

Raising Ejection Fraction: Exercise & Other Lifestyle Changes

How effective can exercise be at raising ejection fraction?
What else can raise ejection fraction other than exercise?
“There are some patient populations where ejection fraction is modestly increased with regular exercise,” says Norman E. Lepor, MD, cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
“The benefits in terms of quality of life and an increase in exercise tolerance are achieved by increasing skeletal muscle efficiency and lung function more than it will increase ejection fraction.”
Other Ways to Raise Ejection Fraction
“Increasing ejection fraction can be accomplished by avoiding potential cardiotoxic substances such as alcohol and tobacco,” says Dr. Lepor.
“Patients with reduced ejection fractions (cardiomyopathy) can also increase their ejection fractions through the use of medications such as beta blockers and aldosterone antagonists.”
Recommended Types of Exercise
“A mix of moderate aerobic exercise regimen (power walking, jogging, bicycling, swimming) and moderate isometric exercise (weight training for tone, not mass) are best to enhance muscle efficiency, lead to weight loss, reduce insulin resistance or tendency to develop diabetes and improve cholesterol levels.

Shutterstock/Interpass
“People with low ejection fractions from weak heart muscles are much more likely to increase their ejection fractions with exercise and medical therapies than those who have sustained permanent damage to heart muscle from myocardial infarctions or heart attacks.”
Can an elderly person increase ejection fraction with only exercise — NO drug therapy?
Dr. Lepor explains, “Exercise has been shown to increase ejection fractions in some patients, such as those who have had heart attacks who are in a cardiac rehab program.
“It would be very unusual for a patient who has a low ejection fraction to normalize with exercise alone.
“In cases where the cardiomyopathy is related to certain noxious compounds such as alcohol abuse, abstaining from alcohol use can lead in some cases to normalization of ejection fraction.
“One cannot expect someone with a very low ejection fraction to normalize without drug therapy and lifestyle modifications including exercise and smoking cessation
“It is very important to understand the precise cause of the mild CHF to know if it can be reversed with exercise.
“Common causes of CHF in this country include coronary artery disease, hypertension, valvular heart disease, viruses, alcohol.
“So ignoring treating the primary cause will limit the benefit from interventions such as exercise.”
How to Correctly Use a Treadmill for Exercise

Shutterstock/Credit: This Is Me
The first inclination for many new users of a treadmill, particularly elderly people, is to cling onto the front bar or side bars.
But think about what this really means: mimicking using a walker.
If you’re able bodied (don’t rely on a cane or walker), but then step onto a treadmill and hold on during your walking session, you are performing BELOW baseline walking ability. This will downgrade you, not upgrade you.
In the activities of daily living, a person with chronic heart failure but without mobility handicap will not hold onto anything for support while walking from point A to point B.
Sure, he or she may pause to catch their breath here and there, but actual mobility is not impaired. Hence, there is no need to hold onto a treadmill.
To hold onto a treadmill means to regress your ability to balance and to “unteach” your body in efficient walking.
Start out at a slow speed. It’s amazing how many older people will put a treadmill at its highest incline and the speed at a fast clip, then hold on tight and claim they’ll fall off if they don’t.
Use a zero or small incline and a SLOW speed, and do NOT hold on.
This is the only way to resemble actual walking.
Holding on can lead to repetitive stress injuries in the hips and shoulders, and can lead to forward posture.
Gradually build up your confidence by increasing the speed in small increments over time.
An arm swing burns more calories and is the natural way to walk — and this rule applies to people with low ejection fractions or chronic heart failure who want to employ exercise therapy.

Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com/yanalya

How Much Will Mild Chronic Heart Failure Affect Exercise?

