

Why You Should Never Ask People Why They Never Remarried

You should never ask someone why he or she never remarried. This is just plain thoughtless and inconsiderate.
It’s dumbfounding how often people, who’ve lost a spouse to death, are asked this question.
However, it’s still a dopey question when it’s asked to a divorced woman or man as well.
Either way, it’s an offensive question, even though there will always be that predictable percentage who will actually delight in explaining why — especially if they lost a spouse to divorce rather than death.
“This question feels very personal for most,” begins Talia Wagner, marriage and family therapist and author of “Married Roommates.”
“When some people are asked this, it comes off as judgmental and critical.
They feel judged for the lifestyle they have in the moment, and the question is taken as their failure to meet the social norms or the expectation of others.
“Some people have a negative viewpoint of marriage and know that they never want a redo of that time.
“However, they also may not want to be judged for having a negative interpretation of marriage, so they give a surface- or façade-like answer, or get upset for even being asked about it.
“This is frequently a defensive response to their own interpretations and insecurities.”
Is it supposed to be easy to find another soulmate?
When people ask, “Why haven’t you remarried?” or something similar, such as “How come you never got remarried?” it’s asked as though remarrying is as easy as buying a new pair of shoes.
A considerate person with common sense will avoid asking this question.
If you know the divorced or widowed individual very very well, you’ll very likely already know why they never remarried.
If you don’t know why and are wondering — DO NOT ASK. Instead, try to figure it out on your own — which shouldn’t be hard to do.
There are several logical explanations for why a widow or widower never remarried:
- They just never crossed paths with Soulmate #2.
- They can’t conceive being with someone other than their deceased beloved, whom they believe was the only one meant for them.
- They are too despondent to date again.
Wagner adds, “For these people, getting remarried feels like a betrayal of their beloved lost one, and swearing off marriage just feels like the right thing to do to not taint their memory.”
As for the divorced person:
- See the first bullet point above.
- By the time the divorce rolled around, the children were still young and naturally demanding, and the parent has decided to involve themselves as much as possible with their kids instead of getting involved with a new person.
For some divorced men and women, Wagner explains, “Marriage was hard for them, and the thought of going through anything similar ever again becomes so distasteful that their overall view of marriage gets colored by it.”
Next time you’re tempted to ask someone why they never remarried, consider the possibility that they’ve been on many bad dates and have had several worthless relationships — and are now bitter and frustrated — and have decided to throw in the towel.
 Talia Wagner, along with her husband Allen, has a private practice in California.
Talia Wagner, along with her husband Allen, has a private practice in California.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, katemangostar
DVT Risk after Joint Replacement Surgery Stays for Years

