assess the strain mid-rep and also difficult to stop without a spotter).”

So what does this mean?
Dr. Stewart concludes: “It is much safer to exercise with specific muscle groups, lighten the weight, and work towards failure.”
There is “mechanical” failure and there is “metabolic” failure.
Mechanical: The weight can no longer be lifted because it becomes too heavy.
Metabolic: The athlete still has strength to continue lifting, but the muscle “burn” is so intense that another rep is impossible. This debilitating burn can be instigated with even a very light resistance load.

In the case of squats and other compound routines, many muscle groups are recruited, and at a 12 RM (and even more so with a 6-8 RM), there will be a surge in those catecholamines and hence a major blood pressure spike.
The resistance becomes too heavy to continue lifting, even though muscle “burn” may be minimal, if at all existent.
An athlete with aortic aneurysm that does not meet criteria for surgical repair, should do only around half the reps of his or her 12 RMs for compound routines.
For arm isolation work (e.g., dumbbell curls, triceps kickbacks, triceps rope), a 12 RM is fine.

Freepik/jcomp
Those with aortic aneurysm who want to complete 12 reps (or 10 or 8) with compound moves (exercises involving more than one joint) must then use 20-30 percent less resistance!
An aortic aneurysm, when it comes to lifting weights, means things will never be the same again – your safety is priority.
If your 12 RM bench press is 200 pounds, and you have aortic aneurysm, stop at six or seven reps with this load.
Or, do 12 reps at 140 to 160 pounds. Do not push through to true metabolic failure at this lighter weight, either.
Stop when you’re almost there. And don’t even handle the loads that would be for 10 or less RMs.
Another safe weightlifting technique for aortic aneurysm: avoid “super slow” or “negative” training. Move loads quickly to minimize time that blood pressure is high.
Best move: Convert to a 15-20 RM minimum. Dr. Stewart explains, “Reps cause failure of the muscle group more than higher weight, which necessitates recruitment of other muscles and more straining.
“I believe that higher reps with lesser weight is a safer option. Breathing is essential!!! Avoidance of Valsalva is important.”
It’s especially important for those with aortic aneurysm to exaggerate exhalation during the “positive” (concentric) portion of the lift, to prevent pressure-buildup in the thoracic cavity.
Inhale very deeply during the “negative” or release portion.

A pioneering aortic disease surgeon for 20+ years, Dr. Stewart has performed 5,000+ open heart surgeries and is the developer of a hybrid endovascular procedure for treating complex aortic aneurysms. In 2013 Dr. Stewart was recruited to lead the Center for Aortic Disease at Mount Sinai Hospital, later promoted to Associate Professor of Cardiovascular Surgery.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Following Aortic Aneurysm: CT Scan vs. Echo vs. MRI
A cardiologist gives imaging information about following an aortic aneurysm.
If you’ve been diagnosed with an aortic aneurysm, perhaps you’ve been wondering what is the most accurate imaging tool for which to “follow” it.
Whether your aortic aneurysm was picked up by a CT scan, echocardiogram or MRI, you’ve most likely been told by your doctor that serial imaging is in order (depending on size of the dilatation).
As for which imaging modality is best for serial following, the answer varies from one medical journal to the next.
“The most important factor is that at any particular institution where the patient is being followed with serial imaging, then one single modality (MRI, CT or echo) should be used for serial measurements,” explains Renee P. Bullock-Palmer, MD, a board certified cardiologist based in NJ.
If at all possible, make sure that the technician who is conducting the test is the same person every time.
Dr. Bullock-Palmer continues, “That being said, especially for younger patients where there is the associated risk of repeated radiation exposure, then a non-radiation type test is preferred, and thus MRI or TEE would be better than CT.”
TEE stands for transesophageal echocardiogram.
Transesophageal Echocardiogram
“TEE being more invasive in that this procedure is performed similar to an endoscopy, then MRI would be the preferred modality for serial imaging, particularly in the younger patient.”
If your aortic aneurysm was first detected by a CT or CAT scan, it’s important to have another, immediate scan via either MRI or TEE.
The reason is that sometimes, the interpretation of a CT reading is overestimated.
This happens when the slice of the aorta is done at an angle, or obliquely, rather than head-on, or, to put it another way, perpendicular to the curvature of the vessel, or to the linear dimension, in the case of the abdominal aorta.
If you’re having trouble visualizing this, then take a hand mirror that’s circular.
Catch the sun in it and cast the reflection of the sun on the wall. Move the mirror about and you can manipulate the shape of the reflection.
Angle the mirror in certain ways, and the reflection becomes more oval-like. Get a more head-on reflection and the shape is a circle.
The elongated reflection is akin to an overestimated reading of aortic diameter. An MRI or TEE will be more accurate as to true diameter.
The reading from a standard echocardiogram can also be overestimated, in that the interpreter may tack on one or two millimeters and conclude that the aortic aneurysm has “grown,” when in fact, it might still be the same size as it was the last time it was imaged.
Some people are afraid of MRIs, but remember, at least with an MRI, you will not be exposed to radiation.
MRI is highly sensitive, and the loud knocking noises, and length of test, are worth the more accurate reading of aortic aneurysm diameter.

