

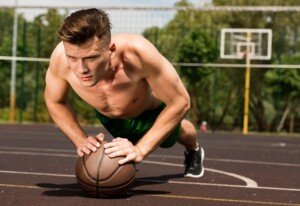
Thigh Muscle Twitching: Don’t Worry, or Panic?

Does your thigh muscle twitch like thump thump thump!?
Whether your thigh muscle twitching is continuous, periodic, just a flutter or a real thumper, perhaps you’re freaking out that you might have ALS, since ALS sites list muscle twitching as a symptom of this disease.
So there you are with that twitching thigh muscle, wondering if you’ll be dead in two years.
There are perhaps thousands of people sitting in that boat right with you, worried sick over their twitching thigh muscles, wondering if they’ll be alive two years from now.
If you have a twitching thigh muscle, whether the twitch occurs many times per minute, or a few times per hour, every day or occasionally throughout each month, the chances of this being ALS are next to nothing — if not absolutely nothing …
… as long as you are walking fine; getting out of chairs fine; and are not stumbling or dragging a leg.
“Muscles may randomly twitch for many reasons,” points out Carolyn Dean, MD, ND. She is a medical advisory board member of the Nutritional Magnesium Association at nutritionalmagnesium.org.
“They can twitch due to anxiety or stress, a sleepless night, too much coffee or after exercise.”

Freepik.com
In ALS, you may have read that the twitching comes after muscle weakness, but online information is not definitive on this.
However, the muscle weakness of ALS isn’t something that you’d have to wonder if you actually had it.
In other words, struggling to get one’s legs up a flight of stairs certainly means something is very wrong.
ALS weakness is obvious without having to perform strength or balance tests like seeing how long you can stand on one leg, especially if it’s affecting a thigh muscle.
I recall watching the Jerry Lewis Telethon several years ago, and a victim of ALS was describing the onset of his earliest symptom.
He said it was muscle weakness, and it was literally overnight.
The man said he went out to jog and couldn’t do it. Now THAT’S pronounced muscle weakness.
This should alleviate your fears that any very subtle weakness in your thigh (or rather, what you perceive to be subtle weakness) is the beginning of ALS.
That is… it’s far more likely to mean something else.
When I was a personal trainer, I had clients all the time who had “weakness” in their thighs, which was corrected with exercise.

Shutterstock/IvanRiver
Another thing to consider:
- ALS weakness does not come and go.
- It does not switch on and off.
“Weakness from ALS is generally progressive, says Mitzi J. Williams, MD, clinical neurologist with Morehouse School of Medicine, an MS specialist and clinical advisor for the Multiple Sclerosis Foundation.
Dr. Williams explains, “There could potentially be mild fluctuations, but there should not be dramatic fluctuations in symptoms for prolonged periods of time.”
Ask yourself if your “weakness” comes and goes in more than a mild sense, especially if joint pain from overuse seems to be the trigger of the weakness.
And when the weakness is not there, don’t be surprised if during those times your mind is on something else! It’s there only when you’re obsessing about it!
Another cause of thigh muscle twitching is anxiety over unrelated matters.
Anxiety causes all sorts of physical symptoms, of which muscle twitching is one.
Furthermore, worrying about the twitching can make it persist or rapidly “spread” to other parts of the body.
A motor neuron disease does not spread body-wide in only minutes.
“Sometimes magnesium deficiency can lead to muscle twitching, so replacement of magnesium or other electrolytes can help alleviate the symptoms,” says Dr. Williams.
Lack of water intake can also fire up thigh muscle twitching.
Next time your thigh muscle is twitching, move it and see what happens.
If you are seated, move the leg back and forth. The twitching will probably stop.
Should you find yourself performing strength tests like seeing if you can lift out of a chair with one leg, be assured that this is inherently difficult to do, and your other leg will have just as much trouble.
If you had ALS, you’d have difficulty performing everyday routine movements, rather than just a gut feeling or sensation of weakness.
Twitching in your thigh muscle is generally caused by exercise, and the twitching can have a delay of one to two days from the onset of the exercise.
Here is what Kevin Plancher, MD, says about exercise and twitching.