The length of time that DVT risk remains significant after joint replacement surgery will shock you.
It’s years. Yes, the risk of this dangerous blood clot goes on for years after the joint replacement.
This is the result of a study, led by Yuqing Zhang, D.Sc., Professor of Medicine and Epidemiology at Boston University School of Medicine, that was published in Arthritis & Rheumatology.
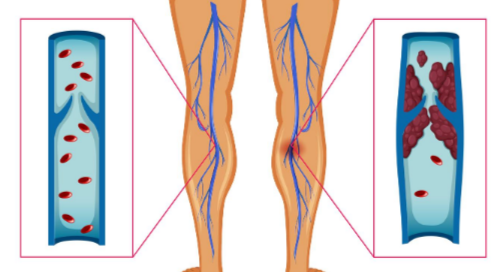
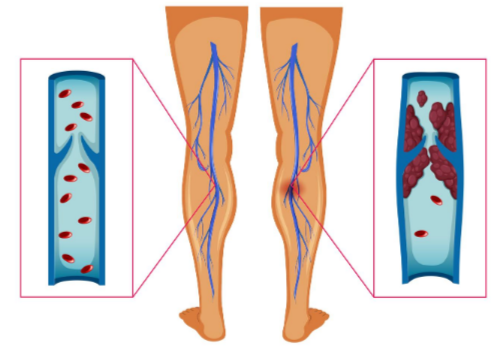
Risk of DVT is high in the first month following joint replacement surgery (knee or hip), but this risk persists for a long time out—years, say the researchers.
“The long-term risk of heart attack was insignificant,” says Dr. Zhang in the 2015 paper, “but risk of blood clots in the lung remained for years after surgery to replace a hip or knee damaged by osteoarthritis.”
A blood clot in the lung is called a pulmonary embolism, and this originates from a DVT (deep vein thrombosis) in the leg when a portion of it breaks off and travels to the lung.
The results of Zhang’s study means that long after your surgeon has taken you off the blood thinners to prevent a DVT, you must still be alert to symptoms that could mean this kind of blood clot.
Why aren’t joint replacement patients on blood thinners for much longer if DVT risk persists for years?
“Anticoagulants raise the risk of bleeding, especially in the head and brain,” says Dr. Paramjit “Romi” Chopra, MD, founder of the Midwest Institute for Minimally Invasive Therapies (MIMIT), an interventional radiology and endovascular therapy practice.
“Therefore, they are not prescribed indefinitely after joint replacement surgery — with the assumption that these patients will resume their normal activity within a few weeks to months,” continues Dr. Chopra.
“Staying active, well-hydrated and maintaining an optimal weight will reduce the overall risk of DVT.”
Symptoms of a DVT are any of the following:
- Redness in the lower or upper leg
- Swelling in the lower or upper leg
- Tenderness or warmth to the reddened area
- A pain or cramp in the calf, leg or pelvic area that does not go away when you sit and rest the leg
However, half of DVTs do not produce symptoms. If some of it or all of it travels to the lung, this can produce one or more of the following symptoms:
- Difficulty breathing
- Chest pain
- Fainting or a faint feeling
Though the risk of a DVT, according to the study, stays for years after the joint replacement surgery, you now know why your surgeon will not want you on a prescription blood thinner for those years.
Dr. Chopra combines his Eastern roots and 30+ years’ Western experience to unify the best of both worlds at MIMIT to treat venous disease, peripheral artery disease and musculoskeletal disease.
combines his Eastern roots and 30+ years’ Western experience to unify the best of both worlds at MIMIT to treat venous disease, peripheral artery disease and musculoskeletal disease.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus/CreativeCommons
Source: sciencedaily.com/releases/2015/08/150831001112.htm

Younger Daughter Bigger than Older Son: Solutions

Do you have a younger daughter who’s bigger than and bullies an older son?
Don’t blame the size difference before you look in the mirror as the cause.
There’s a thread on a health site explaining that the girl is nine years…but 5-5 and 120 and shows signs of puberty. The son is 13, five feet and 90 pounds.
The post describes the son as depressed, and that he and his sister occasionally get into fights and that she is stronger “and can hurt my older son.”
The second case from answers.yahoo.com involves a 16 year old boy, 5-5, and his 14 year old sister, six feet.
The parent writes that the girl regularly inflicts physical harm to him.
I used to be a certified personal trainer for a large gym. My knowledge of physical fitness, muscles, force exertion, etc., tells me that the nine year old girl — as a general rule now — cannot possibly be stronger than a 13 year old boy.
Never mind the height difference; his body is 13 and her body is only nine.
Long bones and long muscles don’t translate to more absolute strength. Let’s call her “Sally” and him “Jack.”
Unless Sally has a bizarre medical condition that has caused her to acquire teenage musculoskeletal development at age nine, I very strongly doubt that she could bench press more weight or throw a harder punch than a same-age girl of “normal” height.

