
Can a Skinny Ectomorph Be Strong?
There’s a reason why a skinny ectomorph may be able to lift an impressive amount of weight and seem quite strong. (more…)

Why Does Stress Cause Cold Hands?

Ever notice that in a warm room, your hands have suddenly gone cold?
You’re sitting there at the computer—doing some kind of work, rather than relaxing with an entertaining story—and you begin noticing, “Gee, my hands sure are cold.” (more…)

Can Sjogren’s Syndrome Cause ONLY a Cotton Dry Mouth?

If you’ve been suffering from a cotton dry mouth, could this possibly be Sjogren’s syndrome, even as your only symptom?
One of the hallmark symptoms of Sjogren’s syndrome is the very dry mouth.
This situation can have a number of causes, and one of the most notable, if not the absolute most notable, is that of the side effects of medications.
Hundreds of prescription drugs can cause the dry mouth. But what if you haven’t been on any medication?
What if you don’t have diabetes, which is another cause? AIDS and also Parkinson’s disease can be culprits.
But you’re healthy, right? So is it possible to have Sjogren’s syndrome with only that one symptom of dry mouth?
For this article I interviewed Ali D. Askari, MD, Professor of Medicine – Case Western Reserve University; Chief, Division of Rheumatology – University Hospitals Case Medical Center; Director, Rheumatology – University Hospitals Case Medical Center. Sjogren’s syndrome causes joint pain in many patients.
“Dry mouth and dry eyes are important components of Sjögren’s syndrome,” begins Dr. Askari, “and indicate the presence of inflammation in the salivary glands, and in a whole variety of other exocrine glands (these glands are the ones putting the secretions out into the body and not into the circulation).”
It’s possible for a cottony dry mouth to be the first sign of Sjogren’s syndrome, and the only symptom actually for many years before other symptoms (such as dry eyes, joint pain, a burning throat) begin to show.
But usually, the Sjogren’s dry mouth is also accompanied with eyes that are dry (which may include itchiness, burning or a gritty feeling). In 80 percent of patients, joint aches or pain present themselves.
Antibodies associated with Sjogren’s syndrome are present in 60-70 percent of the patients.
“In the absence of clinical manifestations and the absence of antibodies, one can proceed with doing a lip biopsy,” says Dr. Askari, “which is a small incision biopsy of the (inside of) lips, and that indicates the presence of inflammatory changes, that supports the diagnosis of Sjögren’s syndrome.”
The lips contain salivary glands, and when Sjogren’s syndrome reduces saliva production, dry mouth results.
“In the absence of all these findings,” says Dr. Askari, “one can presume the dryness of the mouth and eyes are due to causes other than Sjögren’s syndrome.”
And these include “iron overload in the body referred to as hemochromatosis, hyperlipidemia (excess fat in the blood stream), sarcoidosis (formation of inflammatory cellular clumps that can exist throughout the body), and other immunologic disease, which can lead to the inflammatory changes of salivary and lacrimal (tear duct) glands.”
When a person has only the dry mouth along with dry eyes, this is called sicca syndrome.
Dr. Askari says, “Occasionally dryness of the mouth and eyes precede other manifestations of Sjögren’s syndrome for years.
“This is especially important in the close relatives of those who have already been diagnosed with primary Sjögren’s syndrome based on criteria established for this diagnosis.”
For a diagnosis of Sjogren’s syndrome, the dry mouth (or the eyes) must be present for three months; there must be objective findings such as a chronic enlargement of salivary glands; and a lip biopsy must be positive for antibodies.
There are two other causes of cottony dry mouth, but they are not chronic: salivary gland infection, and salivary gland “stones,” which are mineral deposits that become large enough to block the salivary gland portals through which saliva is secreted.
The latter is fairly common and can present with just a dry cottony mouth, but may also present with difficulty in swallowing, opening the mouth, and pain in the mouth or face.
Sometimes, though, there are zero symptoms.
Update: As of April 2024, Sjogren’s syndrome is now known as Sjogren’s disease.

