

How to Get Your Child to Like Martial Arts Lessons

Does your child balk at taking martial arts classes? Here are sure-fire ways to get him or her to look forward to every lesson and eagerly want to learn more and more.
If your child doesn’t like the idea of taking karate or other-style martial arts lessons, this might possibly be traced to some negative perception of the martial arts that he or she has picked up from somewhere.
It’s your opportunity as a parent to undo this perception.
I have studied martial arts in a variety of schools over the years and have a karate brown belt.
If your child is afraid or reluctant to take karate lessons, never become authoritarian with a growling “Well you’re gonna take karate whether you like it or not!”
The goal is to make your child feel good about martial arts — so good, in fact, that they never want to stop attending classes — even as an adult.
Never tell your child they must take karate “because I said so.”
This won’t cut it, and relying on this easy, quick response will fail to educate kids about the importance of martial arts.
“I’m afraid of getting hurt.”
Explain that more common physical activities, such as bike riding and playground equipment, have a much higher risk of injury.
Physical activities that involve wheels or a lot of running also rank high for injuries.
And according to the Centers for Disease Control, football, baseball, basketball and soccer comprise 80 percent of ER visits for kids 5 to 14.
Other high risk sports are gymnastics, figure skating, skiing and equestrian.
Tell your child that unlike many other sports, in karate, students wear protective padding, and work out on mats (stay away from martial arts schools that don’t use mats or a padded floor).
“I don’t want to fight.”
Explain that there is no angry fighting in martial arts, but there may be fighting on a basketball court or baseball diamond when kids get into arguments.
Learning self-defense, and sparring according to strict rules, are not the same as “fighting.” Tell your child that anger is not permitted in karate class.
“I don’t want to get beaten up.”
Explain that fighting, anger and hostility are forbidden in karate schools, and that karate lessons will help your child defend himself or herself against school bullies.
Ask your child why they are reluctant or afraid to study martial arts.
Chances are, they have seen martial arts in a video game or movie and thinks it’s full of violence.
However, they may also be fearful of failure.
Explain that in martial arts, there is no pressure to score points or make a perfect shot, and that it will be fun. Act enthusiastic.
If your child is still leery, ask the instructor to allow you and them to observe several classes first.
If your child, after you have tried all the tactics in this article, still feels discouraged about taking karate lessons, don’t give up.
Sign them up anyways; martial arts is something that your child will have to do because it is very good for him, just like kids must do other things they don’t want to do, like homework and taking baths.
But remember, always act enthusiastic rather than “because I said so!”
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Kaderov Andrii
Child Asks Embarrassing Questions in Public to Disabled Person?