Dr. Bullock-Palmer specializes in and has a passion for cardiac imaging as well as cardiovascular health of women.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
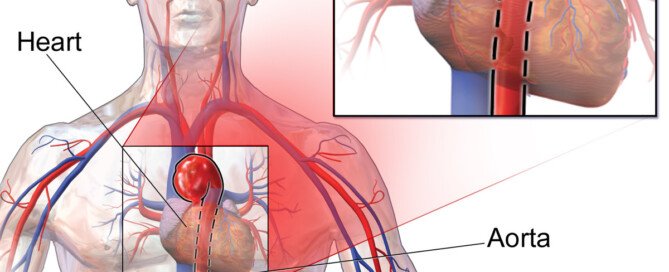
Top image: BruceBlaus/CC
Can Beta Blockers Shrink Abdominal Aortic Aneurysm?
A leading vascular surgeon discusses beta blockers can shrink an abdominal aortic aneurysm.
Many people with abdominal (and thoracic) aortic aneurysms wonder if taking beta blockers will shrink the bulge.
A beta blocker belongs to a class of drugs designed to lower high blood pressure.
Do beta blockers have a shrinking effect on an aortic aneurysm?
“With regards to beta blockers, there is no data that I am aware of that helps shrink abdominal aortic aneurysm,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“There is, however, data that indicates that AAAs expand at a slower rate in patients who are on beta blockers than those who are not.”
In general, an aortic aneurysm expands at the rate of 3 to 5 millimeters per year.
This doesn’t sound like a lot, but in aneurysmal terms, it’s very relevant.
When an abdominal aortic aneurysm reaches a minimum size, surgery is strongly recommended to repair the problem.
Until then, the patient practices “watchful waiting” which includes yearly scans, and blood pressure control, since higher blood pressure produces increased tension in the inner wall of the aorta – which can tear or rupture the aneurysm.
Dr. Gashti continues, “According to LaPlace’s law, arterial hypertension (high blood pressure) increases aortic wall tension and has been related to an increased rate of expansion and rupture.
“So since beta blockers lower blood pressure and the rate of the aortic pressure wave, they should inhibit AAA expansion and therefore rupture.”
An abdominal aortic aneurysm will never shrink spontaneously.
There are no known drugs that can produce a shrinking effect. The only means of repair are surgery or stent grafting.
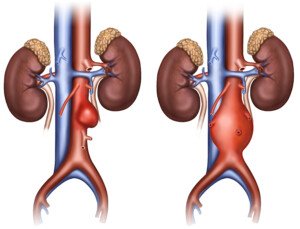
An AAA doesn’t necessarily keep getting bigger and bigger; some do remain small, but there is no way to tell if this will be the outcome; hence, the patient must maintain watchful waiting and regular imaging for life unless surgical repair is done — such as an endovascular graft as shown below.
Usually an abdominal aortic aneurysm does not cause symptoms, and most are detected by accident when the patient is being imaged for an unrelated issue.
A person can go his entire life with an AAA and never know it and live to a ripe old age.
Unfortunately, once one is discovered by accident, the knowledge of its existence changes things dramatically in that the patient now must make sure his blood pressure is consistently low, usually must take beta blockers to help ensure this, and must avoid heavy straining weightlifting.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
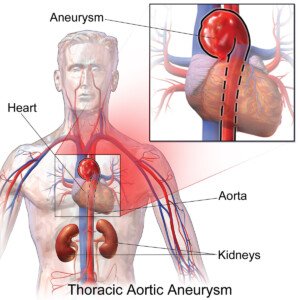
Top image: BruceBlaus

Can Lifting Weights Cause Aortic Dilatation (Enlargement)?