Shutterstock/F8 studio
Though Sally would find it easier than her female classmates to, say, place a 15 pound box on a six-foot-high shelf, this is only because of her positioning — her start position has her vertically closer to the shelf.
But this isn’t a display of absolute strength. An example of absolute strength, rather than mechanically-advantaged strength, is that of pressing a force away from your body.
Though a longer arm should have more torque than a shorter arm, and thus in theory should be able to land a harder punch, I have not seen evidence of this in all the years I’ve studied martial arts.
Due to his age, Jack has more developed muscles, bones and neuromuscular connections.
This would make him stronger in the absolute sense. But psychologically, Sally has him pummeled.
I’ve worked with short strong clients and tall “weaklings.” For instance, I’ve had tall clients struggle with pushups.
So then, what’s going on when the smaller son gets beaten up by his younger, bigger sister?

Shutterstock/aekkorn
The shock value that Little Sis is so much taller may create the illusion that she’s stronger.
This may intimidate the older brother who already has a pre-existing low self-esteem stemming from unhealthy family dynamics.
One day Sally gets mad at Jack and shoves him. Her towering height scares him; he concludes she’s stronger; she comes to believe this based on his fear; she continues pushing him around because she thinks she’s stronger.
(I wonder which of these kids Mom tells to take out the heavy garbage — I’m betting the son.)
I’m betting Jack would find it easier to bench press an empty Olympic bar (45 pounds) than would Sally.
But there’s a big power imbalance going on that’s based on psychology, not muscle fibers.
Haven’t you yourself ever witnessed, when growing up, situations in which the bully was smaller than the victim? I certainly have.
Even in the adult world, the “bully” is sometimes smaller than the victim.
It’s akin to the feisty cat scaring off the much bigger dog.
In the second example, the six-foot-girl might be stronger than her slightly older, shorter brother because she’s already 14.
Maybe she’s a jock; maybe the brother, only two years older, is a bookworm.
A child or teenager will not automatically become a bully to an older sibling just because the older sibling is a lot shorter!
If being bigger than the older sibling is indeed all it takes to turn a child into a bully…then nearly every teen or child with a smaller but older sibling would be a bully.
Size differences do not create bullies! Size is only a tool that the bully realizes she has!
SOLUTIONS
– Get to the root of the sibling bullying instead of blaming it on the superficial feature of size difference.
Could it be your own behavior that’s setting a poor example? Bullies don’t always spring from a physically abusive parent.
For example, “What is more likely, is that children who bully have witnessed their parents use bullying tactics on others,” explains Rona Novick, PhD, developer of the BRAVE bully prevention program and a clinical psychologist.
“They may see Mom or Dad abuse their power to get their way with waiters, dry cleaners, teachers, neighbors or other family members.”
– Reassess your typical response to the fighting between your younger, bigger daughter and older, smaller son. It’s obviously not working.
“Scolding is not the best remedy; humiliating a child only escalates the behavior,” says Janet Lehman, MSW, co-creator of The Total Transformation Program, a program for empowering parents.
“The best approach is to clearly identify the behavior: Label it, communicate that it is unacceptable and attach a clear consequence for the rule breaking,” says Lehman.
– Enroll both kids in martial arts. The bully will mellow out and learn self-discipline, and the victim will learn self-confidence and have tools to stop a fight with minimal physical force.
– Telling Sally to be nice to Jack because she’s probably stopped growing, but he hasn’t yet reached his growth spurt and will be bigger and stronger than her in a few years, won’t correct the underlying problem.
 Dr. Novick is recognized for her expertise in behavior management and child behavior therapy. She has published scholarly articles on school applications of behavior management, children and trauma, and bully prevention in schools.
Dr. Novick is recognized for her expertise in behavior management and child behavior therapy. She has published scholarly articles on school applications of behavior management, children and trauma, and bully prevention in schools.
 Janet Lehman, with her husband James, developed the foundational parenting programs offered by EmpoweringParents.com.
Janet Lehman, with her husband James, developed the foundational parenting programs offered by EmpoweringParents.com.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Black Rock Digital
Sources: healthboards.com/boards/childrens-health/309697-8yr-old-boy-blood-urine.html and: answers.yahoo.com/question/index?qid=20110515065052AAfl9I2