Dr. Williams is author of “MS Made Simple: The Essential Guide to Understanding Your Multiple Sclerosis Diagnosis,” available on Amazon. She is a member of the American Academy of Neurology.

Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/crazystocker
Source: alsa.org/about-als/symptoms.html?referrer=https://www.google.com/

Triceps & Other Muscle Twitching, ALS Fear

Muscle twitching is a terrifying topic for many people because when they do some Googling, they think, “Twitching muscles is a symptom of a killer disease.”
Muscle twitching is very common, affecting millions of people, but ALS, the disease in which muscle twitching is a symptom according to medical sites, is extremely rare.
Nevertheless, a person with twitching muscles may become vulnerable to a terrifying hypochondria in which they think they have fatal ALS whenever a muscle twitches. But muscle twitching is a fact of life.
“While muscle twitching can be a concerning and disturbing symptom,” says Dr. Daniel Kantor, “many people have it simply as ‘one of those things.’”
Daniel Kantor, MD, is President Emeritus, Florida Society of Neurology, and director, Neurology Residency Program, Florida Atlantic University.
“It is nothing to worry about,” he continues. “Of course, you always want to clarify this with your primary care doctor or neurologist to exclude other, more serious, causes.”
As I type this, my triceps muscle is twitching away. I pulled my sleeve up and watched. Boing, boing, boing, like there was a beating heart below my triceps muscle.
But am I scared I might have ALS? No. It’s no coincidence that two days ago, I put my triceps muscles through a punishing weightlifting routine.
Two days out from grueling weight workouts often result in strange things, like muscle twitching.
If your muscles are twitching, ask yourself if one or two days ago, you worked that muscle pretty good.
Shutterstock/LightField Studios
The fact that you can see the twitching is NO cause for concern. Of COURSE you can see the muscle twitchin’ away; why wouldn’t you be able to see it?
Muscle Twitching Can Be a Good Thing
You can train your mind to accept it, and then perceive it as cool — as in: It feels neat when muscles twitch, especially fatigued muscles that are drained from exercise.
My right hamstring is strained, and when it twitches, boy does it feel good !
The twitching is like a little massage machine inside the hamstring, soothing it.
What makes muscles twitch?
“Muscles may randomly twitch for many reasons,” says Carolyn Dean, MD, ND, and medical advisory board member of the Nutritional Magnesium Association at nutritionalmagnesium.org.
She adds, “They can twitch due to anxiety or stress, a sleepless night, too much coffee or after exercise.”
Muscles will twitch even more if your anxiety is related to ALS. People who suffer from this hypochondria will typically report that one day, a twitching muscle was becoming annoying.
So they googled muscle twitching and several ALS links came up. The link descriptions clear-out say muscle twitching is a symptom.
The person panics and suspects they have ALS. They then visit the ALS site and read that muscle twitching is one of three chief ALS symptoms. The fear intensifies.
Convinced they might have ALS, the person becomes overwhelmed with anxiety, and within minutes, their localized muscle twitching has “spread” throughout their entire body.
Has this happened to you?
Realize that ALS does not instantly “spread.” Though muscle twitching is an ALS symptom, the ALS websites often fail to add a very crucial detail:
This symptom is preceded by, and then accompanied by, “clinical” muscle weakness.
A fearful person who hits a website that actually includes this detail, however, won’t necessarily be relieved, because once they read this, they’ll then suddenly feel “weakness” in a twitching part of their body.
They’ll stand up and test it out, and sure enough, suddenly the area feels weak. This experience is called perceived weakness.
This is how the mind works.
But ALS weakness is serious; it’s not just a feeling of weakness or a perceived weakness.
You can perceive weakness in your leg all you want, but you’ll still be able to trot up a flight of stairs or run across the parking lot.
If you have ALS weakness, those stairs will be impossible to climb without struggling.
Exercise ranks high on causes of muscle twitching because lactic acid collects in the exercised area, and lactic acid and other byproducts of exercise can cause nerves to spontaneously fire away.