A vascular surgeon who performs aortic repairs answers if weightlifting can cause aortic dilatation.
“With regard to aortic dilatation in athletes, these kind of exercises (lifting weights) do in fact, over a long period of time, result in a compensatory dilatation of vessels, including the aorta,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
When an athlete, particularly one who does weight lifting, learns he has an enlarged or dilated aorta, his first instinct might be to conclude that working out caused this, and that it’s a good thing, not a bad thing.
Unfortunately, aortic dilatation in the truest sense is a crushing blow to a person who lifts weights.
The diagnosis of pathological dilatation (dilation or enlargement) isn’t always determined by just one reading off of one slice of the great vessel.
A more definitive imaging test may detect a smaller diameter, and reveal that the measurement, when taken in context with the entire aorta, actually shows a normal structure.
An athlete, upon learning that a slice of his aorta is at the upper limits of normal, or borderline aneurysmal in terms of centimeter measurement, wants to know if exercise can lead to this as part of a remodeling of the vessel as it adapts to greater cardiac output.
Dr. Gashti explains that the compensatory dilatation of the aorta comes about from “the need for increase in supply of blood to the exercising tissues/organs.
“For example, a patient who is being scheduled for creation of an arteriovenous fistula (artificial connection between artery and vein) for hemodialysis (machine-filtering of waste from blood), is told to exercise the intended arm so that when the time comes for surgery, the vein and the artery are larger and therefore they would have a better fistula.”
Aortic dilatation is a rather broad term, and indeed, it can refer to an aneurysm.
In the event of exercise-induced enlargement, Dr. Gashti says, “But the dilatation in this situation would be diffuse rather than focal, such as an aortic abdominal aneurysm.”
“Diffuse” means evenly distributed; in terms of the aorta, this would mean enlargement that’s uniform, as though it’s simply part of the vessel – a scaled up vessel, you might say, but still with normal proportions or dimensions.
“Diffuse dilatation of a vessel is immuned from the pressures that may lead to rupture, and therefore are generally of no concern,” says Dr. Gashti.
“Focal” means an isolated section of the aorta that’s enlarged. It appears bulging on an imaging test.
It can also appear sac-like, maybe even on just one side of the vessel. In short, the overall picture looks abnormal.
The diameter dimensions along various slices do not follow a normal pattern of increase and decrease.
“There is actually a condition called “arteriomegally” that describes this diffuse dilatation of vessels with no significant sequelae,” adds Dr. Gashti.
The bottom line is that there is no evidence that lifting weights can cause an aortic aneurysm, which, by definition, is a pathological process.
However, exercise indeed can cause a diffuse enlargement that does not result in any abnormal dimensions or weak vessel walls, and the athlete thus has no restrictions on activity.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
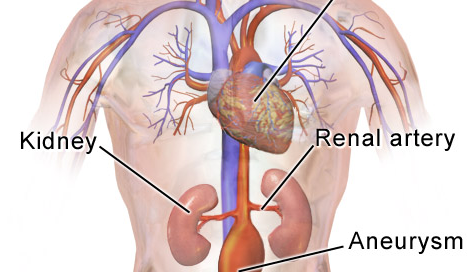
Top image: Depositphotos.com