Dr. Askari’s special interests include diseases of the muscles, fibromyalgia, general rheumatology, lupus and Sjögren’s syndrome.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

10 Reasons the Weight Loss Has Stopped Despite Exercise & Diet

Some of the reasons you’ve stopped losing weight despite all that exercise and strict dieting will shock you.
#1. You haven’t been lifting weights.
This particularly applies to young females (afraid of bulking up) and people over 50 (thinking they’re too old or might get injured).

Shutterstock, Travelerpix
Muscle is the metabolic furnace of the body.
The more muscle you have, the faster resting metabolism will be, even during slumber. Lifting weights will dramatically jump-start metabolism.
#2. Focusing on long cardio sessions and doing only a little lifting.
Long, frequent sessions on cardio equipment, or that after-dinner “power walk” have limitations regarding fat loss.

Twenty minutes of high intensity interval training on a stationary bike three times a week will cause much more weight loss than will two hours of steady state walking seven days a week.
#3. Skipping breakfast
You might think you’re saving calories, but many times, the absence of a morning meal will cause greater hunger later on, causing you to eat more than you would have, had you eaten breakfast.
#4. Skipping meals or going long periods without any food.
For some, this may slow metabolism because the body learns to become efficient at storing fat.
For others, long periods of not eating result in fatigue, which then adversely impacts exercise.
#5. Not eating enough.
“You are not consuming enough calories,” says Amanda A. Kostro Miller, RD, LDN, whose specialties are nutrition counseling, weight loss and medical nutrition therapy.
“According to the Harvard School of Medicine, women should eat at least 1,200 calories per day.
“Men should eat at least 1,500 calories per day. Consuming less than these amounts may deter weight loss.”
#6. Poor sleeping habits.
They finally caught up with you and are interfering with your weight loss goals. Aim for 7-8 hours of quality sleep.
This maximizes release of human growth hormone during sleep.
Human growth hormone is a natural fat burner.
#7. Frequent napping.
A 20 minute snoozer is fine, but some people, despite sleeping 7-8 or even nine hours, will take a two hour nap most days.
This is complete inertia and completely unnecessary in an otherwise healthy adult who’s already getting sufficient sleep overnight.
#8. You don’t lift heavy enough weights.
Surprise! Those green dumbbells aren’t enough. And when you set the barbell down for your heaviest deadlift set’s last repetition…do you really feel like you can’t do more?

Shutterstock, Lisa F. Young
If you can do more than 12 repetitions, increase the resistance to keep your body in a shocked mode, rather than a maintenance state.
A shocked body burns more fuel (body fat) to adapt.
#9. Few compound exercises.
Clients who want to lose weight whose trainers have them doing things like standing on half balls and curling small dumbbells for 10 minutes are wasting their money.

Shutterstock, Reshetnikov_art
Compound exercises such as the deadlift (above) target multiple muscle groups simultaneously, forcing the body to dig deeper into fat reserves for energy and recovery fuel.
A top trainer knows that the cornerstone for weight loss includes the squat, deadlift, leg press, bench press, standing overhead press and pulling movements, all done with heavy resistance.
#10. Counting housework and yardwork as exercise.
This sabotaging approach leads to skipping structured workout sessions.
Bonus: MORE Reasons You’ve Hit a Weight Loss Plateau and Can’t Bust Past It
• “Your calorie goal is too high for your new weight,” says Kostro Miller.
“Now that you’ve lost weight, your body may actually need even less calories. Have your calorie needs reevaluated by a dietitian after weight loss.
• “You’re holding onto water weight,” continues Kostro Miller.
“People can hold onto water weight for a variety of reasons. For women, the time of the month can affect our water weight.
If you have certain health conditions that put you at risk for water retention, that can slow or stop weight loss.
If your diet is high in sodium, sodium can make you retain water.
• “Your weight loss diet is not sustainable. If you tried a fad diet and lost a lot of weight, don’t expect it to stay off.
Fad diets like the boiled egg diet, cottage cheese diet, etc., are designed to make you lose some weight initially, but then weight loss stops when you stop the fad diet.
Choose a sustainable weight loss plan that will help you in the long run.
• “Control your alcohol intake. Alcohol can throw off metabolism and can be a cause of weight fluctuations.”
Women should consume no more than four ounces of liquor/day, and for men, it’s eight ounces.
“Having several drinks in a night can make us temporarily retain water weight.”
Amanda Kostro Miller has worked with U.S. veterans, people with eating disorders and those with various acute and chronic diseases.
has worked with U.S. veterans, people with eating disorders and those with various acute and chronic diseases.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Depositphotos.com