Freepik.com
In layman’s terms, the nerves are still buzzed from the exercise, and this buzzing can manifest itself one or two days after the exercise.
Anxiety causes twitching because fear signals to muscles to get ready for a battle.
The muscles rev up their engines and this causes twitching: The muscles prepare for flight or a fight.
This natural neurological response helped humans survive during primitive times; ancient man’s muscles needed to react quickly to an urgent situation (hissing snake, approaching animal, unexpected chance to catch a rabbit for food, etc.).
Other causes of muscle twitching include electrolyte imbalance, calcium and magnesium deficiency, medications, Lyme disease and dehydration. ALS ranks at the bottom of the list because it’s so rare.
Dr. Kantor is also President Emeritus, Florida Society of Neurology.
Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes
Source: http://www.mayoclinic.org/diseases-conditions/amyotrophic-lateral-sclerosis/basics/definition/con-20024397

Benign Fasciculation Syndrome: Causes and Solutions

If you’ve been diagnosed with benign fasciculation syndrome, you may still be experiencing a lot of panic as a result of what you’ve been through for the past several weeks or months.
This is because the symptoms of benign fasciculation syndrome can resemble, or seemingly resemble, symptoms of ALS and multiple sclerosis.
If you have benign fasciculation syndrome, you’re perhaps now wondering how to get rid of it, not to mention what the heck even causes benign fasciculation syndrome in the first place.
There are causes and solutions for benign fasciculation syndrome.
The causes are many and include anxiety. “Persons with anxiety or panic attacks have higher levels of excitatory neurochemicals, says Mary Dombovy, MD, a neurologist with Rochester Regional Health in New York.
“These neurochemicals cause the feeling of anxiety, increased heart rate, increased blood pressure and twitching.”
If your case of benign fasciculation syndrome has been caused by anxiety, then logic says you can cure benign fasciculation syndrome by managing your anxiety. The anxiety may or may not relate to fear of ALS or MS.
Anxiety over, for example, your job, may have initially caused some BFS symptoms.
But the symptoms of benign fasciculation syndrome went wild after you suspected (via the Internet) that BFS symptoms resemble symptoms of ALS and MS.

Shutterstock/ShotPrime Studio
A new level of anxiety set in and exacerbated your pre-existing benign fasciculation syndrome symptoms.
And since then, your body hasn’t had much of a rest from benign fasciculation syndrome.
One of the most effective treatments or even cures, for BFS, is TIME PASSAGE.
Because you know that once a certain period of time passes, what I call the grace period, you can be less panicky about ALS, as this affliction doesn’t exactly take its sweet time in wasting away at your body.
The first few months within the onset of benign fasciculation syndrome can be harrowing, to say the least.
I recommend buying a separate calendar and some sticky-stars or sticky colored circles about the diameter of a nickel.
Every morning, place a sticky on that day on the calendar. Before you know it, you will see rows of stickies, indicating time passage.
Before you know it, the entire calendar page will be full of stickies, indicating one month behind you.
And if you had something more alarming than benign fasciculation syndrome, you know that after 30 days, you’d probably be noticing some very bothersome symptoms, like difficulty holding your coffee cup or going down a staircase.
Benign fasciculation syndrome can have physical causes, such as:
1) medications
2) being taken off medications
3) viral infections
4) Lyme disease
5) calcium, magnesium and/or potassium deficiency
6) fatigue
7) hard exercising, and
8) no known cause.
If you’re taking medications, ask your doctor about side effects, or effects of quitting the medications, that may resemble benign fasciculation syndrome.
The solutions to benign fasciculation syndrome are clear once you establish cause.
But one thing’s for sure: BFS symptoms almost always become more pronounced when you worry about the condition.
Anxiety and hard exercising may be the top causes of benign fasciculation syndrome.
“The muscles are most likely overworked at this point,” says Kevin Plancher, MD, a leading sports orthopedist and sports medicine expert in the New York metropolitan area.
“The nerves that send impulses to the muscles become fatigued as well,” continues Dr. Plancher, “which can cause erratic firing of the muscles.”
Lactic acid buildup following exercise can also be involved. “It alters the way the muscles contract as well, possibly causing twitching.”
But the solution to benign fasciculation syndrome does NOT mean quit exercise!
Once you have retrained your mind to relax and recognize the symptoms of BFS for what they are — benign — you won’t mind these symptoms as a result of exercise.
In fact, you may even begin to use BFS symptoms as a way to confirm that you put in a great exercise session.
Stress management is another solution to benign fasciculation syndrome. Natural ways of managing stress include exercise and finding a new hobby.