Suppose a person has been exercising for years, but then gradually develops chronic heart failure.
How noticeable or rapid will the decline be in this person’s ability to exercise?
“The decline in function will depend on the pace and severity of the process that leads to a weak heart,” explains Norman E. Lepor, MD, cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
“Generally a patient with good cardiovascular fitness will tolerate a given amount of cardiac dysfunction than one who is in poor shape.”
What this means is that if we have two people, “A” and “B,” and “A” has been doing aerobic exercise for years, while “B” has been completely sedentary…then if both people begin developing congestive heart failure, it will be better tolerated in “A.”
Nevertheless, congestive heart failure would over time start manifesting itself to “A.”
Where will the uncharacteristic fatigue be most noticeable?
“Walking rapidly or on inclines,” says Dr. Lepor.
The progression of exercise-performance declination will be more rapid than what would normally occur from the aging process.
For example, suppose a woman has been hiking for many years, continuing to do this into her 60s and 70s.
But we can’t expect her to be as efficient in her 80s as she was in her 70s—simply due to the aging process.
There will be a natural decline in her cardiorespiratory efficacy—and she’ll notice that hiking the same mountain—the one she’s done for years—takes a bit longer, and/or requires more frequent or longer rests.
But the decline in cardiorespiratory fitness, from congestive heart failure, could also be subtle, says Dr. Lepor. It can be subtle enough to be misdiagnosed as asthma or chronic obstructive pulmonary disease, he says.
It will help to be very aware of exercise performance and capacity, and to note when you take time off from cardio exercise (due to foot injury, travel, schedule conflicts, the flu or some other non-cardiac reason).
After all, skipping aerobic workouts will result in a decline in cardiovascular function; this decline happens faster in older people.
However…the absence of congestive or chronic heart failure means that the older jogger, hiker, cyclist, hill-dasher, runner, etc., will bounce back and recover their previous stamina rather quickly (assuming that they haven’t missed so many training sessions that they’ve lost significant fitness).
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, pressfoto

How Low Can Ejection Fraction Be without Congestive HF?

Is it possible to have a really low ejection fraction and still not have congestive heart failure?
“There are two major types of congestive heart failure (CHF),” begins Norman E. Lepor, MD, cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
“Half of the patients with heart failure symptoms that include shortness of breath with exertion, easy fatigue, a decrease in exercise tolerance and lower extremity fluid accumulation (edema) have what we call preserved or normal ejection fraction due to stiff and thickened ventricular walls.
“This condition is seen in patients who have poorly treated chronic hypertension [high blood pressure] and/or coronary artery disease.
“The other half of patients with heart failure have abnormal ejection fractions or what is called systolic dysfunction.
Shutterstock/EstherQueen999
“There is wide variance in the threshold of ejection fractions in these types of heart failure patients, but one could expect symptoms to occur when the ejection fraction is less than 40 percent.”
How does patient’s level of fitness factor into this?
Dr. Lepor explains, “Fitness plays a pivotal role in developing symptoms of heart failure.
“In patients who exercise regularly and maintain good fitness, have muscles that are more efficient and need less oxygen and nutrition to function.
“Therefore the better fit one is, the less symptoms such as easy fatigue or exercise intolerance they would have at any level of ejection fraction reduction.”
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Green Apple

Can Heart Problems Cause Sudden Weight Gain?

The kind of weight gain that heart problems can cause is not the same that’s caused by eating too much.
In fact, weight gain from chronic heart failure has absolutely nothing to do with body fat.
“Heart failure can lead to weight gain due to fluid retention most likely seen in the lower extremities, though much fluid can accumulate in the abdomen as ascites or in the chest as pleural effusions,” says cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
In the lower extremities, the weight gain presents as swelling around the ankles and lower legs.

