
Can Intense Exercise Prevent Insulin Resistance?

Is it really true that intense exercise can prevent you from ever getting insulin resistance?
IR is when the body’s cells can no longer efficiently “take” the glucose molecules that are delivered to them via the hormone insulin.
Glucose is blood sugar. When insulin receptors on the cells can no longer receive all the sugar for energy, the body is then left with unutilized sugar, resulting in higher-than-normal blood sugar levels, and excess sugar going to the liver where it’s converted to fat.
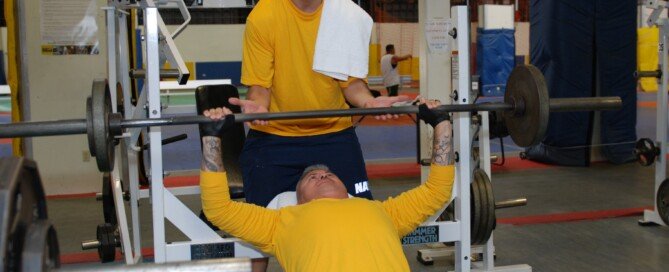
Intuitively, it seems as though regular intense exercise should prevent insulin resistance.
After all, exercise lowers blood sugar and creates more insulin receptors on cells.
We’ve always heard that type 2 diabetes, of which insulin resistance can lead to, can usually be controlled with just diet and exercise.
And we’ve heard that lack of exercise is strongly — very strongly — implicated in the development of insulin resistance.
“Insulin resistance is a genetic trait … you either have it or you don’t,” says Dr. David Edelson, MD, board certified in internal and bariatric medicine, one of the top obesity experts in the U.S., and founder and medical director for thin-site.com and HealthBridge.
However, much like a pendulum, it must be pushed to be set into motion. The ‘push’ could be bad diet, lack of exercise, poor sleep, aging, medications or some other external environmental force.”
Think of it this way: Genetics load the gun, but lifestyle habits pull the trigger.
Dr. Edelson continues: “Conversely, exercise acts like a ballast providing extra weight to a pendulum, making it require more force to set into motion.
“So while in a strict sense exercise will not prevent insulin resistance, it will make it much harder to turn on the gene and set the wheels in motion.”
This is why exercise is one of the major forces that physicians urge their IR patients to undertake to reverse the condition. Inactivity is a leading cause of IR, which affects about one out of every five American adults.
Dr. Edelson explains, “Exercise has definitely been proven in several clinical studies to reduce insulin resistance.
“First of all, it burns up excess circulating blood sugar, preventing the pancreas from having to secrete too much insulin.
“Persistently high levels of insulin in the bloodstream cause reduction in the amount of insulin receptors, the first stage of manifesting IR.”
“Secondly, regular exercise causes increased production of insulin receptors on the muscle cells.
“More receptors means better response to the effects of insulin, resulting in lowering blood sugar and triglyceride levels, less hunger and prevention of weight gain.”
By the way, you can have a normal fasting blood sugar value and still have IR (too much of the hormone in the bloodstream because the pancreas has to over-secrete it in order to lower blood sugar).
Hardcore, intense exercise, though not capable of outright preventing insulin resistance, is a formidable tyrant at minimizing your odds of ever developing IR, not to mention so many other medical conditions.

Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Sources
“Exercise-Induced Transcription of the Muscle Glucose Transporter (BLUT4) Gene”; Biochemical and Biophysical Research Communications, Volume 292, Issue 2, 29 March 2002, Pages 409-414
“Acarbose with Exercise Improves Metabolic Control and Cardiovascular Risk Factor”; Diabetes Care 2006 29:1471-1477
www.thin-site.com; www.healthbridgeinfo.com

Can Insomnia, Poor Sleep, Cause Insulin Resistance?