Pushups Using a Dangling Kettlebell: Instructions

Get ready for the kettlebell heavy pushup — for those who dare, for those who find pumping out lots of plain ‘ol pushups is just way too easy.
Pushups need not be fancy to be tough and intense.
For people who are no longer challenged by the conventional pushup, and who don’t want to hassle around with the placement of weight plates on their back, or fussing around with tension bands to add resistance, the kettlebell heavy pushup is just for you.
Equipment needed: kettlebell (ideally two or three of different weights), dip belt and two high exercise stools.
Getting Started
It would be wise to do a set of non-weighted pushups using the stools, to get used to how it feels to perform this exercise in this fashion.
The stools are placed apart so that one’s hands are on the top of one stool, and the tips of their feet are on the second stool: a standard pushup position.
From here, simply do a warm-up set. If you find that your middle is sagging towards the space between the two stools, figure out why this is happening.
It may very well be bad form. During a pushup, the body is supposed to be straight as a board, like a plank of wood. Imagine a group of military personnel doing pushups.
On the other hand, if a trainee cannot keep their body straight, they are not strong enough to perform pushups with solid form.
Bad form (either due to unawareness or weakness) should not be tolerated in the pushup any more than it’s tolerated in the squat.
Though bad form in a pushup isn’t as risky as bad squat form, it will still interfere with achieving desired results.
How much added weight do you think you need to be challenged by a set of pushups?
Select that weight of a kettlebell. However, select two more weights; one lighter and one heavier, just in case your judgment is a little off, or in the event that you want to do drop sets.
Working Sets
Slip into a dip belt and attach a kettlebell, then position yourself on the stools in a pushup start position.
The arms are extended, feet on toes, body straight, kettlebell hanging below midsection.
Now lower into a pushup. The stools should be high enough so that when you lower, the kettlebell does not touch the floor. Push back up. A variation is to place the hands over the sides of the stool.
What makes this kind of weighted pushup superior to bands or a plate placed on the back, is that the added resistance is disconnected from the body.
In tension band pushups, the bands surround the body and are integrated with the trainee. Of course, a plate on the back is on the body.
The kettlebell hangs and even swings a bit. Even the tiniest swinging adds to the workout.
Plus, because it’s disconnected from the body, it produces a unique element to the so-called resistance arm.
In a regular pushup, as well as tension band style, the resistance arm is not extended.
The resistance arm is the athlete’s body itself. When one adds a plate to the back, the resistance arm is extended only by the width of the plate, which is negligible.
In the case of a suspended kettlebell, the resistance arm is extended for whatever the length is from the attachment point of the dip belt to the bottom of the kettlebell; that’s a lot of extra vertical resistance.
Is there a way to increase intensity without increasing kettlebell weight? Yes, depending on available equipment.
If the feet are elevated higher than the hands, this will make the pressing harder.
Give this a try if you can find two elevated surfaces of different heights, but that will get you high enough to prevent the kettlebell from touching the floor.
Why not just do elevated regular pushups for increased resistance?
Why bother hooking up a kettlebell? The more that the feet are elevated, the more that the muscle recruitment shifts from chest to shoulders.
This is why an elevated pushup is harder than a flat one; the shoulders are forced to take more work, and shoulders aren’t as strong as the pectoralis muscles of the chest.
The most elevated form of a pushup is the handstand press; this is all shoulders and very difficult.
It should be clear now why simply elevating the feet higher and higher isn’t a practical solution for those wanting to create a heavier pushup.
The kettlebell heavy pushup keeps the chest as much involved as in a regular pushup, without the trainee having to hassle with the balancing moves of placing each hand on a medicine ball for “extra intensity” or doing other funky things like using only the fingertips or clapping in between.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Plantar Fasciitis Prevention: New Habit for Stronger Feet