Abdominal Aortic Aneurysm: Endovascular vs. Surgical Repair
In plain English, here are the pros and cons of endovascular vs. open repair of abdominal aortic aneurysms, described by a vascular surgeon.
This article describes in plain English endovascular vs. surgical repair of abdominal aortic aneurysms.
From an intuitive standpoint, it seems as though endovascular repair of an abdominal aortic aneurysm would have far greater benefits than invasive, open surgery, including increased survival rate and decreased risk of infection, stroke and cardiac arrest.
“I do not believe that any vascular surgeon that performs EVAR (endovascular aortic repair), would offer this procedure to a younger, relatively healthy individual – one who is able to do bench presses or weight lift,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Dr. Gashti points out that if he himself had an abdominal aortic aneurysm, he’d opt for the open technique, given that his current state of health is otherwise good, and he also says that the open technique is the preferred method among the physicians who invented this procedure, if they too, had the condition. The world’s first EVAR was performed in Russia in 1987.
Dr. Gashti continues, “You have to realize that EVAR was originally thought of because we had patients with large abdominal aortic aneurysms but with significant co-morbidities which made them very poor surgical candidates.”
A co-morbidity is an additional ailment that has the potential to complicate a surgery beyond what are the normally-established complications.
For example, a co-morbidity might be poor kidney function. Open surgery on someone with impaired kidneys dramatically increases risk of life-threatening complications.
“So we told them to go home and hope that the abdominal aortic aneurysm did not rupture. Endovascular repair provided an alternative to this option for this group of patients,” explains Dr. Gashti.
Today, about 75 percent of abdominal aortic aneurysms are repaired via endovascular. Most patients are men over age 70.
Dr. Gashti continues, “But one has to realize that, yes, it is true that this is a very minimally invasive procedure, initially, but the rate of re-operation for things such as endoleak, migration, device separation, thrombosis, fracture, etc., is much, much higher than the traditional open repair.”
An endoleak refers to leaking blood. Migration refers to shift in position of the stent graft. Device separation means the stent separating from the aortic wall; “This is when different pieces of the stent graft separate from one another,” says Dr. Gashti. Thrombosis means blood clot.
He adds, “When I repair an abdominal aortic aneurysm openly, I do not image their abdomen for at least five years post-surgery, because there is no reason to do so. These procedures (surgical) have been proven to be very durable.
On the other hand, a patient post-EVAR needs a CAT scan of abdominal (abdomen)/pelvis with IV contrast (dye) every three to six months for the first two to three years, and every year after that for the rest of their lives; that is if everything is okay.”
Picture the hassle of all of these imaging tests, not to mention the anxiety of worrying that the next test might show a leak.
“Just imagine the amount of radiation and cost that is involved,” continues Dr. Gashti.
“This is because we still do not know what the long-term results of endovascular repair are.
“So for a younger individual – younger than 60-65, with a smaller aneurysm who wants to be active with isometric exercise, I think that it would be reasonable to consider repair, but only via open technique.”
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
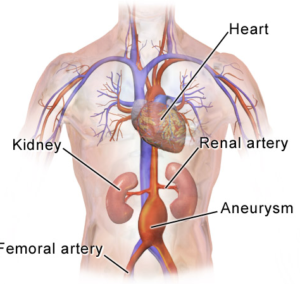
Top image: Shutterstock/ilusmedical
Source: ctsnet.org/portals/endovascular/procedures101/exp_tech.html

Why Can’t Stent Grafts Repair Ascending Aortic Aneurysm?

A vascular surgeon explains the reasons why stent grafts are not the solution for ascending aortic aneurysms.