Shutterstock/Toa55
This fluid retention can extend higher up in the legs and affect the groin area.
A person with chronic heart failure (formerly more commonly referred to as “congestive” heart failure) can gain five pounds of fluid weight in a single night.
This is why people with chronic heart failure are instructed to weigh themselves first thing every morning — and never skip a morning.
Why this Heart Problem Causes Sudden Weight Gain
Though fluid retention can be caused by a variety of illnesses, chronic heart failure is a very common cause.
Fluid in the lungs is called a pleural effusion, and this will show up on a CT scan or X-ray.
Dr. Lepor says that this fluid retention in heart failure patients is treated with diuretics and salt (sodium) restriction.
The diuretics, such as Lasix, treat the symptom, not the underlying disease process.
Another name for the fluid retention or “swelling” is edema.
The fluid can cause, for instance, an increase of eight pounds over a period of just several days — despite the patient not changing their eating habits.
Men and women with chronic heart failure are urged to also document their weight every morning to see if there’s any unexplained weight gain from week to week, not just day to day.
Not all people with chronic heart failure develop the edema in their lower extremities.
For some, the sudden weight gain could be in their abdomen (ascites; pronounced uh-sight-eez) or the pleural effusion (excess fluid around the lungs).
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rocketclips, Inc.

Can Heart Bypass Surgery Prevent Congestive Heart Failure?

Are you wondering if coronary bypass surgery, aka CABG, can prevent the development of chronic heart failure?
- Heart failure may involve fluid buildup in the legs that needs to be controlled with medication.
- In other cases there is not an issue of fluid buildup, but the patient still needs to take great care to manage the condition.
Coronary Bypass Surgery Preventing Chronic Heart Failure?
“CABG and percutaneous interventions (angioplasty) can in some cases [sic] to preventing CHF in patients who have severe blockages in their coronary arteries that severely reduce blood flow and the delivery of oxygen and nutrition to heart cells by increasing blood flow,” explains Norman E. Lepor, MD, cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
Why can’t CABG prevent congestive heart failure in ALL the patients who undergo this heart procedure?
Dr. Lepor explains, “Patients who do not seem to benefit from CABG or angioplasties to prevent CHF include those with milder disease (fewer blockages, blockages that are not in critical areas such as the ‘widow maker’ and less severe blockages.”
The widow maker refers to the left main artery in the heart, which supplies the left anterior descending (LAD) artery and left circumflex artery. Sometimes, however, this term refers only to the LAD.
If a blockage occurs to the left main artery, a significant portion of heart muscle will be left without oxygen.
If not treated promptly, a victim can suffer a quick death.
Other Ways to Help Prevent Chronic Heart Failure from Developing
How often do you check your blood pressure? High blood pressure is a big risk factor for the development of chronic heart failure.
Ideally, you should check your blood pressure at least once a week, or as advised by your healthcare provider.
Consistent tracking helps manage and reduce the risk of developing chronic heart failure.
Do you smoke? Then quit. Yes, it should be that easy for anyone who knows just how dangerous tobacco is.
While quitting can be challenging, there are many resources available to help, such as support groups, medications and counseling.
It’s important to remember that every attempt to quit is a step towards better health.
Seeking professional advice can provide additional strategies and support.
Do you exercise? No, not housework or walking the poodle, but REAL exercise: structured aerobics and strength training workouts. Get moving.
These three tactics not only fight off chronic heart failure but they also help prevent the need for coronary bypass surgery.
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, peoplecreations
Can an MRA Detect Congestive Heart Failure?
An MRA (magnetic resonance angiogram) is often used to see if there’s anything wrong with the heart and associated structures.
If someone has an MRA, the report will include what the ejection fractions are for each ventricle.
This made me wonder if an MRA could detect and diagnose congestive heart failure, since I was thinking that a very low ejection fraction (such as under 35 percent) might mean CHF.
“MRI is the gold standard for determining ejection fraction,” says cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
MRI stands for magnetic resonance imaging, so the MRA is a type of MRI.
Dr. Lepor adds that MRI is an intrinsic three-dimensional imaging modality. He further explains, “Echocardiography [ultrasound] is the modality most commonly used to determine ejection fraction.
“CHF is a clinical diagnosis that is based on symptoms and biomarkers such as BNP levels. Remember, half of patients with CHF have preserved ejection fractions.”
What would be abnormal on the findings?
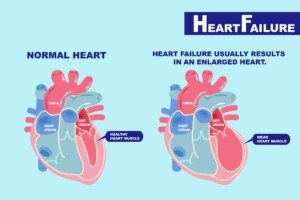
Dr. Lepor explains, “Finding on MRI or echo can include enlargement of the heart chamber sizes, reduced ejection fraction in some patients, thickening of ventricular muscle thickness, leaky or stenotic [narrowed] heart valves, abnormal estimated pulmonary artery pressures, abnormal blood flow patterns from the left atrium to the left ventricular consistent with either diastolic or systolic dysfunction.”
An MRA to show heart function is an expensive procedure and is not used to screen for congestive heart failure.
Instead, it’s ordered by a cardiologist as a diagnostic procedure after the doctor finds, during an examination, something concerning and wants to pursue the cause.
In addition to ejection fraction values and the possibility of congestive heart failure, an MRA will show other details that can help a cardiologist understand what’s going on with the patient’s heart, such as any abnormally enlarged structures.
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Green Apple