Dr. Dombovy completed her neurology residency at Mayo Graduate School of Medicine. She is board certified in both neurology and physical medicine and rehabilitation.
 Dr. Plancher is founder of Plancher Orthopaedics & Sports Medicine, and lectures globally on issues related to orthopedic procedures and sports injury management.
Dr. Plancher is founder of Plancher Orthopaedics & Sports Medicine, and lectures globally on issues related to orthopedic procedures and sports injury management.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: medscape.com/viewarticle/804221_5

Doctor Describes what Clay Colored Stools Look Like

Do you keep seeing “clay colored” as a descriptor of stools on medical sites and wonder exactly what this refers to?
There’s a lot of misinterpretation as to what “clay colored” refers to, even though “clay colored stools” is commonly listed as a symptom for disease, including liver problems.
Definition of Clay Colored Stools
“Clay colored indicates light grey, not the dark color of a clay pot,” says Akram Alashari, MD, a trauma surgeon at Geisinger Medical Center in PA, and author of “THE POWER OF PEAK STATE.”
When we think of clay, what we envision will vary from one person to the next.
The flower pots that we see outside that contain flowers are made of clay.
What color are they? They are a dull orange, or even what could be described as a dull salmon, or a salmon-tan combination.
Fresh moist clay that you dig up in the ground appears to be a combination of tan/brown and grey, similar to the moist clay that a sculptor works with.
And this hue is not light; it’s more of a medium range.
So when a reputable medical site lists “clay colored” as a description for bowel movements, this actually refers to a light grey appearance.

This is what “clay colored” stools look like.
In addition to alcoholic liver disease, here are other causes of this light grey appearance, in no particular order:
1 Biliary cirrhosis. This form of liver cirrhosis results from damage and scarring of the liver caused by a problem with the bile ducts.
2 Benign or malignant tumors of the liver, biliary system or pancreas. Tumors can obstruct the bile ducts.
Bile, produced by the liver and stored in the gallbladder, gives BMs their normal brown color.
If a tumor blocks the bile ducts, bile can’t reach the intestines, leading to pale or grey stools.
3 Bile duct cysts. These are fluid-filled sacs that form in the bile ducts.
4 Narrowing of the bile ducts.These ducts become constricted, limiting or blocking the flow of bile into the small intestine.
5 Congenital structural problems with the biliary system.
6 Medications. Drugs like Maalox or Mylanta, which contain aluminum hydroxide, can sometimes lead to grey or clay color stools. So can Pepto-Bismol and some antibiotics.
7 Iron supplements. Iron oxide can discolor bowel movements.
8 Gallstones. The stones influence bile production and flow, which can turn bowel movements a clay color.

Dr. Alashari was formerly with Grand Strand Regional Medical Center in SC as an abdominal and critical care surgeon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/sukiyaki

Can Gallbladder Problem Cause Loose Orange Stools?

If you have loose orange stools, here’s why a gallbladder problem is not causing this.
“The color of stool normally is brown,” says Akram Alashari, MD, a trauma surgeon at Geisinger Medical Center in PA, and author of “THE POWER OF PEAK STATE.”
“The reason for the brown color is the presence of bile metabolites in the stool.
“Gallstones that pass from the gallbladder to the common bile duct can potentially cause bile duct obstruction.
“This will lead to absence of bile flow to the intestine and can result in a pale colored fatty stool and jaundice.”
Now, what is meant by a “pale” colored stool? This refers to “light grey color,” says Dr. Alashari.
“Stool can be gray or clay-colored if it contains little or no bile. This is referred to as steatorrhea.”
“Clay-colored” refers to a light grey hue, says Dr. Alashari, and not (as some people might assume) the dull orange color of a flower pot.
“However, fatty bowel movements may have a “light orange tinge to it, like fatty oil droplets.
“(Kind of like the color if you had cooked meat, put in the fridge; the next day there is this fatty layer around it; looks pale/light orange tinge).”
He adds: “Also, ‘fatty’ stool is characterized by being malodorous [foul odor], associated with oil droplets, and floats on the surface of the water in the toilet.”
So as you can see, if you’re perceiving what you’d describe as loose, orange stools in the toilet bowl, this probably is not being caused by a problem with your gallbladder.
Orange should not be equated with a light grey.
Orange diarrhea can have harmless as well as serious causes.
Dr. Alashari was formerly with Grand Strand Regional Medical Center in SC as an abdominal and critical care surgeon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why Your Hair Smells Burnt: Causes, Solutions