Perhaps you already know that stent graft repair of descending and abdominal aortic aneurysm is the repair procedure of choice for select patients.
I didn’t understand, then, why stent graft repair was apparently impossible with an aneurysm of the ascending aorta.
I thought maybe it had something to do with not being able to “feed” the catheter over the arch of this great vessel. Well, that’s hardly the reason.
Stent graft repair is also known as endovascular repair. The issue with “endo stenting” of the ascending portion of the aorta is the length of this section; it’s too short, says Seyed-Mojtaba (Moji) Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Endovascular repair of the ascending aorta, to my surprise, is actually being done, says Dr. Gashti, but only for select patients, mostly at the Arizona Heart Institute.
He explains, “For endo stenting to work, you have to have adequate ‘landing zones.’ What this means is that you have to have ‘normal’ aorta both proximal and distal to the diseased (aneurysmal) area so that you get a good seal.”
Proximal and distal mean, in layman’s terms, on both ends of the aneurysm.
Without that good seal, a leak (called an endoleak) will occur, and the aneurysm will continue to be pressurized: a bad thing.
Dr. Gashti explains, that when he does a “TEVAR or EVAR (endo graft for thoracic aortic aneurysm and abdominal aortic aneurysm), a minimum of 20 millimeters of normal aorta is needed both proximal and distal to the aneurysm,” meaning, on either side.
The portion of the aorta that’s inside the heart is called the root. Attached to this area are the coronary arteries that feed blood to the heart.
These coronary arteries are the first branches (closest to the heart itself) of the ascending portion of this great vessel.
These first branches absolutely cannot be covered by the stent graft. After all, the stents are covered-type stents, not the bare metal type.
At the other “end” of the ascending aorta (the distal end) are branch-offs, or takeoffs, of the subclavian and carotid arteries.
Dr. Gashti says you certainly don’t want these to get covered by stent material, either.
“So by the time you add the landing zones and branches, not much room is left,” he says.
If you can visualize this scenario, it’s easy to see why stent grafting just won’t work for ascending aortic aneurysms — elongated aneurysms, that is.
“But for very focal aneurysms and particularly if they are saccular rather than fusiform, it is being done.”
- Fusiform is an elongated, more uniform bulge all around the great vessel’s circumference.
- A saccular bulge looks like a sack protruding from one side of the vessel.
Saccular can also mean a protrusion of short width encircling the vessel — imagine an expandable rubber tube the diameter of a dime, but at some point five nickels are stacked together inside it; imagine the shape this would cause to the tube.
Dr. Gashti continues, “The other problem is the aortic pressures that you have to deal with at the time of deployment — so close to the left ventricle — which will push your device away from the intended location; so these procedures usually require cardiac arrest at the time of deployment.”
In other words, the heart must be stopped for the surgeon to position the stent, and this means use of a heart-lung machine (cardiopulmonary bypass).
So now you know why stent grafting, as of 2014 when this article was published, is not a practical option for the repair of an ascending aortic aneurysm.
Update As of 2025: Stent Grafting in the Ascending Portion
- Stent grafts can be done in the ascending portion for an aortic aneurysm.
- However, stent placement here is complex and still in the experimental realm.
- The procedure is usually reserved for high-risk patients.
- The procedure involves a very customized, fenestrated or branched stent graft — and “debranching” of major arteries may be required. These arteries supply blood to the brain and arms.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rocketclips, Inc.