Statins vs. High Doses of Niacin: Why Not Take B3?

Why are statins pushed when instead, it seems that the safer route is to just take high doses of niacin (vitamin B3) to lower cholesterol?
You may have read that niacin or niacinamide has a positive effect on cholesterol profile, and that some cholesterol drugs are “knockoffs” of vitamin B3.
“Although most people think of niacin as just a vitamin, if you give it in high enough doses (the doses you need to budge cholesterol levels), it actually becomes a drug,” explains Dr. Elizabeth Klodas, board certified cardiologist and co-founder of Step One Foods.
She continues: “And drugs have side effects. High dose niacin can make blood sugar control worse in people with diabetes and prediabetes. It can cause flushing and itching [though non-flush versions are available].”
Okay, so what if you have great blood sugar levels and use the non-flush version of niacin?
“It can affect liver function,” says Dr. Klodas. “It can cause muscle achiness. And if you take a look at the medical literature as a whole, niacin does not appear to be that effective in improving patient outcomes.
“So even though it may lower cholesterol, the net benefit is more neutral for niacin than for statins.
“The benefit data behind statins is actually quite strong, especially in individuals with heart disease, those with diabetes and those with persistently very high LDL (bad) cholesterol levels (over 190 mg/dL).
“I only use high dose niacin as a second-tier therapy in those patients with known heart disease who cannot tolerate statins and don’t recommend them for diabetics.
“Because the benefit data for primary prevention with statins (taking them as a purely precautionary step) is less robust, I always try to work hard with my patients to address their cholesterol profiles with lifestyle changes, especially diet.”
Diet for Improving Cholesterol, Rather than Statins and Niacin
The key is not letting your cholesterol profile become undesirable in the first place.
“If you take in enough food-based fiber, omega-3 fatty acids, antioxidants and plant sterols (and I have to emphasize that these nutrients need to come from REAL FOOD in its REAL FORM to be effective), chances are high that your cholesterol profile will improve,” says Dr. Klodas.
“Because my patients found it hard to modify their diet to get these nutrients in adequate amounts, I created Step One Foods to make it easy.”
Don’t let your cholesterol reach a point where you must decide between statins and niacin; practice preventive medicine via the right diet.