Here’s how to respond if your child asks an “embarrassing” question in public to a disabled person.
If your child has embarrassed you with questions to disabled people, or reactions to disabled people in public, a man who was born without arms has advice for how parents should deal with these tricky situations.
Chet McDoniel grew up without arms, and has very short legs. When he’s in public, people, including children, will stare, and sometimes there are questions, comments and reactions.
If your child has loudly called your attention to a person with a disability; or your curious kid has actually approached a handicapped person and inquired about the disability, McDoniel offers superb tips in how you, the parent, should respond.
The first and foremost rule for parents when their child blurts something about the nearby handicapped person is DO NOT SPANK.
McDoniel, father to two, explains that, though the parent should not ignore the child who spots an obvious disability, he also believes that parents should never “rebuke the child openly/loudly for their behavior.”
McDoniel continues: “I have even seen parents hit or spank their children for the outburst. I can only assume that the parent is embarrassed, and yes, outbursts like that need to be corrected.
“However, I believe that type of correction only serves the purpose of furthering the child’s fear of people who look different than they do.”
If your child spots a disability, consider this an opportunity to educate about the disability, rather than punish for being curious about handicaps.
There are general ways for parents to respond to kids who have noticed a disabled individual, and there are also specific ways parents can react, based on the child’s age and the specific behavior of the child. First here is McDoniel’s general guideline:
“If the parent has the opportunity, I recommend for them to stop what they are doing, get eye-to-eye with the child, and explain that some people look different, but that does not mean they aren’t people, too.
“Many times, with this reaction, I’m able to speak to both the parent and child, which reinforces what I am saying because mom or dad can interject when needed.
“Even better, when the parent involves me in the conversation, I get a golden opportunity to share God’s love with both the parent and the child. Even though I may look different, God still loves me in every way that He loves you.”
Specific situations involving kids who make comments about disabled people in public:
Child is preschool age and loudly blurts, “Look Mommy, that man…”
“Never stifle the child’s curiosity. Preschool children who have outbursts like this are truly surprised by what they see.
“They don’t mean it as an insult, but rather, that they are trying to reconcile what they are seeing with what they know about the world around them.
“Kneel down and talk about people who look different than we do. Unfortunately, many parents try to quiet the child, which will lead to more outbursts, rather than simply talking out the issue.”
Child is preschool age and can’t stop staring (though says nothing).
“Same kind of thing … while it’s important to talk to them about staring, a parent must let their child know that there is nothing to be afraid of.”
Child is grade school age and keeps staring, but says nothing.
“At this stage, I fear the parent has not followed the above advice and has allowed the child to treat others who look different as spectacles instead of allowing the child to know others as humans, first. It isn’t too late, though.
“Again, I would say that you cannot allow the child to continue to stare, but take the opportunity to have the child tell you their feelings about the person they saw.
“Then, work through those observations and feelings to help them understand why staring is inappropriate … and also why people who look different should be treated with kindness as they would treat anyone else.
Child is grade school age and actually goes up to person with disability and innocently asks about the handicap.
“I absolutely love this situation. It gives me a chance to tell the child about myself and to break down the communication barrier. Never apologize for the child’s curiosity.
“This is a perfect teaching opportunity, and it will allow the child to get to know the handicapped person.
“You might approach the person before the child does in order to ask if it’s okay for the child to ask a question.
“While I have never met a person with special needs who would be rude in this situation, I can imagine that such a person does exist, and you do not want the child to have a negative encounter at this stage.”
A parent’s instinct, when a child goes over to a disabled person and asks, “What happened to your arms,” or, “Why can’t you walk?” is to grab the kid by the arm or shoulder, mutter something like “Johnny! How can you?!” and then pull the kid away from the handicapped individual.
Now think about this for a moment. What message did you just send to an impressionable youngster?
You just made it far more difficult for him to ever feel comfortable or at ease around someone who’s handicapped, and your reaction won’t motivate him to befriend any disabled kids at school; he’ll feel it’s “wrong” to go over to them.
Child is grade school age and behaves fearfully or uneasily.
“Never ignore this issue. I have had grade school children who have been terrified of me because of the way the parent has either ignored or punished these behaviors.
“It’s ridiculous for a child to be afraid of a person with special needs, but the behavior can always be traced back to the parent and how they handled the child’s interactions with handicapped people.
“Take the time to reassure the child in that moment, and spend some time back at home working on building confidence.”
Grade school or junior high age kids are snickering amongst each other, pointing, whispering, giggling.
“At this age, if they are doing these kinds of things, I fear that parents have failed.
“Unfortunately, about the only thing you can teach at this point is to correct the behavior.
“Hopefully, once they mature, they will value all kinds of people enough not to do these kinds of things. That’s why it’s important to teach early.”
Child is junior high or teenager, and reacts in an alarming way with, “Oh my God, Mother, oh God, that man has no arms…(or whatever the situation)…” The adolescent or teen may let out an expletive and appear very distraught and upset.
“A parent cannot allow this kind of behavior. At this age, they know what is appropriate in a public setting, and if they won’t value the handicapped person enough not to make this outburst, at least teach them to control their reaction.
“Again, since the child wasn’t taught to respect early on, I fear you’ll just have to wait until maturity hits for this type of behavior to stop.”
Read more about inspirational speaker Chet McDoniel, author of “I’m Not Broken: You Don’t Need Arms to Be Happy.”
Visit Chet’s site at: chetmcdoniel.com
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer. .
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer. .
Legs Suddenly Too Weak to Stand After Playing Volleyball?