There is a unique but very simple way to help prevent the heel pain of plantar fasciitis, and it’s so cheap you won’t believe it.
Just kick off your shoes. And socks. This is what Patrick McKeon recommends. He’s a professor at Ithaca College’s School of Health Sciences and Human Performance.
This doesn’t mean throw out the arch supports. Keep using those, but in addition, go barefoot.
Think of the muscles in the feet as having the same kind of job as the muscles in your “core” (abdomen and lower back).
MeKeon says that there is a feedback cycle between larger muscles of the foot and leg and smaller muscles of the foot.
These two muscle groups send information to the brain. Shoes interfere with this signaling, a “missing link,” he says.
The result is that the larger muscles over-compensate and eventually become too overused to keep up with repairing themselves, leading to overuse injuries including plantar fasciitis.
To help prevent plantar fasciitis, which typically causes a burning type of heel pain, McKeon suggests Pilates, martial arts and yoga—and performed barefoot.

Freepik.com yanalya
Use Common Sense
You don’t want to be playing basketball, volleyball or running on a treadmill barefoot.
“Going barefoot can be beneficial for some, if performed properly (on safe surfaces, done gradually so as to build up mileage over time, and proper stretching is performed before and after activity),” says Bruce Pinker, DPM, who specializes in sports medicine and surgery of the foot and ankle.
“It may help strengthen feet and prevent plantar fasciitis,” says Dr. Pinker.
“Barefoot walking and running is a great activity that can strengthen feet, but should always be performed with caution so as to avoid injury.”
Just make sure you don’t stub your toes and that there’s no broken glass or other sharp objects on the floor.
 Dr. Pinker is with Progressive Foot Care, which provides state-of-the-art, full diagnostic testing and treatment of the foot. He’s a professional foot and ankle health and wellness speaker who delivers many original seminars annually such as “Keep On Running.”
Dr. Pinker is with Progressive Foot Care, which provides state-of-the-art, full diagnostic testing and treatment of the foot. He’s a professional foot and ankle health and wellness speaker who delivers many original seminars annually such as “Keep On Running.”
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/Vladimir Gjorgiev
Sources:
ithaca.edu/faculty/pmckeon
sciencedaily.com/releases/2015/11/151117181929.htm

Sudden Tiny Brown Spot Under Lip Likely Clogged Pore

Have you noticed the seemingly sudden appearance of a very tiny brown dot under (not on) your lip? And you wipe and rub it, and it remains? And it just doesn’t go away?
One day I noticed a very, very small brown dot under my lip.
I aggressively rubbed it with the tip of a finger and it didn’t budge, so I quickly ruled out a speck of grime.
I had an appointment already scheduled with a dermatologist for a routine skin exam, so I knew that soon, I’d be getting a dermatologist’s assessment.
I’ll admit, I was worried, because I just couldn’t figure out what benign thing this very tiny spot could be.
It certainly did not resemble any of the solar “age spots” on my face; those were lighter brown and less dense.
It also didn’t resemble the beginnings of the benign seborrheic keratosis (those need to begin from something, right?). This tiny little spot under my lip, as teeny as it was, looked dense.
If you’ve noticed something like this, stand under very good lighting and stretch your lips into a “smile,” and look closely at the stretched skin around the little brown dot.
What I eventually noticed was that this spot’s location fell neatly into the location of neighboring pores.
During previous inspections, I had not noticed the surrounding pores because I had not stretched my lips out and angled my face in such a way that the light illuminated them.
But this time I did, and voila, lots of visible pores, like a field of them, and this tiny brown speck was neatly part of the field. A clogged pore, I wondered.
I also had noticed that it strongly resembled a few of the clogged pores on my nose. I held out hope that this was what the dermatologist would tell me.
And she did. She took no time, after viewing it, to tell me that it was a clogged pore.
So if you notice something like this near your lip, you now have a benign explanation of what it could be.
However…I would urge you to get it checked by a dermatologist just to be sure. DO NOT PICK IT WITH A PIN.
It may make you feel relieved to “get rid of it,” but then if you do—you’ll never know what it really was.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Image Point Fr
COLON CANCER: STOOL CHANGES, Symptoms, Detection: Answers