A dermatologist explains what can cause hair to smell burnt and what the treatment is for this most unpleasant problem.
Does your hair have a burnt smell to it? What can cause this and what can be done about it?
“Burnt hair is a condition that relates to a burning smell in hair,” says Dr. Joel Schlessinger, MD, board certified dermatologist and cosmetic surgeon with a private practice in Omaha, NE.
“This is generally due to over-processing of hair, combined with too much heat on the same hair.
“Once hair has been damaged by either heat or chemicals it becomes thinner and open to further damage.
“Once this damage occurs it is easier for a ‘burnt smell’ to set in and be retained.”

Shutterstock/Vladimir Gjorgiev
Solutions to a Burnt Odor in Your Hair
Dr. Schlessinger explains, “There are many things to avoid if hair has a burnt smell, but the most important of these to avoid is being too close to a curling iron or wand.
“If and when hair needs to be dried it is important to avoid too high of a heat on the drier and always hold the drier away from the hair.
“Certain oils and nourishing shampoos will offer benefits to regain the natural smell of hair, but in the worst case scenarios it will simply be months until the damaged hair has the chance to grow out (usually, hair grows about an inch per month).
“During this growth time it is essential to avoid trauma and heat/chemicals.”
If a curling iron is used on hair that isn’t completely clean or dry, this can cause a problem.
When the heated device comes into contact with hair that has oils, hair products or residue, it can produce a burnt or unpleasant odor.
The heat can cause these substances to actually burn slightly, releasing a smell.
Additionally, if the curling iron itself isn’t cleaned regularly, any buildup of product or residue on the iron can contribute to a smell that transfers to your hair.
To minimize this issue, ensure that your hair is clean and dry, rather than “oily and grimy,” before using the curling iron, and regularly clean the iron to remove any buildup on it.
 Dr. Schlessinger, founder of LovelySkin.com, has 25+ years of experience treating many skin conditions including melanoma. He’s founder of the Advanced Skin Research Center, a clinical facility that investigates new medications and treatments.
Dr. Schlessinger, founder of LovelySkin.com, has 25+ years of experience treating many skin conditions including melanoma. He’s founder of the Advanced Skin Research Center, a clinical facility that investigates new medications and treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Does Your Hair Smell Like a Wet Dog?

A dermatologist explains why your hair smells really bad, like a wet dog, and how to get rid of this problem.
Peeuww ! Does your hair’s smell remind you of a wet dog? The natural scent of hair should be pleasant, almost sweet.
Its natural fragrance originates from the sebaceous glands — there’s one of these glands in each hair follicle.
The glands secrete an oily substance called sebum, and it makes its way to the surface of the scalp.
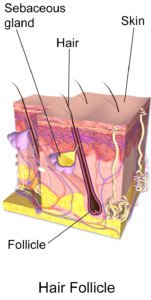
James Heilman, MD, CreativeCommons
Once there, it then makes its way onto the visible hair shaft and down the length of the hair as you brush it; the brushing (or combing) distributes the beneficial sebum all over your hair.
But a certain problem can override the scent of your hair’s natural oils, making it stink like a wet dog or just be plain smelly.