Have you ever been sitting out during sports play and then tried to stand and couldn’t due to “dead” legs?
This isn’t about your legs “falling asleep” due to a nerve being compressed from sitting in a scrunched position.
It’s about trying to get up, and your legs, particularly your quadriceps, just can’t support you, and you collapse back down.
I had a doctor weigh in on this, but before I tell you what he said, you should know that this exact situation once happened to me.
After training in volleyball with a volleyball club, I sat out because we were rotating in groups. I felt fine.
Then when it was time to stand, my legs just folded. My quadriceps felt very fatigued and weak, and I couldn’t get up.
Someone had to lift me off the floor and carry me to another part of the gym, where I just sat there to let this sudden leg weakness run its course.
Cause of Weak Legs, Inability to Stand, after Sports Play
“I would suspect that the culprit was lactic acid,” says Marc I. Leavey, MD, a primary care physician with 40-plus years of experience.
“During rigorous exercise, the muscles need energy faster than the normal metabolic pathways can provide it.
“An intermediate compound of metabolism, lactic acid, is produced as a means of delivering that energy without the use of oxygen.
“After a few minutes, it can build up, and the body responds to that buildup with burning or weakness in the muscles being exercised, such as the legs in volleyball.
“So a period of intense exercise may be followed by a buildup of lactic acid and an acute loss of strength and function.
“After a period of rest, which may be just 10 to 20 minutes, the lactate has been metabolized and all is back to normal.”
Note: I had not injured anything (no pulled hamstring or quadricep). This extreme weakness never occurred again, even though for years after, I continued to play at a very competitive level.
Leg work in volleyball is not the same as in basketball, tennis and soccer.
Though basketball involves a lot of jumping, keep in mind that in volleyball, along with the jumping is also a lot of deep hip flexion (squatting), from which the player must spring up from in different directions to pass balls.
Prevention
“You can help prevent this situation by staying adequately hydrated, being sure to practice good breathing techniques, and being aware of your body’s condition,” says Dr. Leavey.
“If you start feeling weakness or burning in a group of muscles or an extremity, don’t work through the burn; stop and rest.
“Weakness or discomfort that lasts more than a short time may be due to micro-tears in the muscles involved, and is a different type of process.

Dr. Leavey was formerly with Mercy Medical Center in Baltimore, MD, where his focus was primary care and internal medicine. He has a blog, STRING OF MEDICAL PEARLS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/P Stock
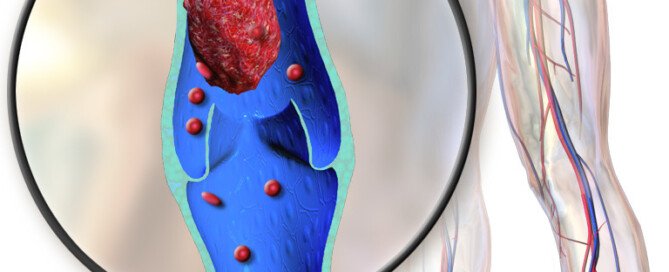
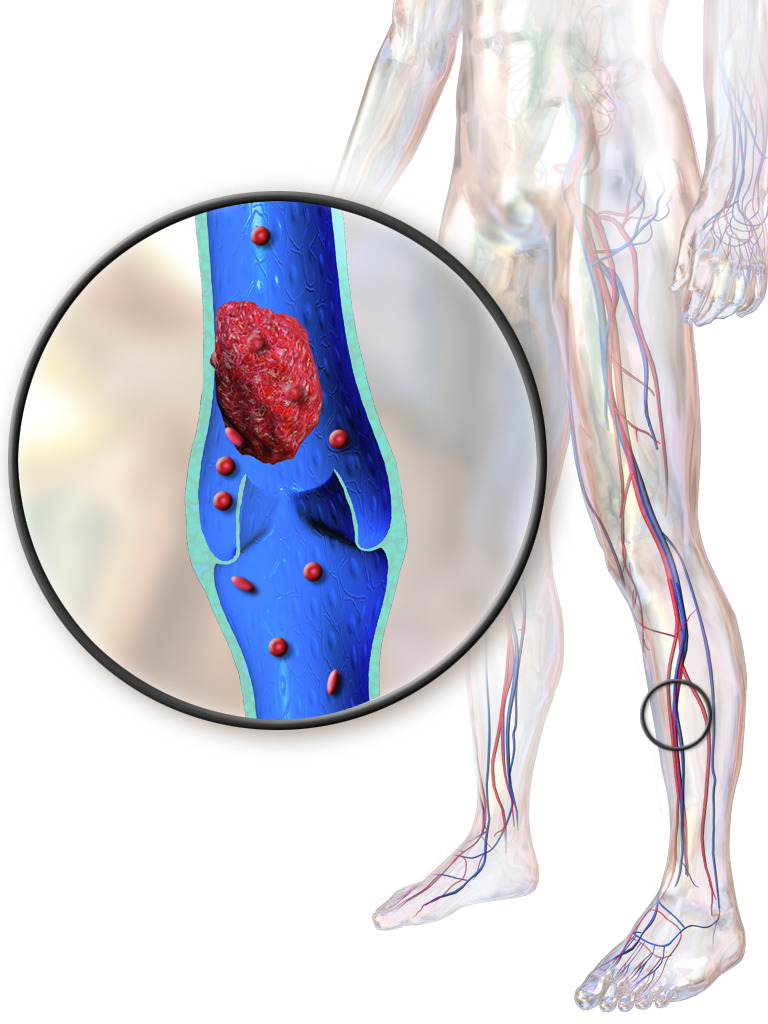
DVT Prophylaxis Duration after Hip Fracture Surgery

