
10 Signs of a GOOD Nursing Home: Have Peace of Mind

Here are 10 signs that a particular nursing home would be a great place for your elderly loved-ones to live at – signs that you can feel good about and reassured they’re getting top-notch care. (more…)

Bladder Pressure: Causes (Including Cancers) and Solutions

The feeling of bladder pressure, even though you don’t have to “go,” has many potential causes including three kinds of cancer.
Causes of Bladder Pressure Excluding Cancer
Urinary tract infection. “Urinary tract infections are common and can be quite painful,” says Walter Gaman, MD, FABFM, board certified in family medicine and the author of several award-winning books including “Age to Perfection: How to Thrive to 100, Happy, Healthy, and Wise.”
“The first sign of a UTI is often cloudy urine followed by painful urination. Urinary tract infections are more common in women than in men,” says Dr. Gaman.
Cystitis. The bacteria that cause a UTI can also inflame the bladder. The feeling of pressure on the bladder is caused by muscle spasms, not urine buildup.
Prostatitis. “The prostate is a gland the size of a walnut,” says Dr. Gaman. “It sits just below the bladder. The function of the prostate is to produce semen. When the prostate becomes enlarged, it’s called prostatitis.
“Although the cause of prostatitis isn’t always known, a common cause is bacterial infection that is relieved with antibiotics.
“Because of the location of the prostate, inflammation can put pressure on the bladder. That pressure can cause nighttime urination, painful urination, a feeling of fullness or pressure on the bladder, and even cloudy urine.
“Men often notice that their urine stream is weak, a tell-tale sign that they have prostatitis. This happens because the enlarged prostate is interfering with the bladder and urinary tract.”
Uterine fibroids. These benign masses can exert pressure that affects the bladder.
Endometriosis. Uterine tissue grows behind the uterus or endometrium, affecting the bladder.
Medical conditions not directly related to the urinary tract. These include a spinal cord injury or other neurological disorder that gives way to an overactive bladder. This is caused by impaired neuromuscular function.
Obstruction. A kidney stone or benign mass can cause an obstruction in the urethra, impeding the flow of urine.
Cancers that Can Cause Bladder Pressure
Obstruction. An obstruction in the ureter can also be a malignant mass.
Bladder cancer. You’ll feel you need to relieve yourself even though there is no urine to void. The tumor is pressing on the bladder. Other symptoms may be blood in the urine.
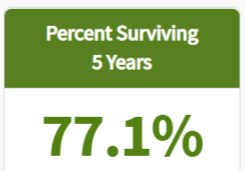
Survival rate for bladder cancer.
Ovarian Cancer. The growing cancerous mass can cause the ovaries and the uterus to put pressure on the bladder, creating the illusion that urine needs to be voided.
Bladder Pressure Remedies and Solutions
Preventing a urinary tract infection is the first line of prevention of bladder pressure.
“Prevention of urinary tract infections stems from the protection of the urethra from bacteria,” says Dr. Gaman. “If you are prone to UTIs, there are several things you can do to help prevent them.”
First, avoid wearing tight underwear; this can trap bacteria.
When you feel you must “go,” then do so. Holding it in can help proliferate bacteria.
“Always urinate and wash up before and after sex,” says Dr. Gaman. “This helps clear anything out of the urethra that may have been backwashed during intercourse.
“Limit the amount of sex you’re having to no more than four times a week. ‘Honeymoon bladder’ is a common term used by medical professionals to describe the common UTIs that occur in newlyweds who have frequent sex.
“Skip the bath and opt for showers instead. This is especially true if you add bath bubbles or body wash to your bath. If you do take a bath, be sure to urinate immediately after.
“Drink plenty of water. Dilute urine is better for a sensitive bladder and urinary tract than concentrated urine. Limit the amount of tea and coffee.
“Avoid spermicidal jelly and other lubricants that can cause irritation.
“Always wipe front to back. A common cause of UTIs is E.coli bacteria. E.coli is common in stool, but can cause serious infections if it reaches the vaginal area and travels to the bladder.”