Trained at Mayo Clinic and Johns Hopkins, Dr. Klodas believes in first changing the diet, rather than taking pills, to improve cholesterol profile.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sirtravelalot

Lower Bad Cholesterol, Raise Good Cholesterol with Supplements

Why settle for drugs when you can lower your bad cholesterol and raise good cholesterol with natural supplements, minus side effects?
Don’t be fooled by brilliant ad campaigns for drugs — drugs that are among the best selling in the world.
Natural Supplements for Improving your Cholesterol Profile
Fiber. “Soluble fiber does have an effect on cholesterol,” says Shana Spence, MS, RDN, CDN, a registered dietitian nutritionist based in New York.
“Foods like oats, beans, Brussels sprouts, apples and carrots are all examples.”
But if you don’t care for these foods, a fiber supplement will help.
“How soluble fiber works is that while it digests, it actually attaches to the ‘bad cholesterol’ or LDL and removes them from the body,” continues Spence.
“Insoluble fiber is the kind that our body cannot digest, like in the skin of vegetables and fruits or grains. Insoluble just keeps us regular and our gut healthy.”
Green tea extract. “Green tea contains catechins, which are antioxidants,” says Spence. “EGCG is the most potent type (and the one most people have heard of) that is found and also extracted.
“There have been studies that show this particular antioxidant does help to lower LDL levels or ‘bad cholesterol.’
“To get this benefit, it’s actually recommended to take the capsule form or use the extract rather than just drinking tea, since there is only about 50-100 mg of catechins in the tea itself and 145-3,000 in supplement form, depending on which brand you purchase.
“The only thing to be mindful of is the caffeine level. For those sensitive to caffeine or for those who are pregnant it’s best to speak to a doctor.”
Niacin (vitamin B3). Spence explains, “Niacin actually works to raise the HDL levels of ‘good cholesterol’ in the body while decreasing your levels of triglycerides (a type of fat known for contributing to cardiovascular diseases).”
Niacin also lowers the bad cholesterol (LDLs).
“What niacin does best is promote digestion and also aiding the nervous system,” says Spence.
“As for treatments, niacin is most commonly used in people who have high cholesterol but can’t take statins.”
Omega-3 fatty acids. The safest and most practical source of omega-3s is the fish oil supplement.
Pantethine (vitamin B5). “Studies for this vitamin are unfortunately scarce,” says Spence. “Yes, some people have reported taking this for their cholesterol.
“Like niacin, pantethine has been found to increase HDL and decrease LDL in some.
“One particular study [Rumberger et al, Nutrition Research, 2011] found that in addition to the TLC diet, pantethine significantly decreased total cholesterol and LDL levels.
“The TLC diet focuses on foods low in cholesterol and saturated fats.
“However, the study was only 16 weeks and done on women. There is still a definite need for studies to give a definite yes on this one.”
Plant sterols (PS). Though plant sterols are found in just about all plants, the amount isn’t sufficient to impact cholesterol levels. A person, even a vegetarian, must ingest PS in concentrated form (supplements).
“Taking in around 1,000 mg of plant sterols twice per day with food has been shown to lower LDL (bad) cholesterol by as much as 15%,” says Dr. Elizabeth Klodas, a board certified cardiologist.
“Step One Foods have 1,000 mg of phytosterols per serving – so you don’t have to worry about taking the supplement.”
Policosanol. Works like statins by inhibiting the liver’s ability to make cholesterol; lowers LDL and may raise HDL.
Red yeast extract. “Red yeast rice contains a compound that is structurally similar to statin medications,” says Dr. Klodas. She adds that red yeast extract can also cause the same side effects as statins.
Tocotrienols. These antioxidants are found in barley oils and rice bran, and inhibit the liver’s ability to manufacture cholesterol.
Turmeric. Supplements are best, for potency.
Note. Supplements are available that contain many of the above compounds in just one tablet or capsule.
 Shana Spence of The Nutrition Tea is committed to providing trending information and nutrition facts covering a wide range including nutrition for heart disease and diabetes, pediatric nutrition and healthful lifestyles.
Shana Spence of The Nutrition Tea is committed to providing trending information and nutrition facts covering a wide range including nutrition for heart disease and diabetes, pediatric nutrition and healthful lifestyles.
Trained at Mayo Clinic and Johns Hopkins, Dr. Klodas believes in first changing the diet, rather than taking pills, to improve cholesterol profile.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources:
webmd.com/cholesterol-management/side-effects-of-statin-drugs
webmd.com/cholesterol-management/guide/high_cholesterol_alternative-therapies
drcarolyndean.com/magnesium_miracle/
scholar.google.com/scholar?hl=en&q=turmeric+lowers+cholesterol&btnG=&as_sdt=1%2C6&as_sdtp=

Is Female Pattern Baldness the Same As Male Mechanism?