Who’d ever think that poor sleep or insomnia can actually cause insulin resistance? But it can.
Insulin resistance is associated with obesity, even being moderately overweight, lack of exercise and poor diet. It can lead to type 2 diabetes.
But a person who works out like a warrior, has a strict diet, and is a lean, mean athletic machine, can still end up with insulin resistance if he or she gets poor quality sleep.
“There is a strong association between sleep disorders and both obesity and insulin resistance,” says Dr. David Edelson, MD, board certified in internal and bariatric medicine, one of the top obesity experts in the U.S., and founder and medical director for thin-site.com and HealthBridge.
“When I refer to sleep disorders, I am speaking of anything that can cause either a lack of sufficient quantity of sleep (insomnia, lifestyle issues) or poor quality (sleep apnea, restless legs, fragmented REM sleep, etc.).”
Lifestyle issues include anxiety levels that keep a person tossing and turning, unable to slumber for more than several hours at a time.
Dr. Edelson continues, “The basic problem is that the body requires a certain amount of deep cycle sleep to restore its normal functions after a full day of activity.”
There are two phases of restorative sleep: REM (the dream stage) and slow wave.
“During these phases the body undergoes repair and rejuvenation, restoring depleted hormones and repairing damaged tissues,” says Dr. Edelson.

“If someone has poor sleep quality or quantity, these processes will not occur to a sufficient degree.
“Over time this can result in a multitude of medical issues, including obesity, insulin resistance, hypertension, heart failure, arrhythmias, immune disorders, and the list goes on.”
Insulin resistance can even be caused by just one night of poor sleep, according to a study that was reported in the Journal of Endocrinology & Metabolism (2010).
“Our findings show a short night of sleep has more profound effects on metabolic regulation than previously appreciated,” says Esther Donga, MD, of the Leiden University Medical Center in The Netherlands, and the study’s lead author, in the report.
“Our data indicate that insulin sensitivity is not fixed in healthy subjects, but depends on the duration of sleep in the preceding night.”
Millions of people have obstructive sleep apnea (OSA) and don’t even know it.
Though obesity is associated with this life-threatening condition, not all patients are overweight, and it can affect children, though not commonly.
If you’ve been diagnosed with OSA, you may have insulin resistance.
“As the patient falls into the deep stages of sleep, the muscles around the airway relax and the breathing becomes obstructed,” says Dr. Edelson.
“Oxygen levels fall as the patient literally is choking, and in most cases he/she snaps out of the deep stage sleep into a lighter stage.
“This can happen over 100 times an hour in severe cases, with oxygen levels falling to 60 percent of normal.”
As frightening as this sounds, and as life-threatening as it is (dramatically increasing risk of heart attack and stroke), you can have this disorder and be completely unaware, especially if there’s nobody with you overnight to hear your snoring — a classic symptom of the condition. An overnight oxygen level test will confirm diagnosis.
A questionnaire on thin-site.com, called the Epworth Scale, can evaluate your risk of having OSA.
If you turn out to be diagnosed with OSA, insist on being screened for insulin resistance.
Dr. Edelson says, “Restoring good quality sleep is often one of the most powerful things that can be done to improve a patient’s overall health,” including lowering the risk of insulin resistance, or reversing it if you already have it.
If You Can Retire, Do So! You’ll Sleep Much Better.
Retirement leads to better sleep and improves insomnia, while continuing to work doesn’t.
There’s fewer sleep disturbances and insomnia once a person retires, but this improved sleep isn’t so much from the benefits of retirement, as it is from the removal of the stress of having a job—so says a study that’s reported in the journal Sleep (2009).
The researchers (lead by Jussi Vahtera) found that the chances of having poor sleep during the seven years following retirement were 26 percent lower than in the seven years before leaving the workforce for good.
This post-retirement improvement was greatest in the study participants who were in management jobs, people who had reported jobs with high psychological demands, and those who worked nights.
So remember that if your concerned about poor sleep leading to insulin resistance.
Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
www.thin-site.com
www.healthbridgeinfo.com

Can Insulin Resistance Kill You?