Dr. Gaman is with Executive Medicine of Texas and is with the Staying Young Radio Show 2.0 podcast.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasha2109
Senior Orphans–Lonely Elderly: Causes and Solutions

It’s a fast growing problem: elderly people “orphaned” by their families and the health care system, at high risk for abuse, depression and illness.
The word “orphan” usually conjures images of helpless children with no one to care for them, but that same term can apply to seniors as well.
It is becoming a growing problem with these seniors who fall through the cracks of the healthcare system.
Senior orphans are people over age 65 who have no family, are isolated from family either because of dysfunctional relationships or geographic distances, or who have family members who take advantage of them financially.
With more single adults and fewer women having children to potentially care for them, the plight of senior orphans is potentially a huge one.
Nearly 25 percent of Americans over age 65 are at risk of becoming senior orphans, according to a study from researchers at the North Shore-Long Island Jewish Health System and the Hofstra North Shore-LIJ School of Medicine.
An example is an elderly patient who lived with his sister. Both had made quite a bit of money in their careers, but once in their eighties, both developed dementia and mental illness.
They had years of magazines and unopened mail stacked in their home, and had meals delivered so they could survive.
A neighbor befriended them and had them sign over power of attorney documents so he could “help them” pay bills.
In doing so, that neighbor also helped himself to money from their accounts.
Their patient advocate intervened by calling Catholic Charities, which in turn contacted the state guardianship office.
The couple was moved to an assisted living home, where they did quite well with adequate support and treatment for their multiple medical problems.
This story had a happy ending. Unfortunately, not all do. But there are steps people can take to prevent themselves from falling prey to a “helpful” neighbor or family member.
Solutions to Ending up a Forgotten Elderly Person
Start planning early. People should start putting a care plan in place in their fifties or early sixties.
The earlier the better, since the plans are cheaper when you’re younger. There are many different models of long term care (LTC) insurance.
Some, for example, are whole life plans that convert to LTC, and if the policy owner dies first, the benefit still gets paid to the family.
Consider consulting an estate planning attorney. Many people benefit from asset allocation trusts developed with monies already available; this is particularly important when chances are that the senior will eventually run out of money and have to rely on Medicaid.
An attorney can help clients prepare for Medicaid in ways that ease the transition. Trying to plan without expert help can be a bad idea.
Understand the costs. One of the biggest mistakes people make is giving away money to family members without understanding how much they may need that money for their own care down the road.
Nursing home costs are expensive—typically from $6,000 to $10,000 per month. People often run out of money quickly once they enter skilled nursing care homes.
Medicare usually covers only 100 days of rehab yearly but may ask you to leave a facility after three weeks if progress is not being made. After that, the patient is responsible for all of the costs.
Know that the best care comes at a price. The higher-quality nursing homes rarely admit people when their resources are almost depleted and they are in the process of applying for Medicaid.
The reality is that the more money one has, the more choices there are.
Recognize that family members don’t always have your best interests at heart.
There is, unfortunately, a big problem with elder financial abuse in this country.
Healthcare professionals regularly encounter sons and daughters who are reticent to approve needed expenses for long-term care of their parents because they are experiencing financial stresses themselves.
They are afraid that there will be no inheritance left for them if Mom or Dad gets transferred to an assisted living or quality skilled nursing facility.
Seniors do have legal protection if people try to take advantage of them financially. Elder financial abuse is a felony.
When abuse is reported, bank accounts can be frozen, a guardian appointed and perpetrators sent to jail. “But why get to that point?”
With a plan in place, seniors can make sure their needs are well taken care—even if they reach a time when they can no longer take care of themselves.
 Teri Dreher, RN, CCM, is the founder of NShore Patient Advocates. A critical care nurse for 35+ years, she’s also the author of “How to Advocate for Yourself & Your Loved Ones,” available on Amazon.
Teri Dreher, RN, CCM, is the founder of NShore Patient Advocates. A critical care nurse for 35+ years, she’s also the author of “How to Advocate for Yourself & Your Loved Ones,” available on Amazon.
.
Top image: Shutterstock/wavebreakmedia
Red Urine Isn’t Always Blood, But You’d Better Be Sure