How long should DVT prophylaxis (prevention) be following hip replacement surgery to repair a fracture?
Unfortunately, there does not exist a be-all, end-all answer to this question.
Joint replacement surgeons don’t even agree on which anticoagulant drug to use.
“There is no right answer when it come to DVT prophylaxis,” says Kamala Littleton, MD, board certified orthopedic surgeon with Orthopedics and Joint Replacement at Mercy Medical Center, Baltimore, Maryland. Dr. Littleton specializes in joint, hip and knee replacement and reconstruction.
She continues, “We tend to use Coumadin for two weeks after surgery, then aspirin twice a day for an additional four weeks.
“However there are times when I just use a very low dose of Coumadin, so nothing is written in stone.
“If a patient is very high risk for PE or DVT, we will have the vascular surgeons place a temporary IVC filter.”
Hip fracture repair surgery (replacement with hardware) elicits a higher risk of deep vein thrombosis than does the elective hip replacement surgery which people have to mitigate the pain of osteoarthritis.
However, if the THR is performed with an anterior (front) entry, rather than posterior (back), this reduces the DVT risk, relative to the posterior approach.
Nevertheless, the DVT risk is still high when compared to other major surgeries, and research into the duration of the prophylaxis is intense and ongoing:
“The American College of Chest Physicians guidelines strongly recommend extending prophylaxis to up to 35 days for total hip replacement and hip fracture.” (ncbi.nlm.nih.gov/pmc/articles/PMC3195664/)
“Symptomatic VTE continues to be reported in patients within 3 months after surgery.” (ncbi.nlm.nih.gov/pubmed/21774881)
“As risk of VTE persists for up to 3 months after surgery, patients at high risk for postoperative VTE may benefit from extended prophylaxis…” (Chest. 2003 Dec;124(6 Suppl):386S-392S)
A lot of research shows that the risk of DVT following joint replacement surgery (such as hip) persists for 90 days out, even if the patient is mobile.
Nevertheless, there is no standard protocol, or universally accepted protocol, for just how long the DVT prophylaxis should be.
There’s not even a general consensus for a time range, such as four to six weeks, or seven to 10 days, or two to three months, etc.
Therefore, the proper duration of DVT prophylaxis following hip or other joint surgery is at your doctor’s discretion.
 Dr. Littleton offers years of experience and specialized training to perform anterior hip replacement as well as MAKO knee resurfacing and knee replacement. She also performs shoulder surgery.
Dr. Littleton offers years of experience and specialized training to perform anterior hip replacement as well as MAKO knee resurfacing and knee replacement. She also performs shoulder surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus/CreativeCommons

Is Daytime Sleeping Part of Hip Replacement Recovery?