Woman Over 35, Never Married? Why Nothing’s Wrong with You

Women over 35 who’ve never been married need to stop letting all the clowns out there make them feel that there’s something wrong with them.
(more…)

Weightlifting Gloves Pros and Cons for Weightlifting Routines

Weightlifting gloves are a common sight among fitness enthusiasts who do strength training and bodybuilding workouts. (more…)
Muscle Twitching Fear: Foot Drop Strength Test Guidelines
If twitching muscles have you panicking, here’s how to do foot drop strength tests.
If you’re terrified that the twitching muscles in your leg or foot might mean that you have ALS (and you would have gotten this idea after googling “twitching muscles,” no doubt), then invariably, you soon learned of a phenomenon called foot drop.
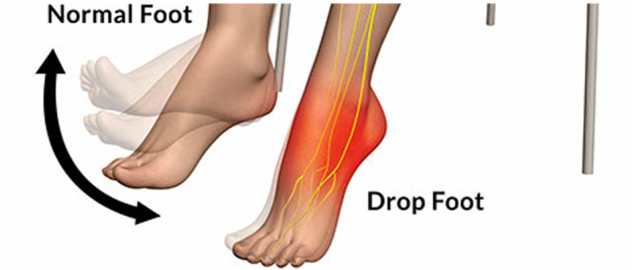
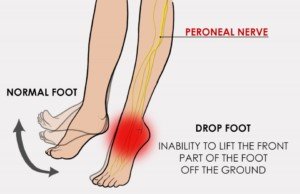
Foot drop itself is not a disease; it’s a symptom that can have many causes.
“Foot drop is typically neurological in nature,” says Dr. Bruce Pinker, DPM, who specializes in sports medicine and surgery of the foot and ankle.
In addition to a neurological cause, “It can be due to stroke (cerebral vascular accident – CVA), which may or may not resolve with physical therapy,” continues Dr. Pinker.
“Usually, in cases of foot drop, the forefoot drags on the floor — as the foot cannot clear the ground during the swing phase of gait.”
But how do you do strength tests for foot drop?
If you had this problem, for real, not just perceived, your gait would be altered to accommodate it.
Namely, you’d be having to lift your knee higher when walking.
Is that what you’ve been doing lately? If not, ask yourself why you’re convinced you have foot drop (other than googling “twitching muscles”).
Now let’s think of some everyday movements that foot drop would prevent you from doing.
Using the pedals of your car might come to mind. Think of how often, during just one 20-minute trip in your car, your foot must flex and extend to work the pedals.

Shutterstock/StepanPopov
There are muscles in the lower leg that move (flex and extend) the foot. If they are weak enough, the foot will drop.
If you have a disease causing enough foot drop to interfere with your walking, it will also interfere with using your car’s pedals.
What about actual strength tests?
The gas pedal usage is a test of flexion and extension with no resistance. But strength? Well, how about trotting up a flight of stairs?
That takes a lot more strength then using a gas or brake pedal.
Can you trot up a flight of stairs without stumbling or struggling?
If your ability to do this has not changed, then this should be reassuring.
Let’s take the foot drop strength test a bit further now. If you belong to a gym, load a calf raise machine with weights. Go up on your toes, then go down (extend, then flex).