Can Exercise Lower the Risk of an Aortic Aneurysm?

If you do not do consistent structured exercise, your risk of developing an aortic aneurysm, when all other things are equal, is higher than if you were to stick to a regular exercise regimen.
Here is what a vascular surgeon says about exercise and lowering the risk of an aortic aneurysm…but first, I want to point out what I’ve read on medhelp.org.
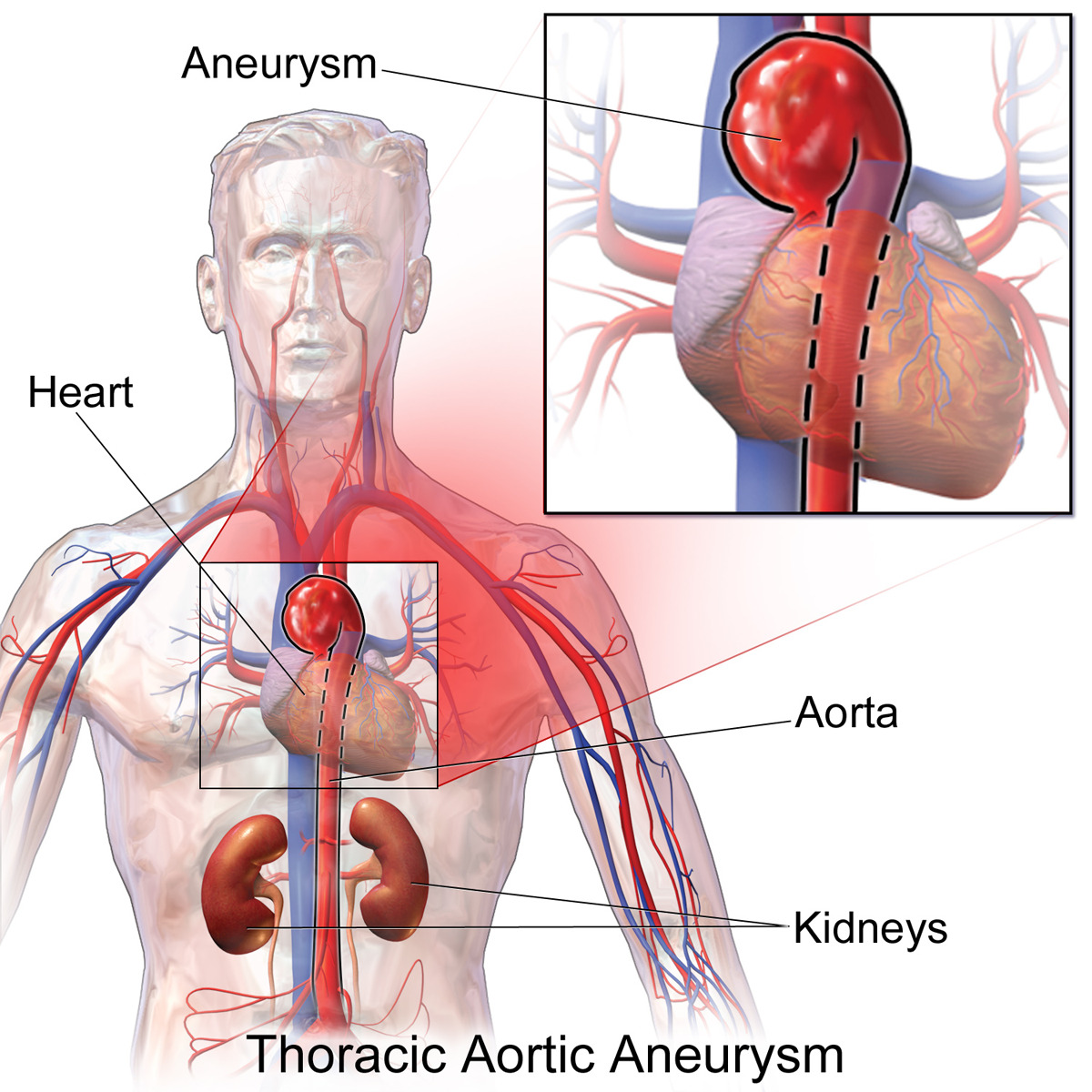
I have read about athletes being diagnosed with thoracic aortic aneurysm – these are people in their 20s to 50s who have led active lives, including jogging or cycling, and lifting weights.
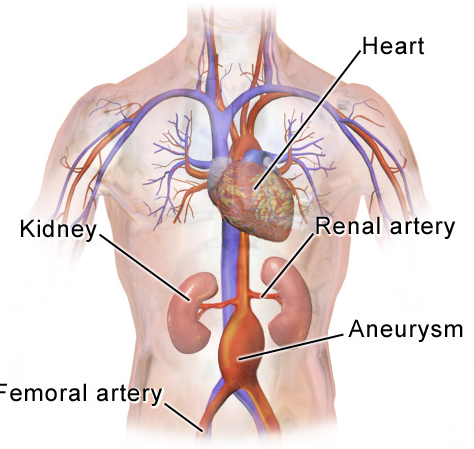
They are then diagnosed with a thoracic aortic aneurysm – a bulge or dilation in the aorta – as a result of an imaging test that was performed for an unrelated reason.
Nevertheless, can exercise actually help lower the risk of ever getting an aortic aneurysm in the first place?
“It is well-established that because exercise increases shear stress and promotes removal of lipid (fat) molecules from the luminal surface of the aorta – by increasing nitric oxide and prostacyclin (fat molecule) release – that it both directly and indirectly inhibits atherosclerotic processes and helps in both reducing one’s systemic blood pressure and risk of developing aneurysms,” explains Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Atherosclerotic processes refer to progressive plaque buildup in the arteries — in this case, coronary.
What kind of exercise is most useful in lowering the risk of developing an aortic aneurysm?
This question mostly applies to people who do not have genetically predisposing conditions to aortic aneurysm, such as Marfan’s syndrome.
First of all, you should know that two risk factors for aortic aneurysm are high blood pressure and atherosclerosis. Plaque buildup damages the inner lining of blood vessels.
By preventing these two variables (high blood pressure and plaque buildup) from occurring, this will reduce a person’s risk of developing an aortic aneurysm.
What better way to control these variables than to exercise?
The issue then become what is the best type of exercise.
In people with normal aortic size and dimension, there are no restrictions with weightlifting workouts or aerobic activity.
A well-rounded fitness/exercise regimen should involve strength training or lifting weights (e.g., barbell, kettlebell, machine, body-weight), aerobic workouts and something extra — such as yoga or tai chi.