If you’re worried about colon cancer and can’t find answers online, you just might find the answers to your questions in the articles below.
Bowel movements or “stools” form as food is digested and nutrients are absorbed in the small intestine, leaving waste material.
This waste has to be expelled, so it then enters the large intestine. This tract is where colon cancer can occur.
It’s also where water is absorbed, and gut bacteria break down remaining substances, forming stool.
The rectum stores stool until signals from nerves trigger the urge to “go.”
Muscles in the rectum and anus then expel your BMs.
Stool consistency depends on diet, hydration, gut health and transit time through the intestines.
The consistency can also be affected by an obstruction in the colon or rectum. That obstruction could be hardened fecal matter (constipation), a colon polyp, or, colon cancer.
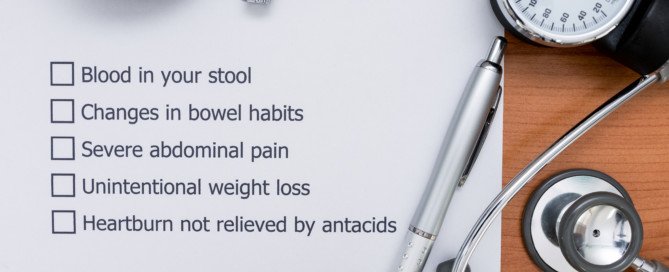
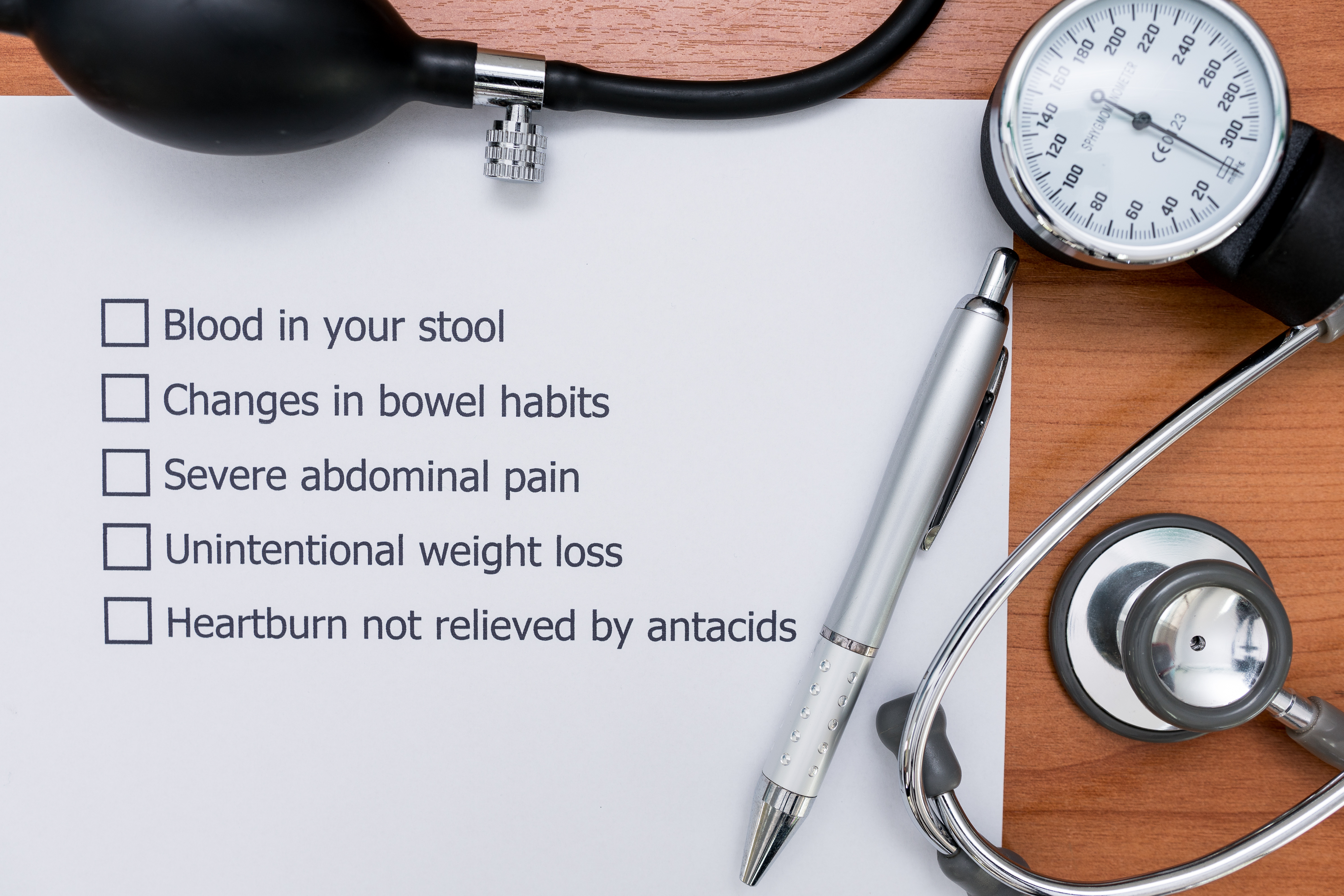
A symptom of colon cancer that nearly health concsious person has heard of is that of narrow, or thin BMs. Sometimes they’re described as like a pencil or ribbon.
But colon cancer isn’t the only cause of elongated thin stools.
Just what goes on inside the body that causes stools to come out in ribbons or like pencils anyways?
The problem doesn’t always exist at rectal level.
Here’s how colon cancer can make BMs narrow and long.
Another symptom that’s relatively well-known is that of “tarry” or black bowel movements.
However, food or medications can also very much darken stools.
But there are differences.
Symptoms of IBS and Colon Cancer Nearly Identical
You should never assume that your new-onset digestive symptoms are “probably just IBS.”
The signs of IBS greatly overlap those of colon cancer.
However, the diagnostic process for each are completely different.
So if you’ve been having the classic signs of irritable bowel syndrome, you still need to get this confirmed by a gastroenterologist to rule out colon cancer; the symptoms are too similar to ignore.
And by the way, if you’re younger than middle age, this doesn’t make you immune to cancer of the colon.
This disease can strike even someone in their 30s.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Image: Shutterstock/Bangkoker