Wondering if insulin resistance can kill a person?
Can you actually die, directly, from insulin resistance?
This is a fair question, because insulin resistance is a precursor to type 2 diabetes, and type 2 diabetes is a leading killer of people in the U.S.
Insulin resistance raises the risk of stroke, heart disease, kidney disease and other potentially lethal conditions.
Nevertheless, can insulin resistance, of which 60 million Americans have (many not even knowing it), outright kill a person?
“Nobody will ever die as a direct result of having insulin resistance,” says Dr. David Edelson, MD, board certified in internal and bariatric medicine, one of the top obesity experts in the U.S., and founder and medical director for thin-site.com and HealthBridge.
“However, think of it like a stick of dynamite with a very long fuse,” he continues.
“Treat it properly with good lifestyle habits and the fuse will never be lit. Adopt poor lifestyles like a diet high in starches, sugars and bad fats, lack of exercise and poor sleep patterns, and you light the fuse.”
Let’s talk about good lifestyle habits. Often, people think they have healthy lifestyle habits, when in fact, they don’t.
I’m a former certified personal trainer and have known many people who believe they get adequate exercise, when in actuality, just the opposite is true.
Vacuuming and hoisting out the garbage on Sunday evening shouldn’t count as your exercise for Sunday, especially since these tasks involve non-neutral spinal alignment — a bad thing.
You still owe yourself at least 20 minutes of vigorous exercise — in a systematic, methodical way, such as a combination of jumping rope, stair stepping (even one step will suffice if all you have is one step in the house), lunges, squats and jogging in place with high knees.
Bad fats are found in commercially-prepared pastries as well as many snack or munchies-type foods. Read the ingredients lists, even if the box says “no trans fats.”
If you spot the word “hydrogenated” in the ingredients list, don’t buy the item; this is a bad fat.
And limit sugar (and high fructose corn syrup) consumption. Sugar is so ubiquitous that it’s found even in tomato soup.
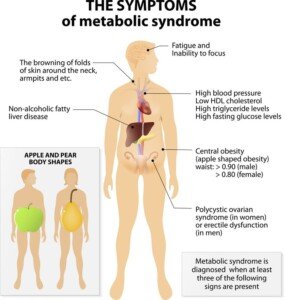
Dr. Edelson continues, “Along this fuse, you pass certain critical points: One is the metabolic syndrome, another obesity, as well as high blood pressure, and finally type II diabetes.
“Each of these points makes the fuse burn faster toward the eventual explosion of heart attack, stroke, kidney failure, etc.”
Shutterstock/Disignua
So the answer to “Can you die from insulin resistance” is actually no, in terms of a direct way, such as dying from a gunshot wound.
But in an indirect way, you definitely can, indeed, die from insulin resistance — though it may take years for that spark along the fuse to travel from the point of insulin resistance to the point of death from stroke (from uncontrolled type 2 diabetes).
Insulin resistance is a warning that you are on the path to type 2 diabetes, a top 10 killer of U.S. people.
Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sukiyaki
How a Low Thyroid Can Make You LOSE Weight

It’s possible that low thyroid can cause weight loss — but wait till you find out how this can happen.
Hypothyroidism (the medical term for “low thyroid”) is often blamed on gaining weight.
Hypothyroidism is associated with weight gain and being overweight.
How many times have you read or heard about overweight people blaming low thyroid on their inability to lose weight?
Hypothyroidism is even blamed on obesity! It’s a fact that hypothyroidism can cause some weight gain.
However, low thyroid can cause weight loss, too. I know this because my mother has hypothyroidism and it has caused her to lose weight.
But how can this be? What few people realize (and many doctors overlook this as well, including my mothers’ doctors) is that hypothyroidism is a major cause of clinical depression.
A savvy doctor, upon being presented with a clinically depressed patient, will order a blood test to screen for low thyroid before hastily prescribing the antidepressants.
My mother’s low thyroid caused her to sink into a profoundly depressed state. This went on for about two months before she finally got a blood test that revealed hypothyroidism.
Sequence of events: Mother starts losing appetite; nobody thinks anything of this. She becomes increasingly edgy; nobody thinks anything of this.
She undergoes knee surgery, and immediately afterwards slips into a deep, dark hole of depression, with absolutely no interest in eating.
She quickly loses 10 pounds (from 145) and must be begged and pleaded with just to eat 600 calories a day.
Six weeks after surgery finally goes on Cymbalta (my father was the obstacle to this; I’d been insisting on an antidepressant since several days post-op, but he wouldn’t hear of it and was in denial, and my mother as well detested the idea of antidepressants; but finally my father agreed).
Cymbalta works like a charm: My mother’s interest in eating resumes the day after her first dose!
However, over the next several weeks she develops other symptoms: constipation and excessive sleepiness.
We take her to ER. The ER doctor notices what appears to be hair loss on her scalp and orders a thyroid test!
Bingo! The test comes back positive for hypothyroidism, which explains all of her symptoms (including cold intolerance and an occasional hoarse voice).
Major depression suppresses appetite. If major depression is secondary to hypothyroidism, then technically, the hypothyroidism will cause weight loss.
But not all people with low thyroid will experience depression.
Low thyroid can cause a myriad of symptoms, but the ones that get the most publicity are the weight gain, fatigue (which my mother also had), hair loss and feeling cold in a warm room.
My mother will be taking medication for low thyroid for the rest of her life, and interestingly, she now weighs 131.
She had eventually gotten back up to 143 (she’s about 5-4), and never “gained weight,” but about 10 months after the hyperthyroidism diagnosis, she had emergent quintuple bypass surgery.
This tripped up her thyroid level (resurrecting the depression), and hence, her medication had to be increased!
It took several weeks for the increase to start taking effect (and she eventually got her appetite back).
Interestingly, the depression had disappeared, but eating like a bird, and holding onto the weight loss, persisted for a while.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Should People with Celiac Gene Avoid Gluten If Not Sick?