How much daytime sleeping is too much for the elderly hip replacement patient who just returned home?
Restorative sleep is a wonderful thing, and sleep deprivation is linked to a myriad of health ailments.
But too much of a good thing can be quite harmful, and sleeping in the daytime, when you already sleep overnight, is no exception to this rule.
How does daytime napping, however, apply to the elderly hip replacement patient?
“Daytime sleeping is fine,” begins Kamala Littleton, MD, orthopedic surgeon with Orthopedics and Joint Replacement at Mercy Medical Center in Baltimore, Maryland. Dr. Littleton is board certified and specializes in joint, hip and knee replacement and reconstruction.
“The fracture and the surgical intervention take a lot out of older patients so they need more rest,” she continues.
“They do need to get out of bed, exercise and walk several times a day. Spending most of the day in a recliner rather than bed is preferred.”
What this means is that the recliner is preferable to the bed, by far. But it does not mean, literally, that the older hip replacement patient should spend most of the day in a recliner. They should be up and about as much as they can tolerate.
The comfort zone is the recliner. The elderly hip replacement patient should be encouraged to leave this comfort zone.
This doesn’t mean they shouldn’t take rests including some snoozers. But too much recliner time, and especially bed rest, bring some serious risks.
“Too much time in bed puts one at risk for blood clots and pneumonia. but I have no problem with napping,” says Dr. Littleton. And what is a nap? A nap may be 20-30 minutes.
If the nap is for too long, the patient will start entering a deeper sleep cycle, and then when they finally get up, they’ll feel groggy and listless.
Several 20-minute naps throughout the day, for example, are beneficial. This should never transform into excessive sleeping or bed rest. Snoozing in a chair, rather than a bed, is less likely to result in an extended period of sleep.
Too much sitting, even in an upright chair, is a bad thing for the elderly hip replacement patient, because it will force the soft tissues around the hip to be in a prolonged “L” position (shortening the muscles), so that when the patient finally stands up and walks…there may be a lot of pain from the stiff, retracted muscles being stretched.
Excessive daytime sleeping, as mentioned, increases the risk of pneumonia, and via more than one pathway.
One of those pathways is that the lungs, being in a lying or reclined position, and even in an upright sitting position, are not in their ideal state in which they can open up with optimal efficiency and take in air.
In fact, the elderly hip replacement patient may be prone to sitting slouched, “crumpling” up the organs.
Being up and about more frequently opens the abdominal cavity up, giving the lungs more room, making breathing easier.
Dr. Littleton offers years of experience and specialized training to perform anterior hip replacement as well as MAKO knee resurfacing and knee replacement. She also performs shoulder surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Hip Fracture Patient Traits that Help Regain Independence

About one-third of hip fracture replacement patients regain pre-surgical independence.
What is different about this group when compared to the two-thirds who fail to get back their independence?
This isn’t a comparison of total hip replacement (THR) patients who had elective surgery for osteoarthritis.
This compares those who underwent the THR for hip fracture with each other: the ones who regained their independence vs. the ones who did not.
“When a person fractures their hip, sometimes it is just a fluke: dog gets under them, crack in the sidewalk, etc.,” says Kamala Littleton, MD, orthopedic surgeon with Orthopedics and Joint Replacement at Mercy Medical Center in Baltimore, Maryland. Board Certified, Dr. Littleton specializes in joint, hip and knee replacement and reconstruction.
Dr. Littleton continues, “Others are at risk. They are weak, have neurological balance issues, dementia, have heart or lung conditions which can make them unsteady (shortness of breath, A-fib, congestive heart failure, poor heart function), which cause them to fall.
“Often (especially in the city) they live in very cluttered houses with many stairs, narrow hallways and throw rugs. They have lived in these places for years (often alone) and miraculously have managed.
“They are a bit like a ticking time bomb. The fall and subsequent fracture are the explosion.
“They can’t use a walker in their houses, can’t navigate stairs, spend time in rehab or nursing facilities and just can’t make it back to independence.”
Though no hardcore data exists on the precise elements that differentiate the hip fracture patients who recover fully from the ones who remain in nursing care or permanently on a walker or cane, it’s reasonable to say that the ones who fully recover have few to zero comorbidities (e.g., dementia, congestive heart failure).
But suppose we have a patient who has only brittle bones and is very de-conditioned, but has decent heart functioning and normal neurological status.
She quickly rises from a chair and hurries to answer the phone, and along the way, a leg gives out and down she goes, fracturing a hip.
If this person has always hated exercise, has always led a sedentary life, has always dreaded the idea of moving enough to trigger a sweat or increased heart rate—and toss in a little stubbornness, pre-existing mild depression and/or baseline sub-rational thinking—then you may just well have the perfect storm for a patient who never regains independence following hip fracture repair.
Another factor that can taint recovery efforts is when the patient, when it’s time to return home, ends up in an environment that’s not conducive to recovery.
An example would be a spouse who’s an enabler—who fetches everything his wife asks for instead of encouraging her to walk to get what she wants.
Or, the spouse may not be proactive. An example is if the patient announces she doesn’t want home physical therapy, and the husband goes along with this instead of wearing the pants.
I know a woman whose mother fractured her hip at age 88. After surgery and a little rehab center stay, the patient returned home—which was her daughter’s house, and refused physical therapy.
The daughter told her she was going to make up a list of nursing homes for her mother to choose from. This casual announcement by the daughter inspired the mother to commit to therapy, and she recovered.
When a patient refuses therapy, the family must do everything possible.
If the patient still isn’t motivated, the family should re-evaluate the environment they’re providing: Is it enabling?
This is particularly important if the surgeon and physical therapist have given NO medical or mechanical reason for why the patient can’t regain independence following the hip fracture repair.
Of course, the presence of psychiatric pathology will likely interfere.
People undergoing hip replacement for a fracture will also need to have their thyroid levels checked post-surgery, as major surgery could alter thyroid levels, especially in a person with pre-existing thyroid disease.
Unchecked levels can cause cognitive impairment, depression, sleepiness and/or weakness.
Dr. Littleton offers years of experience and specialized training to perform anterior hip replacement as well as MAKO knee resurfacing and knee replacement. She also performs shoulder surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
Powerback Rehab, Lakewood CO: Terrible for Elderly Patients