Is a Lot of Bleeding During Menopause Something to Worry About?

If you’re bleeding a lot during menopause — and a doctor has confirmed menopause — then something may be very wrong.
For this post I asked Dr. Gino Tutera, an OB/GYN and a specialist in bioidentical hormone replacement therapy, if heavy bleeding could be normal during menopause.
“No,” begins Dr. Tutera. “But this is the answer if the woman is fully into menopause — as would be evidenced by laboratory testing or having no menses for a full year.”
Obesity can cause menstruation to stop — including for 12 months in a row.
So if you’re of menopausal age and have not had a period in 12 months — BUT are obese (particularly severely obese) — you should have laboratory testing done to confirm the presence or absence of menopause.
If you’re bleeding from your menstrual cycle, then this contradicts going through the menopause, as by definition, the menopause is the end of your menstruation.
So if you’re going through menopause but are also experiencing heavy bleeding — the cause is certainly not your period — and you had better get this checked out promptly by a gynecologist.
If you’re experiencing heavy bleeding during menopause, this is not a normal part of the process.
During the perimenopausal years leading up to menopause, it’s common to experience irregular periods and varying flow, but once you have officially entered menopause, bleeding should cease altogether.
Therefore, any unexpected heavy bleeding after this point is a cause for concern and warrants prompt medical attention.
While it could be related to hormonal fluctuations or changes in the uterine lining during the perimenopausal phase, heavy bleeding could also be a sign of more serious underlying conditions.
Don’t be afraid to get an exam; early detection of a serious problem certainly means a much better outcome.
But are you sure you’re even going through menopause in the first place?
A woman, close to the start of menopause, may go several months without a single period.
Then she starts bleeding heavily—and she assumes that this is another period.
However, if the bleeding doesn’t resemble her typical menstruation, maybe she IS in menopause.
As mentioned, lab testing (a blood test) can show if a woman is in menopause.
“During the transition into full menopause,” says Dr. Tutera, “it is very common to have significant variations in the timing of periods and amount of bleeding. The ovaries are just not functioning consistently day to day.”
What could bleeding heavily during menopause be caused by?
Causes include: benign uterine or cervical polyps, endometrial thickening or thinning, cancer of the uterus, vagina or cervix, or a cervical infection.
This list of causes, including the cancers, is not complete.
Dr. Tutera initially specialized in obstetrics and gynecology and then moved on to treating hormonal imbalances in women. He passed away in 2015.
initially specialized in obstetrics and gynecology and then moved on to treating hormonal imbalances in women. He passed away in 2015.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Chinnapong