Seeing red in your urine can mean you have cancer, and the cancer can involve one of three possible structures.
The bladder is the most likely source of cancer-caused blood in the urine.
What can red urine mean?
“Red urine is not always blood, but you better be sure,” says Michael D. Lutz, MD, board certified urologist with Corewell Health/Beaumont Hospital; President, MIU Men’s Health Foundation.
“Visible blood in the urine can have multiple potential causes including infections, stones of the urinary tract, coagulation disorders or cancers of the urinary tract,” continues Dr. Lutz.
An infection in this case may be of the urinary tract. A coagulation disorder is one in which blood has difficulty clotting and thus can cause internal bleeding.
Dr. Lutz explains, “Only a detailed urological evaluation and appropriate studies can determine the significance or the underlying cause.
“Approximately 13 percent of the population will have microscopic or visible blood in their urine, and one-third will have a urological cause.”
Blood in the urine can also be caused by excessive running or marching. But if you notice a correlation between prolonged running, hiking, etc., with red in your urine, by all means still get yourself checked out.
“Cancers lining the urinary bladder, kidneys or the ureter, occur in a ratio of 50:3:1,” says Dr. Lutz.
“Therefore, the most common malignancy in the urinary tract which causes bleeding is typically bladder cancer.
“The majority of bladder cancers are confined to the lining of the bladder and can usually be treated locally with the occasional additional usage of localized chemotherapy placed into the bladder to help cure the disease and reduce the risk of recurrence. Continued surveillance is the key to a successful course and outcome.
Urine can take on a reddish or pink tinge after you’ve consumed beets. This has nothing to do with blood and is a harmless situation.
 Dr. Lutz is experienced in all areas of adult urology and has special interests in urological cancer, male fertility and urologic stone disease. Men’s Health Foundation
Dr. Lutz is experienced in all areas of adult urology and has special interests in urological cancer, male fertility and urologic stone disease. Men’s Health Foundation
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Eag1eEyes

How Does a Dermatologist Check for Melanoma?
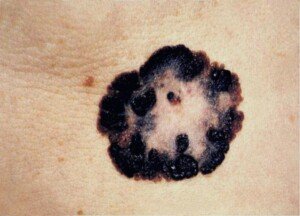
Here’s how to make sure a dermatologist is doing everything possible to check your skin and moles for signs of melanoma. (more…)

Causes of Trapezius Pain Can Include Cancer

When it comes to trapezius pain, few people actually consider cancer and automatically assume it’s just a strained muscle from working too hard or a sore muscle from a gym routine.
But cancer can actually lead to pain in the trapezius muscle.
And it isn’t just one type of cancer that can do this.
Soft-Cell Sarcoma
A soft-cell sarcoma type of cancer can cause pain in the trapezius.
Most of these malignant masses develop in the upper body and can affect the shoulder area.
The definition of a soft-cell or soft-tissue sarcoma is a cancer that develops in connective or soft tissue.
These rare tumors involve less than one percent of all new cancer diagnoses every year in the U.S. Most patients are over 50.
Along with pain in the trapezius muscle, the cancerous mass may also be felt as a lump or area of swelling, and can cause mobility problems.
Putting the Rarity of Soft-Cell Sarcoma in Perspective
“I don’t ever recall seeing a soft-cell sarcoma affecting the shoulder area,” says Dr. David Beatty, MD, a retired general practitioner with 30+ years of experience and an instructor of general medicine for 20+ years.
“I used to audit our practice mortality figures between about 1990 and 2010.
“The practice had 16,000 patients and six to eight doctors.
“Each year about 160-200 people lost their lives. We lost someone with soft-cell sarcoma roughly every other year.
“Given that some sarcoma patients would have survived, I would estimate that the incidence was approximately one person per year for our practice.
“I would only have managed about one in seven of these patients, so I personally would have seen a new case about every seven years.”
Bone Cancer Spread
Osteosarcoma (bone cancer) can metastasize to the trapezius muscle and cause pain.
A report in World Journal of Surgical Oncology tells of a 51-year-old who was diagnosed with bone cancer in the leg.
He underwent chemotherapy and then developed pulmonary metastasis.
A year later a lump was found in his shoulder – the trapezius muscle. The report calls this incident “extremely rare.”
What Trapezius Muscle Pain Is Most Likely to Be
Pain, discomfort or soreness in the traps by far is most likely to be of musculoskeletal origin – caused by some kind of positional or loading strain.
• Hunched over a desk for prolonged periods
• Odd body positioning (e.g., cradling phone between ear and shoulder)
• Non-ergonomic settings such as a keyboard that’s too high or a chair with short armrests
• Sleep position
• Sport or weightlifting
• Repetitive stress injury from work
• Purse or sack slung over one shoulder
• Bra straps
Additional Causes of Trap Pain
• Whiplash
• Uneven leg length
• Tensing up the shoulders
• Heavy coat
“Distorted forward head position with a loss of the normal cervical curve can result in the over-firing of the upper traps, as well as other muscles,” says Dr. Tom Carpenter, corrective exercise specialist, certified personal trainer and chiropractor, inventor of Stand Corrected™, a portable harness-like stretching tool that helps alleviate back, neck and shoulder pain.
Dr. Carpenter further explains, “Poor breathing techniques while exercising can cause these muscles, which are considered accessory muscles for breathing, to be overworked to the point of strain and spasm.
“Also, many people seem to hold their tension from stress in this area.
“Correction of vertebral spinal alignment, myofascial release techniques, trapezius stretching and strengthening, and attention to posture correction can all help to relieve this discomfort in many cases.”