Here is my ONE-STAR review of Powerback Rehab in Lakewood, CO for hip replacement therapy.
Do not let your loved-one go to this place of low quality rehabilitation.
Several years ago both my parents stayed at Azura rehab, which I gave a good review for.
Since then ownership changed to Genesis Healthcare: hence the name change to Powerback Rehab. Here is my review!
Summation of Review of Powerback Rehab in Lakewood for a Hip Replacement Patient
• Physical therapy six days a week for 45 minutes, once per day
• Occupational therapy six days a week for 30-40 minutes, once per day
• This means on Saturday and Sunday they get only one or the other.
• Zero programs outside of therapy to get the patients up and moving.
This is a serious issue for non-compliant, stubborn or depressed patients, or those with impaired judgment stemming from lingering effects of general anesthesia or some other cause.
• Patients have opportunities to get in their walking when venturing to and from their bathroom and the dining hall, but for patients lacking motivation (for the reasons cited above), essentially the only walking they’ll do is that during therapy.
This means outside of therapy, patients are left to their own devices.
• They may be lying in bed all day long or sitting like a blob for hours on end in their rooms.
• Patients with initiative or self-starting capabilities may progress fast, as they will want to walk at every opportunity, including summoning a CNA to accompany them beyond just the walks to the dining hall or bathroom. Powerback, then, benefits only self-starters with sound judgment.
• It’s so crucial for hip (and knee) replacement patients to walk, walk and walk.
• My mother spent a lot of time in bed sleeping. Though Powerback Rehab offers activities like bingo, fruit and ice cream socials and someone who comes in with a “therapy” dog, these activities do not necessarily get a patient to walk.
CNAs at Lakewood Powerback Rehab
Watch out here. The CNAs have the most interaction with patients, and are NOT trained to be proactive with them.
Typically they’ll ask, “Do you want to be wheeled or walk?” when it’s time to accompany the patient to the dining hall or bathroom.
Though some patients cannot walk, others can and SHOULD. A non-compliant or judgement-impaired patient may answer “wheeled,” and the CNA will oblige, rather than recognize the need to encourage the patient to walk.
Before you assume that a CNA won’t be able to change a stubborn patient’s mind, there was one particular CNA at Powerback Rehab who could easily get my resistant mother walking to the dining hall or bathroom — because she was proactive.
A second CNA also took this approach and got my mother up and about. The rest were like robots or failed to recognize the detriment of the “I want to be wheeled” option.
Powerbak Rehab CNAs are NOT required to encourage patients, who can and should walk, to do so.
The isolated gems who actually DO this simply reflect the law of averages: In any group of CNAs there’s bound to be a few who are proactive.
Two of the CNAs had thick accents and spoke rapidly. I had to peel my ears to decipher them.
I cannot understand why a facility, in which most of the patients are elderly (and thus have poor hearing) would hire CNAs with such poor pronunciation of English. Powerback Rehab of Lakewood, Colorado, really misses the boat.
My mother couldn’t hear them half the time and kept asking them to repeat things.
They lacked the smarts to speak s-l-o-w-l-y and instead would repeat in their rapid, thick accent.
Powerback Rehab of Lakewood, Coloraod obviously failed to train them in how to speak to the elderly hearing impaired.
It’s not illegal for a facility with so many hearing-impaired patients to refrain from hiring someone on the grounds that they cannot speak clearly.
Powerback Rehab in Lakewood is very understaffed with CNAs.
I also witnessed at least a few times the CNA on assignment for my mother failing to receive the signal from my mother’s call button. Often it took them a while to respond (due to the understaffing).
Fall Risks
My mother soon made it known she was very prone to using her walker without assistance, even though she was given strict orders to summon for a CNA.
This made her a fall risk. I pointed this out numerous times, but staff didn’t show much concern, citing that laws prohibited them from using bed or chair alarms for a patient who didn’t want them.
Maybe this is true, but there was no program in place to guard against my mother falling.
Fall risks following hip replacement surgery are common, and I ended up having to watch her like a hawk, then keep my fingers crossed when I wasn’t there.
Nurses
One of the nurses could barely speak English. Why would Lakewood Powerback Rehab hire a nurse, whose English was so bad that even I, with my good hearing, had difficulty understanding, to work with predominantly elderly patients who — as everyone surely knows — collectively have poor hearing?
When I needed whichever nurse was assigned to my mother per the shift, it was usually difficult to find her or him.
Yes, there are other patients, but I got the sense that Powerback is understaffed in the nursing department.
Occupational Therapy
The two sessions I witnessed were a joke. For the first session I witnessed, my mother did only one thing in the therapy room: sitting at an arm-pedaling machine.
For the second session, she was shown how to use a device to put on a sock, then taken to that arm pedaling machine.
This second session was 30 minutes, even though the prior one lasted 40 minutes.
The second therapist kept speaking in a soft voice. A smart therapist will ask the patient if there’s any hearing loss and will quickly detect if the patient was truthful or unaware of this, and hence, speak with more volume.
Physical Therapy
I never witnessed a session, but the PT kept saying my mother did well. However, in the 11 days she was at Powerback Rehab in Lakewood, her ambulation never improved much, though she learned how to manage a three-step railed staircase.
Powerback Rehab’s grounds, lobby and lounges are very attractive and clean.
But attractive furnishings, lovely decorations and pictures on the walls, and well-landscaped premises are not what restores mobility to a hip replacement patient.
The food at Powerback Rehab in Lakewood, CO is good. But I’d be much more concerned about the aforementioned issues.
My mother’s home PT said that places like Powerback Rehab set the patient back: A week at rehab means two weeks to catch up. The home PT, after assessing her, said that her mobility should have been much further along.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