Shutterstock/Denis Val
Though the calf raise equipment is designed to work the calves, the foot plays a key role in this because calf muscles move the feet!
For instance, your gastrocnemius and soleus muscles (major calf muscles) are responsible for plantarflexion (going up on the balls of your feet).
Your anterior tibialis muscle enables dorsiflexion (raising the foot/toes upward).
On the calf machine, these two joint actions are possible with weights. See what you can do.
Don’t try to break records; just do what you’ve either been doing, or if you’ve never used this machine, start with light weights.
After doing what you can (don’t overdo it, though; you don’t want sore calves), ask yourself how possible it is to have pathological foot drop if both feet can carry out the motion.
Another strength test is a hard sprint across a parking lot. To be able to do this you must have fully intact, fully functioning muscles and nerves.

Shutterstock/Franck Camhi
Do some jumping. Jump onto a boulder or bench. Leap across a puddle or up a few stairs.
Jump down from a few steps. Jump rope. Bunny hop. Do squat jumps. Kick a heavy bag.
“The activities you have mentioned would qualify as a self-test for whether or not one has foot drop,” says Dr. Pinker.
Unfair Strength Tests for Drop Foot
If you’re freaking out over twitching muscles and decide that a good strength test for drop foot would be to see how long you can balance on one leg, you will set yourself up for doom.
That’s because balancing on one leg, while in a state of fear, is not easy, even for a fit individual. Instead, just run down the street for your strength test.
Don’t try crazy things like seeing if you can hop up a flight of stairs on one leg.
Even a healthy fit person would find this very difficult. Don’t even try hopping across a room on the single leg.
These feats require a level of agility and strength that come from specific training.
The average person will struggle or may not even be able to do them.
And remember, exercise can cause some harmless muscle twitching.
 Dr. Pinker is with Progressive Foot Care, which provides state-of-the-art, full diagnostic testing and treatment of the foot. He’s a professional foot and ankle health and wellness speaker who delivers many original seminars annually such as “Keep On Running.”
Dr. Pinker is with Progressive Foot Care, which provides state-of-the-art, full diagnostic testing and treatment of the foot. He’s a professional foot and ankle health and wellness speaker who delivers many original seminars annually such as “Keep On Running.”
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

The Height Every Woman Wants

Most women would trade their height for another height, it seems.
The average American female is 5-4. There are a ton of women who stand 5-1 to 5-3. I think many wish they were taller. (more…)

Best Weight Loss & Confidence Exercises for the Morbidly Obese
There are plenty of exercises for morbidly obese people to do.
Nevertheless, a morbidly obese individual might be wondering what the best exercises are for his or her size. (more…)

Top 10 Muscle Twitching Reassurance Rules for ALS Fear
If twitching muscles are terrifying you about ALS, here’s all the reassurance you need from someone “eight years out” from benign fasciculations.
“Muscle twitching, also called fasciculations, are small, local muscle contractions that occur involuntarily,” says Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths and Tricks: A Physician’s Advice.” Dr. Tavel adds, “Deeper areas can be felt but are not visible.”
Rules for Twitching Muscle Reassurance
#1 Muscle Twitching Is Common
Dr. Tavel explains, “They occur in nearly all healthy men and women.
“In some cases, these fasciculations can be annoying but, if a neurological examination is negative, it’s best you disregard them.
“Fasciculations have a variety of causes, and most of these are benign, especially when the eyelids are affected.”
#2 Search Result Deception
If ALS sites appear at the top of the first page of search results for “Why do my muscles twitch?” this in NO way correlates to the odds that your twitching muscles are being caused by ALS.
Just because sites that mention ALS are in the top half of the first page of results, doesn’t mean this is what you should fixate on.
However, people tend to fixate on the first five results of a search.