Stand Corrected™
Though the answer is “Yes” to “Can cancer cause pain in the trapezius muscle,” it is extremely unlikely that this is the cause of your pain.
Nevertheless, if you’re worried or the discomfort doesn’t resolve (and especially if it’s accompanied by mobility problems), do not hesitate to see a doctor.
 Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.

Photo credit: Aleesia Forni
Based upon 30+ years of experience, Dr. Carpenter’s practice approach reflects his belief that restoring optimum health and function will enable his patients to enjoy a much greater amount of vitality and wellness. Chiropractic care is true health care, not sick care!
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/BLACKDAY
Sources:
triggerpointrelief.com/cdrom/trapezius.html
knowcancer.com/oncology/connective-tissue/
ncbi.nlm.nih.gov/pmc/articles/PMC4050446/
sarcomaalliance.org/what-you-need-to-know/how-rare-is-sarcoma-really/ cancer
Can You Be Too Weak for a Normal Strength Training Program?
There is no such thing as being too weak for a normal strength training program.
Can you pick up a broom? Then you can deadlift.
If you’re lying down, can you push the broom up with your hands? Then you can bench press.
Have you ever squatted to pick something up? Then you can do squats.
Do you have to do pushups or pull-ups for a good solid strength training program? No.
There are untrained individuals who believe they are too weak to work out with weights.
Have you ever stocked your cupboard and removed from it soup cans?
Then you can strength train.
If you feel too weak to lift weights and are brand new to the world of strength training, tell yourself that this new endeavor, at the beginning, will be more about assuming CORRECT FORM rather than lifting heavy weights.

Freepik.com
Most gyms have five-pound bars. You can begin with this tool and work on your deadlift and squat forms.
And along the way, you’ll get a little stronger, because you’re working with five pounds of added resistance that your body is not used to.
You can lie on a bench and press this bar above you for the bench press, acclimating your body to this movement.
You can do exercises with two and a half pound dumbbells or tiny weight plates.
There is no such thing as being too weak for a strength training program.
For seated rows you can insert the pin at the very top of the weight stack and perform this exercise at the lightest resistance. You can apply this approach to other machines.
There are very frail, elderly people who do strength training. However, those who believe they’re too weak to lift weights are often much younger.
Ask Yourself…
• Do I pick up babies and toddlers?
• Do I carry out garbage?
• Do I carry groceries?
• Do I carry a dog?
• Do I carry a vacuum cleaner?
• Do I ever carry a can of paint, a tool box or move a big potted plant?
All of the above, technically, falls under the category of lifting weights.
Stop making excuses. You do not need to be strong to begin a weightlifting program. Every time you stand up from a chair, you lift weight.
You will not build fitness, health and strength by avoiding training with weights.
There is a lot to learn, however, but as the saying goes, “How do you eat an elephant? ONE BITE AT A TIME.”
Recommended Exercises for Novice Weight Training
• Squat (barbell, kettlebell, dumbbell, medicine ball, even body weight)
• Deadlift (barbell)
• Leg press
• Leg extension and curl
• Bench press or inclined press
• Overhead press (barbell or dumbbell)
• Seated cable row
• Lat pull-down
• Kettlebell swing
Dumbbells and kettlebells start at around two pounds. Though not all gyms have five pound bars, see if yours does, or perhaps yours has weighted bars of 10 or 15 pounds only.
Try those. If they’re too light, your gym probably has pre-fixed weight barbells as light as 20 pounds.
An unloaded Olympic bar is 45 pounds.
If you want to use weight stack machines, use ones for the chest press, overhead press and pulling motions (e.g., pulling down from above).
Tension Bands
Tension bands and tubing are another option for strength training.
Operators of gyms want to make money. From a business standpoint, it would make zero sense for the operator to design a gym that only strong or fit people can use.
Nearly ALL people are able to work out at a gym – this is the best way for the gym owner to make a profit!
So if you think you’re too weak to lift weights at a gym, you could not be more mistaken.
![]()
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Can Cancer Cause One Eye to Keep Tearing?