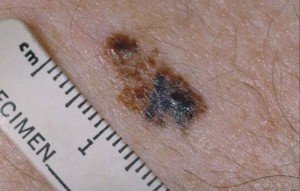
NEVER Pick Off a Melanoma, Says Dermatologist

Don’t even THINK about picking or scraping off that ugly or odd-looking mole that might be melanoma.
“You should not try to rub off a growth that you suspect could be a
melanoma,” says Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
A melanoma will not easily come off. You will need to deliberately and fervently pick or scrape at it to remove some of the cancerous tissue.
A melanoma cannot accidentally come off while routinely shaving over it, routinely rubbing a sponge or rag over it while bathing, while inadvertently rubbing the area against something such as a seatbelt or tight doorway, etc. The removal would have to be on purpose.
And this is possible with “aggressive picking or scrubbing with a device such as a Clarisonic to get to raw tissue,” says Dr. Prystowsky.
“After healing you may not see the growth return. However, in the case of melanoma, cancerous cells may be in follicles and even be non-pigmented, giving the illusion that you successfully rubbed off a suspicious growth.”
Usually, a cancerous mole is as deep below the skin as it is high above the skin.
So removing the surface of it, flush with the skin, will still leave the under-part of it.
And don’t even think of solving this issue by scooping out an area around it.
You STILL might not get all the cancer cells — because there could be microscopic branches of the melanoma extending deep into an area that your scooping missed.
Cancer cell. Shutterstock/Lightspring
And don’t trust your eyes; just because you can no longer see the black or dark pigment, doesn’t mean you cleaned it all out.
“The residual cells may multiply and grow more deeply into the skin and even spread throughout the body and be deadly,” says Dr. Prystowsky.
“Any growth that raises suspicion of melanoma needs to be biopsied to determine if it is melanoma.
“Any treatment decided upon will depend on what the cells look like under a microscope and how deep they are in the tissue.”
When a dermatologist inspects a suspicious mole or new spot, make sure he or she uses a dermatoscope.