Can Discharge from Vaginal Atrophy Resemble Cervical Mucus?

Is cervical mucous even present when there’s vaginal atrophy?
Atrophic vaginitis (vaginal atrophy) is the result of menopause, when a woman’s estrogen levels drop so much that her vagina literally dries out or loses its natural lubricant.
According to Mayoclinic.com, one of the possible symptoms of moderate to severe vaginal atrophy is “vaginal discharge.” Does this resemble cervical mucous?
“The answer is absolutely no,” says Dr. Gino Tutera, an OB/GYN and specialist in bioidentical hormone replacement therapy.
Dr. Tutera explains, “Cervical mucous is quite different than the natural moisture from a normally functioning vagina.
“Cervical mucous consistency varies considerably based on the woman’s level of estrogen.
“Vaginal atrophy is caused by lack of estrogen, so there will be very little, if any, cervical mucous.”
Dr. Tutera initially specialized in obstetrics and gynecology and then moved on to treating hormonal imbalances in women. He passed away in 2015.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasha2109
Source: mayoclinic.org/diseases-conditions/vaginal-atrophy/basics/symptoms/con-20025768

How Does Colon Cancer Increase Mucous Production?

Yes, colon cancer can increase the amount of mucous in your stools.
And this is what’s so scary, because this substance in the stools is actually a normal occurrence.
The reason for the normal mucous production that appears in one’s bowel movements is so that the transit of the fecal matter through the digestive tract can be smoother; think of the mucous as lubrication.
So naturally, a little bit of this white goop will sometimes make its way into the toilet bowl with your stools.
However, colon cancer can also result in mucous appearing with your stools.
“Villous tumors can secrete mucous,” says gastroenterologist Sander R. Binderow, MD, FACS, FASCRS, with Atlanta Colon & Rectal Surgery.
“They can be malignant or benign. A large villous tumor can still be benign and make large quantities of mucous.”
Get to know what’s normal for your bowel movements.
If you’ve been taking note of what’s normal—over a long period of time—then something out of the ordinary will be more obvious.
On the other hand, if you’re new to getting to know your poops, and you just happened to notice some white goopy stuff in them the first time you decided to inspect them, this could be unnerving—because you don’t know if that’s normal for you.
It’s also important to point out that the white goop that a woman sees with her BMs isn’t necessarily from her digestive tract; it could be normal discharge from her cervix or vagina that coincided with the bowel movement.
Look closely at the mucous whether you’re a male or female to see if there’s any blood in it.
It may have a tinge of orange-brown—that’s normal, from the fecal matter that contacts it.
Another thing you can do is to take a stool sample test at home with Cologuard.

Cologuard is by prescription only.
It uses advanced DNA technology to detect abnormal cells in your stools, and if this test turns out positive, the next step would be a colonoscopy as a diagnostic test to look for colon cancer.
 Dr. Binderow
Dr. Binderow 

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}