Yes, cancer can actually cause one eye to begin tearing, a condition called unilateral (one-sided) epiphora.
There are far more common causes of this situation – but tumors are not excluded from possible causes of one eye mysteriously getting very watery.
“The lacrimal glands are the glands that produce tears to lubricate your eyes,” begins Gene Liu, MD, MMM, and Chief, Division of Otolaryngology, Cedars-Sinai Medical Group.
“As you blink, the tears are spread across the eyeball itself and then drain through small pipes called the nasolacrimal ducts, or tear ducts, into the nose,” explains Dr. Liu.
“Epiphora is the medical term for a watery eye and can happen with irritation of the eye, a problem with eyelid position or tone, or something that is causing an issue along the drainage pathway.”
An obstruction in the drainage pathway, caused by a cancerous or benign tumor, will result in a buildup of tears.

The eye will then water up, sometimes to the extent that full tears are dripping down one’s face.
The unilateral epiphora can be caused by a benign lacrimal sac tumor or a malignant mass.
Lacrimal Gland Tumors
• 72 percent are cancer and 28 percent are benign, according to reviewofoptometry.com, but only 50 percent are cancer, according to reference.medscape.com.
• Cancer must be ruled out when a patient presents with one eye that keeps tearing– especially if there are other symptoms.
• “The likelihood that epiphora is caused by a cancer of any part of the nasolacrimal system or sinuses is extremely low,” says Dr. Liu.
“These types of problems are not only very rare, but usually also would cause a lot of other symptoms.”
How rare are these malignant masses?
A report in Smith and Nesi’s Ophthalmic and Plastic Reconstructive Surgery (2012) says, “Approximately 750 cases [of malignant AND benign lacrimal sac tumors] have been reported in the literature over the last century, of which 50 to 100 percent were malignant.”
A report in a 2013 Ophthalmic Plastic Reconstructive Surgery (a different journal than above) states, “Lacrimal sac tumors are rare with approximately 300 cases described in the literature.”
A report in the online journal Cancer (2011) states, “Forty-six patients with malignant epithelial neoplasms of the lacrimal apparatus were treated at a single institution from 1945 through 2008.”
And finally: “Whereas there are a myriad of small case series and reports, fewer than 250 cases have been reported in the international literature and population data are scarce.” (JAMA Otolaryngology – Head & Neck Surgery, 2014)
So based on the above excerpts, you should be very reassured that the odds that your unilateral epiphora being caused by cancer are exceptionally unlikely.
Furthermore, the most common age for diagnosis is in the 30s, and the second most common age is in the teens.
If you’re in your 30s, don’t panic. Reread the above data to absorb just how incredibly rare this cancer is.
Symptoms of Lacrimal Gland Tumor Other than Epiphora
• Double or blurry vision
• Pain in or near eye
• Eyelid fullness or lump in eyelid
• Swelling around the eye
To be fair, a brief coverage of another type of cancer that can cause one eye to tear needs to be made.
A tumor can form in the naso-pharyngeal cavity. These are called paranasal or sinus tumors.
According to hopkinsmedicine.org, some possible causes are:
• Exposure to industrial chemicals
• HPV infection
• Exposure to leather, wood, nickel, textile, chromium or flour dust
• Cigarette smoking
• Not all paranasal tumors have known causes.
Cancer.org says that about 2,000 U.S. people a year are diagnosed with a paranasal tumor. Eighty percent of patients are at least 55 and most are men.
Symptoms of a Paranasal Tumor Other than Epiphora
• Bulging eye
• Vision problems
• Persistent sinus congestion
• Nasal drip
• Frequent nosebleeds
• Change in voice
• Reduced sense of smell
• Headache
• Facial numbness
• Loose teeth
• Trouble opening mouth
Benign Causes of One Eye Tearing
“A gradual onset of epiphora with no other symptoms or findings is almost always due to narrowing or scarring of the nasolacrimal duct,” says Dr. Liu.
“This can happen with the development of casts or stones [hardened debris inside the drainage system], from inflammation of the nose and sinuses [infection], from trauma, as a result of inflammatory disease such as sarcoidosis, and many other obscure medical reasons.”
– Canalicular obstruction (caused by debris from lids, lashes, makeup, conjunctivitis, age related constriction). The canaliculum is part of the drainage system.
– Canaliculitis (inflammation of canaliculum)
– Cysts
– Dacryocystitis (lacrimal sac infection)
– Dacryocystocele (lacrimal sac enlargement due to congenital problem)
– Facial (blackhead extractions on the nose)
– Lacrimal diverticulum (herniation)
– Laceration (tiny cut)
A condition called recurrent corneal erosion can also cause only one eye to water up too much.
Corneal irritation (from past trauma such as walking into a protruding tree branch or a fingernail contacting the cornea) triggers hyperlacrimation. This condition can develop months or years after the trauma.
Parting Thoughts
• If one eye gradually or suddenly begins tearing (unilateral epiphora), chances are extremely unlikely that the cause is cancer.
• Don’t panic. See if it runs its course and tapers off after a week or so.
• Be on the ball for other new-onset symptoms that seem associated.
 Dr. Liu’s clinical areas of focus cover a broad range including surgery of the head and neck, sinuses and thyroid, and disorders of the ears, salivary glands and vocal cords.
Dr. Liu’s clinical areas of focus cover a broad range including surgery of the head and neck, sinuses and thyroid, and disorders of the ears, salivary glands and vocal cords.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
Sources:
reviewofoptometry.com/ce/disorders-of-the-nasolacrimal-system
reference.medscape.com/article/1210619-overview
reference.medscape.com/article/1210619-overview#a6
link.springer.com/chapter/10.1007%2F978-1-4614-0971-7_40#page-1
ncbi.nlm.nih.gov/pmc/articles/PMC4081470/
onlinelibrary.wiley.com/doi/10.1002/cncr.25813/pdf
jamanetwork.com/journals/jamaotolaryngology/fullarticle/1935579
cancer.org/cancer/nasal-cavity-and-paranasal-sinus-cancer/about/key-statistics.html
hopkinsmedicine.org/healthlibrary/conditions/adult/nervous_system_disorders/paranasal_sinus_tumors_134,87/