In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Air Images

How Much Caffeinated Coffee Is Safe a Day?

What does a doctor have to say about how much caffeinated coffee is safe on a daily basis?
“According to multiple studies, for people in generally good health, up to about 200 mg of caffeine a day is acceptable for most people,” says Marc I. Leavey, MD, a primary care physician with 40-plus years of experience.
Dr. Leavey continues, “With a standard six ounce cup of brewed coffee containing about 100 mg, this would be about two coffee cups daily.
“Remember that coffee cups are six ounces, not eight, so that 12 ounce mug holds two cups.”
Caffeine isn’t the only ingredient in coffee to be aware about.
“Along with the caffeine, there are other substances in coffee which are physiologically active,” says Dr. Leavey.
“Indeed, coffee made with a French Press may have substances which influence serum lipids; filtered coffee removes those substances in the brewing.
“Instant coffee is also lacking those chemicals, and likely is lower in caffeine (for regular instant) than brewed coffee.
“Some studies have suggested there may be toxins in instant coffee, but these are likely at very low levels, ft at all, and may or may not be of clinical significance in typical coffee drinkers.”
Dr. Leavey was formerly with Mercy Medical Center in Baltimore, MD, where his focus was primary care and internal medicine. He has a blog, STRING OF MEDICAL PEARLS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/NOBUHIRO ASADA

Can You RUB Off a Melanoma?

This article is about rubbing off a melanoma, not scraping, picking or cutting.
Ever wonder if melanoma can be literally rubbed off? For instance, with a fingertip, rag or piece of clothing?
“It is not possible to remove a melanoma completely by simply rubbing it with clothing, a rag or a finger,” says Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
But this doesn’t mean you can’t remove some of the melanoma with a rubbing action, especially if it’s big and has raised portions.
It just depends on how hard you rub, the length of time spent doing this (vs. just one swipe with a fingertip or wash cloth) and what the rubbing instrument is (finger vs. sandpaper).
Dr. Prystowsky says that it’s “possible with effort to purposely rub the visible signs of a melanoma off of the skin.
“It would require rubbing that leads to superficial bleeding, however, like a skinned knee from rubbing the rough cement on a sidewalk.”
In short, intense rubbing—with something rough rather than smooth, such as a loofah brush or emery board, as opposed to the smooth surface of your palm or a cotton swab. And it would require repeated swipes.
“Even with this extreme rubbing, it would not mean the melanoma is completely gone, however, because microscopic melanoma cells would remain behind in deeper layers of the skin,” says Dr. Prystowsky.

Melanoma
Melanoma

Melanoma. CDC, Carl Washington, MD, Emory Univ. School of Medicine, Mona Saraiya, MD, MPH
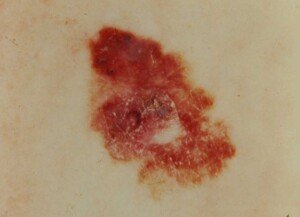
Melanoma. Laurence Meyer, MD/ cancer.gov
There can be micro-metastases, meaning, microscopic branches of the malignant cells extending underneath the visible spot, penetrating into the dermis, which is the second layer of skin.
“Someone rubbing the melanoma would have the mistaken belief that because they cannot see the spot on their skin any longer, that they do not have to worry about it –this is not the case,” explains Dr. Prystowsky.
If you leave even just one tumor cell behind (in theory), that one cell would likely proliferate unseen beneath the visible part of the skin.
“It is worth noting that skin cancer tissue bleeds more readily than normal skin typically, so minor trauma from tight clothing may trigger enough rubbing to disrupt the surface of a skin cancer and cause bleeding.
“This is because cancer cells more readily break away from each other and have a more generous blood supply than normal skin.
“After the bleeding stops, you would expect to see at least some of the skin cancer, e.g., melanoma, remaining under this less traumatic, accidental rubbing situation.”
In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}