Should people with the celiac disease gene avoid gluten even if they have no symptoms of gluten intolerance?
About 30 percent of the American population has the gene associated with celiac disease.
According to the National Institutes of Health, three million Americans actually have celiac disease.
Possessing the gene for celiac disease doesn’t mean you’ll necessarily develop this autoimmune condition.
In fact, only 1 to 2 percent of the population will develop CD, says Pam Cureton, RD, LDN, Center for Celiac Research, Growth and Nutrition Clinic in Baltimore.
Having the gene for celiac disease means that the person is predisposed to developing the condition, which can affect people in so many different ways; is one of the most misdiagnosed illnesses; and can cause serious complications such as small-intestine damage, brittle bones and other fall-out from micronutrient and macronutrient malabsorption.
So how does a person learn he or she has the gene for celiac disease? It’s not discovered by accident.
The gene has been identified, for sure; it’s just a matter of requesting the genetic test for it.
Sometimes a person will request this test because a family member has been diagnosed with celiac disease.
Another motive for getting the test is if the individual either has a confirmed, or a suspected, sensitivity to a certain type of food.
Out of curiosity, they then request a full-spectrum analysis for food sensitivity, which may include testing for the presence of the celiac disease gene. The test then reveals that they have this gene.
Should this person, then, commit to a gluten-free diet for the remainder of his or her life, simply based on the presence of a gene, even if they have no symptoms whatsoever of celiac disease?
It doesn’t seem logical to avoid gluten like the plague, just to prevent getting an illness that they have only a 1-2 percent chance of developing.
Should such a person even just cut back on gluten? Cureton explains, “The quantity and timing of gluten introduction can contribute to the development of CD if introduced before four months of age.
“At this time, however, we do not recommend that anyone with just the genetic compatibility for celiac disease remove gluten from the diet.”
However, suppose someone not only has the gene associated with celiac disease, but he or she tests positive for an immune reaction to gluten (elevated antibodies), yet still has no symptoms or perceived ailments.
Cureton explains, “If antibodies are positive, a person should have an endoscopy to see if there is intestinal damage. This damage can be there without symptoms.
“If the damage continues, the ‘symptoms’ could be a secondary autoimmune disease that will take on a life of its own, separate from CD, treated or not.
“We have seen many people that did not have symptoms but did have a positive EGD in our clinic.”
People with diagnosed CD are committed to avoiding gluten 100 percent.
This means avoiding any foods that may have come in contact with gluten-containing foods, such as fruit that was sliced on an unwashed cutting board that was previously used for slicing bread – which contains gluten.
They must avoid, for example, a food item that was cut with a knife that has a few crumbs on it from cutting the bread. It’s all or nothing.
Even the most minute ingestion of gluten (which is found in tons of processed foods) can set off symptoms of celiac disease in the diagnosed patient.
Untreated CD (treatment is lifelong total avoidance of gluten) over time damages the small intestines, severely impairing their ability to absorb vital nutrients.
So though the person is eating, he essentially becomes very malnourished and sickly. The illness raises the risk of small-intestine cancer and lymphoma.
A person with CD cannot digest gluten, a protein found in wheat, barley and rye; the body “thinks” that the gluten is a foreign invader and stages an attack against it; over time, this over-reactive immune response damages the body.
Symptoms of celiac disease include: unexplained weight loss, fatigue, diarrhea, bone pain and abdominal bloating.
The takeaway message, then, is that if you’ve learned you have the gene for celiac disease, but are otherwise healthy and symptom free, then you can continue to enjoy foods with gluten.
However, if you begin developing unexplained symptoms that elude your doctor, request being tested for celiac disease (a simple blood test is the first step).
 Pam Cureton uses her expertise to help patients with celiac disease as well as other gluten related conditions navigate the gluten-free diet; she devoted to outreach programs for increasing awareness of celiac disease and other gluten-related conditions.
Pam Cureton uses her expertise to help patients with celiac disease as well as other gluten related conditions navigate the gluten-free diet; she devoted to outreach programs for increasing awareness of celiac disease and other gluten-related conditions.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
,
Top image: Shutterstock/ Mia Stern
Source: celiac.com/articles/1164/1/Celiac-Disease-Statistics/Page1.html