Shutterstock/Marian Fil
Cause of a Really Bad Smell in Your Hair Despite Frequent Washings
“Smelly hair is a problem that occurs after bacteria (or fungus) becomes present in the scalp,” says Dr. Joel Schlessinger, MD, board certified dermatologist and cosmetic surgeon with a private practice in Omaha, NE.
“While antibiotics can treat and/or cure infections on the body, the scalp and hair remain incredibly resistant to antibiotics, as the hair can act as a reservoir for these organisms.
“Regular shampoos can do quite a bit to calm frizzy hair, preserve luster or clean off oils, but the last thing (and perhaps the ‘never’ thing) they do is to deep clean bacteria and other organisms.”
How to Get Rid of the Stink in Your Hair
Dr. Schlessinger continues, “This means that it is perfectly possible to wash hair thoroughly and miss the main thing in a situation of ‘smelly hair’ — the bacteria! For this reason, a different approach needs to be taken.
“For one, a sulfur-containing shampoo can help. There are many of these over the counter in drugstores.
“I recommend a bleach-containing shampoo, CLn (lovelyskin.com/o/cln-shampoo), that not only cleans but disinfects.
“Apocrine sweat glands magnify the problem, as they contain microorganisms that, when excreted, have a smell.
“These aren’t something that can be switched off easily, and are the same cause of armpit smells.
“In the worst of cases it may be worth considering Botox injections into the scalp area if the smell isn’t contained with the treatments mentioned here.
“But these are expensive and would not be covered by insurance for the scalp area.”
Washing
“It is important to note that hair should be washed daily,” says Dr. Schlessinger.
“In the case of ‘smelly hair’ it is necessary to wash daily and preferably prior to leaving for the day.”
See if daily washing works for you. For some, washing every other day or so may be a better option.
Wet dog odor still persists?
“If these measures don’t work, it may be wise to see a dermatologist, as there may be a role in antibiotics or antifungals.”
Dr. Schlessinger, founder of LovelySkin.com, has 25+ years of experience treating many skin conditions including melanoma. He’s founder of the Advanced Skin Research Center, a clinical facility that investigates new medications and treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Benefits of Having a Shy Child: Nothing Is Broken!

Trying to “fix” your child’s shyness may cause more harm than good.
I recently read in an advice column of a woman who complained that her husband would make his child sit in the laps of people the boy hardly knew, in an attempt to get the youngster to overcome shyness.
This is outrageous. The blaring reason is that it sends the message to the child that he has no say-so or domain over his body, and that if adults want to physically handle him against his will, he must allow them to do it without a fight.
This mental conditioning will prime this child for being a very easy victim of sexual abuse or molestation, should the town pedophile ever catch him alone.
Many parents are overly concerned when they realize their child is shy.
Now, if your child is so shy that he or she runs for cover whenever a friendly stranger appears within 100 feet, then this is a problem that needs attention.
But if your kid is showing signs of simple typical shyness, then relax and don’t panic.
Did you know that kids who grow up to be extroverted, gregarious, very social teens are more likely to do drugs?
The extroverted, social child is more likely to be influenced by peer pressure and following the crowd.
You may think that the shy kid will want to do anything to be popular, and this may be true in some cases.
But that extrovert will be in far more contact with many more people, and the more people, the more likely she’ll encounter ones of bad influence, and extroverts tend to worry a lot about what other people think.
Kids who keep to themselves, on the other hand, often don’t give a rip what other people think. Now again, who is more likely to be swayed by peer pressure to do the wrong thing?
Introverted, shy teens are rarely the ones smoking in the john with a group of friends between classes.
I know that in my junior high and high school, the “bad” kids usually had a lot of friends. The shy child would rather be in the library reading or listening to music in solitude.
Who is more likely to be lured into a car by a sex offender?
Well, this is a very interesting issue to look into. “An extrovert may have a lot of self-confidence and wouldn’t go with a pedophile,” says Carole Lieberman, MD, a forensic psychiatrist and author of Bad Girls: Why Men Love Them & How Good Girls Can Learn Their Secrets.
“But, a child who has a psychological problem that makes her gregarious because she’s needy for attention would be vulnerable to a pedophile. Similarly, a shy child who is simply very cautious, would be extremely hesitant to go with a pedophile.
“But, a child whose shyness is actually reflective of an underlying depression or mental illness would be vulnerable to a pedophile.”
Just using common sense, you might see that a child who runs over to meet unfamiliar strangers on the street (e.g., steam cleaning man, neighbor’s new housekeeper, exterminator, movers) is anything but shy, and could easily be talked into entering a stranger’s van to view the puppies in the basket (which really aren’t there, if you know what I mean).
Have you yourself ever tried to get a shy kid you don’t know to follow you? Good luck. Pedophiles don’t like to work hard; they go after kids who smile warmly at them and who easily approach them.
What kind of message do you send your shy child if she knows you are trying to fix or correct her shyness? She’ll feel defective and she’ll think you’re not happy or accepting of her.
If you want to “bring out” your kid or get him out of his “shell,” then don’t order him to say “Hi” to every stranger.
He is simply obeying your command and this will not produce an internal ease with strangers.
Do not make her kiss or receive hugs and kisses from strangers or people she hardly knows, including relatives.
Instead, enroll them in martial arts school, encourage them to develop inborn skills and show value to their opinions.
Dr. Lieberman says that shy children tend to be more reflective than their outgoing counterparts.
She also explains, “Shyness can be a plus, when it directs a child towards serious career goals, for example.
“But, parents should try to help their children become more comfortable with others by involving them in playdates and after-school activities from the time they are very young.”
PS: It’s not the shy kids who talk nonstop in a loud, annoying voice and constantly interrupt and act pushy and spoiled.
 Dr. Lieberman analyzes the psychological impact of world events, as a guest and/or host on all major media outlets. Her appearances include “Larry King Live,” “The Today Show,” “Good Morning America,” “Entertainment Tonight,” CNN and Fox News.
Dr. Lieberman analyzes the psychological impact of world events, as a guest and/or host on all major media outlets. Her appearances include “Larry King Live,” “The Today Show,” “Good Morning America,” “Entertainment Tonight,” CNN and Fox News.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