However, no studies have been done to determine specifically what type of activity (e.g., swimming, running, hiking, Pilates, general strength training, body-weight training, group fitness classes, martial arts, pedaling) is the best at lowering the risk of developing an aortic aneurysm.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Iam_Anupong

Aortic Aneurysm & Blood Pressure: Is Losing Temper Safe?

A vascular surgeon comments on aortic aneurysm, and losing one’s temper and blood pressure rise.
According to one investigation, there is a strong link between aortic dissection (from pre-existing aneurysm) and extreme emotional stress—which would include a temper outburst.
A temper outburst would cause blood pressure rise. Blood pressure control is extremely important for people with an aortic aneurysm.
Patients are told to avoid heavy physical exertion such as heavy weightlifting or trying to install an air conditioner, as these can shoot up blood pressure, which can then cause conditions ripe for an aortic dissection.
Emotional stress, too, can raise blood pressure. Dr. John Elefteriades, an aortic repair surgeon, designed a survey of dissection patients.
Ninety responded regarding what they were doing right before the dissection occurred.
Thirty-six (40 percent) reported events that he categorized as severe emotional stress. Though this apparently is the only study of this kind, the results can’t be ignored.
Is it coincidence that 40 percent (although 90 is a very small number for a study) reported emotional stress (which of course is associated with high blood pressure)?
Must people with aortic aneurysms go through life tip-toeing on egg shells, suppressing their emotions, battling urges to vent their feelings about things in life?
“Losing one’s temper would increase the blood pressure and may result in aortic dissection in an individual with predisposing condition (medial cystic necrosis), but the effect on wall tension in an aortic abdominal aneurysm would most likely be negligible,” explains Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
So what does all this mean, then, as far as unleashing emotions?
“Not to say that you should go ahead and get angry all the time, but it is okay to get excited about your football team every now and then,” says Dr. Gashti.
Stress is a risk factor for high blood pressure (also known as hypertension), and that acute (sudden) stress can cause a dramatic rise, though it’s a temporary rise.
However, the transient nature of it can still have a devastating effect on a severely weakened aortic wall.
In fact, chronic hypertension can actually cause the aneurysm in the first place.
Hypertension even for people with healthy aortas can become a very serious, even life threatening condition.
It’s a powerful risk factor for stroke and heart disease, plus dementia and other major conditions.
What is medial cystic necrosis? This refers to a variety of metabolic conditions that affect the composition and structure of the middle layer of an aortic wall, says Dr. Gashti, by altering collagen, elastin, etc. This is seen in connective tissue disorders like Marfan’s syndrome, he points out.
He adds: “The most common consequence of this is aortic dissection; more than 90% of deaths in this group is related to aortic dissection, rupture, and sudden death.
“Aneurysms can also form in patients with this condition, but the incidence of that is low.”
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: ncbi.nlm.nih.gov/pubmed/17950810

Aortic Aneurysm & Lifting Weights: Research Scarce

A vascular surgeon discusses the obscurity of research involving lifting weights with an aortic aneurysm.
The restrictions for lifting weights in people with an aortic aneurysm are, quite literally, all over the map.
It’s like a bell curve: Most doctors urge their patients with aortic aneurysm to lift no more than 25-50 pounds.
On one end of the bell curve are physicians who urge against just about ANY kind of lifting, meaning men should not lift more than 10 pounds, and women should not lift more than 5 pounds.
Think of how much these restrictions would disrupt a person’s life; being warned by their doctor to avoid carrying their own babies!
This means a woman with an aortic aneurysm should not lift her baby from a crib!
What if nobody else is there to pick the baby up? What if nobody is there to put her baby, let alone a heavier toddler, in the car seat?
The other extreme are doctors who warn against straining with heavy weights, but tell their patients with aortic aneurysm they can continue working out – just don’t bear down to the point of having to grunt and moan.
As a personal trainer with an interest in medicine, I dug very deep into this issue and came up with very little research.
“As far as hardcore data on what the weight limit should be for an individual with known thoracic aortic aneurysm or abdominal aortic aneurysm, I am not aware of any,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“It is well-documented that aerobic exercise will actually decrease the systemic blood pressure.
“However, exercise such as weight lifting, if done repeatedly in succession, actually causes significant increase in systemic BP.”
As a person progresses further into a weight set, blood pressure increases.
Pushing out those last few reps means that blood pressure is its highest, and the exercises that cause the highest blood pressure increase, when done with heavy resistance, are the deadlift, barbell squat, hack squat and leg press.

Freepik.com, pressfoto
Dr. Gasthi continues, “I believe that most of these recommendations are therefore at best conjecture and perhaps minimally common sense.”
Lifting Weights on the Job and Aortic Aneurysm
Weightlifting gyms across America are filled with people every day, yet one doesn’t hear about aortic dissections occurring left and right at gyms.
About 200,000 people every year are diagnosed with abdominal aortic aneurysms, and about 30,000 with thoracic aortic aneurysms.
So where are all the dissections that you’d think be brought on by lifting weights?

Yes, a statistically significant percentage of these diagnoses are in people under age 50, and more and more people over age 60 are hitting gyms as well.
Further, millions of people every day do heavy hoisting on the job. Where are all the dissections?
Dr. Gashti explains, “I think that 50 pounds,” including for people who lift on the job, “is not very much, but if you have a 7 cm AAA, you should probably not be lifting more than that.
“But if you have a 3.5 cm AAA, I normally tell my patients to go about their lives normally and am yet to regret these recommendations.”
Research on lifting weights with aortic aneurysm is scarce.
“I am not aware of any randomized controlled trials that have looked into these issues,” says Dr. Gashti.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Kiselev Andrey Valerevich

Aortic Aneurysm: Are Deadlifts Safe to Do?