Does Celiac Gene but No Disease Mean You Can’t Eat Gluten?

If you have the celiac gene but not the disease, should you eliminate gluten?
The short answer is: No.
Even if celiac disease only develops in people who have the genes for it, having the genes only, indicates a predisposition, nothing more; in fact, 95% of those who have such genes will never become celiac,” says Stefano Guandalini, MD, Founder and Medical Director, The University of Chicago Celiac Disease Center.
Dr. Guandalini adds, “Thus, having the genes only, does not mean you must eat gluten-free.”
I wondered, then, about a person whose blood test for celiac disease is negative, he’s symptom-free, but a stool sample shows elevated gliadin antibodies. (Gliadin is a component of gluten.) At that point, should he eliminate gluten?
Dr. Guandalini comments, “No. So far, all forms of testing in the stools carry absolutely no weight in screening or, even less so, diagnosing celiac disease or gluten sensitivity.
“Relying on such tests is to be avoided. Treatment (the gluten-free diet) should only be started after the diagnosis has been conclusively reached, typically on the basis of positive antibody blood tests and a consistent biopsy of the small intestine.”
According to the University of Chicago Celiac Disease Center: If you have a gene associated with celiac disease and are having symptoms, you should have the antibody blood tests to screen for the disease immediately.
If you have the gene and are a first-degree relative of a biopsy‐diagnosed celiac, you should be screened every 2‐3 years or immediately if you have symptoms.
If the blood test is negative and you’re not having symptoms, but you have the genetic predisposition for celiac disease, at that stage of the game, you can definitely continue eating gluten.
A definitive diagnosis comes with an intestinal endoscopy, not a stool sample or even the blood test.
Symptoms of celiac disease include digestive issues, fatigue, weight loss, muscle cramps, aching joints, skin rashes, brittle bones and depression, to name just a few of the wide range of symptoms possible.
Most people with active celiac disease, however, do not have symptoms.
 Dr. Guandalini is an internationally recognized expert on celiac disease, Professor Emeritus, University of Chicago, and the founder of the University of Chicago Celiac Disease Center. His clinical and research efforts have greatly influenced how celiac disease is diagnosed and treated today.
Dr. Guandalini is an internationally recognized expert on celiac disease, Professor Emeritus, University of Chicago, and the founder of the University of Chicago Celiac Disease Center. His clinical and research efforts have greatly influenced how celiac disease is diagnosed and treated today.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/iodrakon
:celiacdisease.net/factsheets