Benign Causes of Bilirubin in Your Urine

If bilirubin has been found in your urine, is there ANY reassurance that this might have a benign cause?
“Bilirubin is not normally found in the urine,” says Akram Alashari, MD, a trauma surgeon at Geisinger Medical Center in PA, and author of “THE POWER OF PEAK STATE.”
“A positive test for urine bilirubin confirms that any raised plasma levels are from conjugated hyperbilirubinemia.
“Causes of bilirubin in the urine include hepatocellular [liver] dysfunction and any cause of bile duct obstruction [which, unfortunately, can include cancer of the bile ducts, gallbladder, liver, pancreas and metastases from distant primary cancers].”
What is meant by “benign”? To some people, this means anything but cancer.
To others, it means not only that, but also non-serious.
With that said, some individuals, then, will consider the following as benign causes of a bile duct obstruction — which can lead to bilirubin in the urine:
Bile duct inflammation
Cysts
Trauma
Abnormal narrowing of the biliary ducts
Pancreatitis
Parasites
But most causes of biliary obstruction are from the presence of gallstones.
Additional Benign Causes of Bilirubin in the Urine
“Urine bilirubin levels may be elevated by medications including barbiturates, birth control pills, steroids and diuretics, and reduced by medications including ascorbic acid and indomethacin,” says Dr. Alashari.
“Urobilinogen and etodolac [arthritis drug] may cause false-positive bilirubin results, while uric acid, nitrite and extended exposure to direct sunlight may cause false negative results.”
Dr. Alashari was formerly with Grand Strand Regional Medical Center in SC as an abdominal and critical care surgeon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Guschenkova

Can Gallbladder Removal Cause a Noisy Stomach?

Have you had your gallbladder removed and are now experiencing strange, funny sounds that seem to be originating from your stomach?
“I am unaware of this condition. Have not read about it or seen it in the clinical setting,” says Akram Alashari, MD, a trauma surgeon at Geisinger Medical Center in PA, and author of “THE POWER OF PEAK STATE.”
So if your stomach is making noises that seem to have arisen only after you’ve had your gallbladder removed, perhaps it is just a coincidence.
Here is the link to an article that you will be interested in: Causes of Stomach Noises
Dr. Alashari was formerly with Grand Strand Regional Medical Center in SC as an abdominal and critical care surgeon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}