Shutterstock/fizkes
What puts something on the first page of Google is the way the article is written plus other factors that Google’s web crawlers detect.
If it’s cleverly written, especially on an SEO-optimized site, it will be in the top three—and often in the No. 1 spot.
If I wrote an SEO-optimized article claiming that most muscle twitching is caused by drinking orange milkshakes, it just might end up on the first page of search results.
#3 Avoid ALS Sites
These will only get you more worked up, more panicky.
Many posters in ALS forums don’t even have ALS.
I also wonder how many thread responses you must read before you come upon one that was posted by an actual neurologist.
Be leery of forums. These are people just as panicky as you.
However, every so often, a thread is started by someone who got a very bad diagnosis—not necessarily ALS; could be MS or some other neurological malady.
Just stay off the ALS sites. These will only fuel your panic.
#4 Avoid Yahoo Answers
I swear, some of the answers are really nutty.
The fact that the avatars are cartoon faces all in the same pose doesn’t help with the credibility of the people “answering” the questions. Just skip it.
#5 Do Strength Tests
As a former personal trainer, group fitness instructor and always longtime fitness and strength enthusiast, I fully endorse strength tests for reassurance.

But you must do these within reason. Come on, if you’re not into lifting weights, don’t expect to hoist a 30 pound box of books onto a high shelf without difficulty (especially if you’re a woman who’s never weight trained).
Don’t try strength tests you’ve never done, either. For instance, if you’ve never before balanced for one minute on one leg while holding a bowling ball…don’t do this as a strength or coordination test.
Instead, keep tabs on tests of strength that your body is already used to, such as trotting up a flight of stairs, carrying out heavy garbage, and of course…gym workouts if you’ve already been doing them.
If your best bench press is five pounds less than it was last week, don’t panic.
If you normally bench 185 but next week can’t even do a single pushup, then yes, something is going on — but still, don’t jump to conclusions; it could be an injured rotator cuff.
Being able to lift more weights than previously, of course, is major reassurance. For reassurance, keep tabs on your gym progress.
#6 Avoid Mirrors Other than for Normal Use
Stop checking your tongue!
Stop checking the symmetry of your legs!
Stop analyzing your dents!
#7 Love Your Dents!
Did you know that people trying to lose weight just LOVE to see dents? So do people training for a physique or bodybuilding competition.
Dents almost always mean three things going on:
1) Low body fat in that area; new ALS awareness draws your attention to it
2) Recent fat loss which increases “definition,” and
3) The body’s natural asymmetry if the dent is visible or more prominent on one side.

Shutterstock/Chad Zuber
When I was a personal trainer, my clients loved showing me their newly discovered dents. Except they didn’t call them dents. They called them “definition.”
Dents in extreme form are called “cuts” by physique and bodybuilding athletes. A person with the so-called buff body has tons of dents, and if you look closely enough, they are NOT symmetrical.
For example, the “dent” (technically known as “separation”) in the quadriceps muscle group is often a bit more pronounced in one leg than the other.
#8 Time Passage
Though anyone who’s frightened by twitching muscles doesn’t have the patience to wait things out, it’s so very true that time passage without progression of symptoms is a powerful reassurance tool.
Mark a red “X” on a hardcopy calendar to indicate each day that there’s no progression, such as true muscle weakness (e.g., you can’t hold up your hairbrush, can’t blow dry your hair, can’t hang up clothes, can’t lift up the cat, can’t carry groceries, etc.)
Not being able to carry a 30 pound box of books up from the basement without fatigue doesn’t count—unless you’re a bodybuilder—and even then, bodybuilders aren’t immune to fatigue.
#9 Sliver Thin Odds of ALS
You’re more likely to get killed in a car accident than develop ALS.
Do you not realize how rare ALS actually is?
Sure, it gets a lot of publicity, especially with the ice bucket challenges, but this is a very rare disease. Yet how many people have you personally known who died from cancer?
#10 Get an EMG
If push comes to shove with your anxiety, get it over with: an EMG. Normal results go a long way in reassuring you.

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}