Dr. John Elefteriades, leading aortic disease surgeon, weighs in on the danger of deadlifts in people with an aneurysm of the aorta.
Though most aortic aneurysms affect older people, younger adults can be diagnosed with an aortic aneurysm, and older adults do lift weights for fitness and strength gains.
Thus, it is perfectly logical to wonder just how dangerous the deadlift is for a person with an aortic aneurysm.
Dr. Elefteriades is a weightlifter and also is William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
Dr. Elefteriades refers to the deadlift as a “dangerous exercise” for a person with an aortic aneurysm.
The deadlift is especially dangerous because it requires the use of so many muscles.
Thus, at heavy weights (relative to the athlete’s strength, of course), this exercise has the potential to cause a rapid, extremely high increase in intrathoracic pressure.
Can a person, with aortic aneurysm, do deadlifts at a non-heavy weight?
After all, a deadlift refers to a type of joint motion, not to an amount of weight lifted. You can do a deadlift with a broom stick.
Dr. Elefteriades advises that an athlete with an aortic aneurysm limit a deadlift to just one-half his body weight.
As a former certified personal trainer, I’m initially thinking of the concept of half one’s body weight.
Suppose a new client of mine weighs 405 pounds: a morbidly obese person. This person has an aortic aneurysm less than 5 cm and not meeting surgical repair criteria.
According to the half body weight rule, this client gets to do deadlifts with a 200 pound barbell.
He won’t be able to at first, but according to the half body weight rule, it’s a safe goal to work towards.
Now suppose I get another client who’s been training for years and weighs 180 pounds, but is solid muscle.
He hires me to help him lose 10 pounds of body fat for a more chiseled appearance, and he’s so strong he warms up with a 200 pound deadlift.
Then he learns he has an aortic aneurysm (under 5 cm) after having a routine coronary calcium score test.
According to the half body weight rule, that 200 pound deadlift warmup is very off-limits, even though it’s easy for him to do.
Meanwhile, my 405-pound client, over time, has worked his way up to eight repetitions with 200 pounds — and he strains with every rep, barely completing the eighth one.
The 180-pound guy, because of his light body weight, gets “punished” for being only 180 pounds by the half body weight rule, being limited to just a 90-pound barbell: a total insult.
Something really doesn’t sound right here, because there would be significantly more intrathoracic strain (and hence a blood pressure spike), in the 405-pounder as he strains, struggles and grunts his way through eight reps at 200 pounds in the deadlift.
Whereas for the 180-pound man, a 200 pound deadlift would be a walk in the park, and hence, very little blood pressure increase.
So rather than a half body weight rule for aortic aneurysm, I wondered about a “no straining” rule that is based on subjective experience, rather than a numerical value.
Dr. Elefteriades explains, “The half body weight rule is for the average individual. There will be a moderate amount of strain for the amateur bench pressing half his weight.”
Though this article is about the deadlift, Dr. Elefteriades’ response applies to any major compound weightlifting exercise.

He continues, “A trained athlete can lift more to achieve a similar amount of strain.”
My 180-pound client might have to deadlift 300 pounds (1.6 times his body weight!) to experience the same degree of straining as my 405-pound client.
Dr. Elefteriades continues, “However, trained competitive bodybuilders achieve the highest aortic pressures ever recorded—up to 380 mmHg—normal is 120 mmHg.”
Even the sickest patients in hospital cardiac care don’t have blood pressures this high.
He adds, “We just advise prorating other exercises to the same perceived strain as with bench pressing 50 percent of body weight.”
The smaller the muscle group worked, continues Dr. Elefteriades, such as in triceps push-downs, the less strain even with max efforts, and hence, the less of a blood pressure rise, when compared to big compound movements like the deadlift, barbell squat and, of course, bench press.
So when it comes to the deadlift and aortic aneurysm, what’s the final verdict?
Well, suppose I get a third client; he too weighs 180 pounds but he’s not as strong as the other lightweight guy, but he’s been training for a while nonetheless and strains to deadlift 160 pounds eight times.
He’s just been diagnosed with aortic aneurysm; the 160-pound deadlift sets are over.
However, he easily knocks off a set of eight deadlifts at 115 pounds. No straining whatsoever. He whips through these quickly without a reduction in tempo.
According to the “no straining” rule, this is safe for him. For the other lightweight guy, a comparable easiness of effort is achieved at 200 pounds—making that safe for him.

Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}