Is there actually a difference in the mechanism that causes hair loss in women when compared to that which causes male pattern baldness?
Well, they are not the same, but the mechanisms can be similar, says Dr. Robert Dorin, DO, NYC-based hair care expert and restoration specialist.
He explains that “there does appear to be other factors contributing to female pattern loss not found in men.
“Unfortunately, we do not know what it is, but clearly there are other factors at play.
“This is why Propecia (a pill to block and lower DHT production in men ) is 70 percent effective and approved for use in men, but is not approved for effective hair loss doctors’ prevention in females, even at twice the normal dose; not to mention that it can cause birth defects in women who use it while pregnant during the first trimester of gestation in a male fetus.”
Propecia goes by the generic name of finasteride.
Of course, from a visible standpoint, female pattern baldness differs from male pattern baldness.
For some women, the first area to begin thinning is the part on the top middle or side of their head–wherever they prefer to wear a part.
Brushing the hair back so that it’s partless will mask this. However, this can then reveal — if not at that point, then eventually — thinning at the temples.
As time marches on, the pattern baldness in women takes on the form of diffuse hair loss, even though the part and temples may seem to show it most prominently.
In men, as we all know, make pattern baldness as it advances takes on that classic horseshoe pattern — after beginning with the proverbial shiny bald spot on the top back of the head.
Hair loss in women is often caused by mechanical means.
Avoiding mechanical insults to the hair root can go a tremendous way at preventing “balding.”
If you like ponytails, here are tips on how to prevent hair loss.

Dr. Dorin of True & Dorin provides creative hair loss solutions, including advanced hair transplant techniques and the latest in regrowth technology, to ensure that his clients achieve their desired results.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ShotPrime Studio

What It Means to Feel Your Pulse Everywhere

“Feeling of the pulse at different locations in the body can be completely normal,” says Chester M. Hedgepeth, III, MD, PhD, Executive Chief of Cardiology at Care New England.
“Importantly, all the arteries in the heart conduct the pulse wave started in the heart.
“Pulses can be felt in the large arteries of the neck (carotid artery) and leg (femoral artery).
“Normal pulses can also be felt in the wrist (radial artery), temple (temporal artery) and even the stomach with deep palpation (aorta).”
The aorta is the body’s largest blood vessel, originating from the heart and extending down the abdomen where it eventually branches off into the femoral arteries in the thigh that supply the legs with oxygenated blood.
“Patients frequently describe feeling their palpitations [pulse] in different parts of the body,” says Dr. Hedgepeth.
“PVCs are commonly associated with this sensation, as they cause a premature firing of the heart’s electrical system.
“Many patients feel a skipped and ‘heavy’ beat because the heart is ejecting significantly more blood volume.
“This ‘heavy’ beat can often be felt in the temple, head or neck.”
In summary, there is nothing to be alarmed about if you feel your pulse anywhere or “everywhere” on your body.
- There is no cause for concern.
- You can relax and breathe easy about this.
Think of your arteries as conduits, kind of like if you were to place your hand on a metal water pipe inside your bedroom wall and feel it vibrating, but the source of the vibrating is a water generator down the street.
 Dr. Hedgepeth also serves as a physician in the cardiovascular division and arrhythmia service at Brigham and Women’s Hospital, plus is an instructor of medicine at Harvard Medical School.
Dr. Hedgepeth also serves as a physician in the cardiovascular division and arrhythmia service at Brigham and Women’s Hospital, plus is an instructor of medicine at Harvard Medical School.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}