How Dangerous Is Feeling a Pulse in Your Stomach?

If you can feel a pulse in your stomach, this can mean a life-threatening condition involving a major blood vessel that runs down your abdomen or a cancerous tumor. (more…)
You Know It’s Time to Start Strength Training When …
Have you been toying around with the idea of starting a strength training regimen but keep putting it off, waiting for the “perfect” time?
Well, there really isn’t a perfect time to begin training with weights, but you certainly know you’re READY to start lifting weights for fitness when certain things are happening with you — whether you’re a woman or a man.
It’s Time to Start Strength Training When …
• Every time you look in the mirror at your arms, you grimace or shake your head.
• You have a habit of grabbing the flappy part of your upper arm and staring at it in disdain.
• You sometimes find yourself deliberately making your “bat wings” jiggle by patting them with your fingers.
• You do the same thing with your inner thighs.
• Every time you see a woman with a super toned body, you think, “Why can’t I look like that?”

This is not a body of malnourishment. It’s a body of strength training and food portion control. Those are strong arms, not weak arms! Shutterstock/Jacob Lund
• You’re sick and tired of asking men – and even women – to carry heavy things for you — definitely a clue it’s time to start hitting the weights!
• You can’t pick up your 125 pound wife or girlfriend.
• You dread carrying your preschooler or toddler around, especially when it’s time to set them in the car seat.
• You let garbage pile up for someone stronger to take out.
• You avoid doing tasks that involve lifting something weighty like removing a box of books from a high shelf.
• Your jeans no longer fit but you haven’t gained weight on the scale.
• You’ve heard at least one person call you “skinny fat” — a clear indication it’s time to start strength training.
• You’ve gained fat despite not increasing your caloric intake.
• Your back is beginning to ache for no apparent reason.
• Your back and/or body aches after doing housework, yard work or participating in an unexpected play session with the kids.
• You dread helping a friend move despite the free pizza and beer – not because you’d rather be relaxing on your deck on a Saturday afternoon reading a book but because you know that the physical work will drain you for the next three days.
• You make your seven-year-old shovel the snow in the name of contributing to the household when you know the real reason is that it would kill your back.
• You stomach is mysteriously increasing in size even though you’ve cut back on the beer and donuts.
• Your young child lovingly says you’re “squishy.”
• You pay markedly close attention to the TV whenever a commercial comes on for a health club.
• When you find nicknames like “Beanpole,” “Skones,” “Teddy Bear” and “Chubs” no longer endearing.
• When friends suggest you enter a Mr. Puniverse contest and you know you’d win.
Oh, and one more: When people keep telling you “Eat a cheeseburger!” or “Eat a salad!”
If you’ve answered “Yes” to even one of these bullet points, you know it’s time to begin strength training!
Though there’s never a perfect time to begin lifting weights, there is always a right time to start a weightlifting program for a fitter, healthier body composition, stronger joints, a boosted immune and cardiovascular system, better balance and better brain function.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}