Low Thyroid Medication Adjustment: Why the 8 Week Wait?
Why must one wait eight weeks between adjustments for low thyroid medication?
The eight-week wait between thyroid medication adjustments can be hairy if the last adjustment wasn’t sufficient to correct the hormonal imbalance.
Typically, the low thyroid patient will have a blood test to determine how much bioidentical hormone is needed on a daily basis to restore thyroxine levels to normal.
It takes eight weeks for the dose’s optimal effect, or ultimate effect, to manifest itself.
This is why the low thyroid patient must wait eight weeks in between adjustments for the medication.
“This is due to the slow effect of the typical formulations used to treat hypothyroidism, which are T4 only (thyroxine, Synthroid and Levoxyl),” says Dr. Kent Holtorf, MD, thyroidologist and founder of Holtorf Medical Group in California.
He continues, “With the use of T4/T3 combinations and T3, which are quicker acting and more effective, the tests can be done much sooner at 2-3 weeks.”
Unfortunately, not all medical establishments rely upon this more definitive testing and treatment for low thyroid, and as a result, some patients suffer needlessly in between the dose re-evaluations.
So if your TSH level is abnormal, indicating low thyroid, you will be given the medication.
It may seem that it’s not working, however, because several weeks later, you may still be suffering symptoms of low thyroid, or, there may be improvement, but not enough to make life comfortable again.
You may then believe that the dose (either first-time or an adjustment) was not enough, and ask your doctor if you can get an increase in micrograms.
Your doctor will reply that you must wait eight weeks, because medication for low thyroid is “long-acting.”
The T4-only protocol can really be problematic, because hypothyroidism can create considerable issues…symptoms severe enough to debilitate the patient.
These symptoms include deep depression, need for excessive sleep, short-term memory problems, and irrational thinking, and not just the other symptoms that most people think are the only symptoms associated with low thyroid: weight gain, fatigue and feeling cold.
Surgery can render current T4-based treatment insufficient in a patient with a pre-existing diagnosis of low thyroid.
Post-surgery, the patient experiences hypothyroidism symptoms, despite continuing to take the daily-prescribed dose of Synthroid or Levothyroxine.
The dose is increased a week after surgery while the patient recovers in the hospital, but the increase wasn’t enough; the patient is sent home to recuperate.
However, there are problems that don’t seem connected to the surgery. The patient continues to be depressed, lethargic, not sensible, not interested in eating, and “always tired.”
Unfortunately, if on a T4-based treatment, the patient must wait six or seven weeks for another blood test to see where the thyroxine levels are at.
However, it’s possible that over that 6-7 weeks, the symptoms will disappear as the long-acting hormone replacement begins kicking in full force.
So now you know why low thyroid medication adjustments have an eight-week wait in between – unless it’s the more effective T4/T3 or T3 treatment plan.
 Dr. Holtorf has published a number of endocrine reviews on complex topics in peer-reviewed journals on controversial diseases and treatments.
Dr. Holtorf has published a number of endocrine reviews on complex topics in peer-reviewed journals on controversial diseases and treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Should Genetic Testing for Celiac Disease Be Standard?
Ever wonder why, at the annual physical exam, your primary care doctor doesn’t do a genetic screening for celiac disease?
Since celiac disease takes an average of nine years to be diagnosed in a symptomatic person, and it is one of the most misdiagnosed medical conditions, one must wonder why genetic testing for celiac disease is not a standard part of the routine physical.
It’s estimated that one in 133 Americans has celiac. That’s pretty common.
“Genetic testing is best used to rule out celiac disease,” says Stefano Guandalini, MD, Founder and Medical Director, The University of Chicago Celiac Disease Center.
“About 30 percent of the population carry the genes related to celiac disease; only 5% of that group ever develop the disease.
“Genetic testing can be useful in at-risk populations, like first-degree relatives of someone with biopsy-diagnosed celiac disease.
“In those cases, if the relatives have the gene/s they should be screened with an antibody blood test every three years or immediately upon symptoms.
“If they don’t have the gene/s, then they never have to worry about developing the disease and no further testing is needed.”
Not having the gene(s) for celiac disease does not mean that any strange symptoms that you have can’t possibly be caused by an intolerance to gluten.
In fact, a person can have the so-called gluten sensitivity, with or without having the genetic predisposition to Celiac Disease.
“This condition (gluten sensitivity), whose prevalence is unknown, typically causes gastrointestinal symptoms such as those from irritable bowel syndrome,” says Dr. Guandalini.
However, gluten sensitivity does not cause the potential harm to the body, that celiac disease does, such as brittle bones, neurological problems and intestinal cancer.
The only known treatment for CD is to banish all gluten from one’s diet … for life … and this means not even one occasional wheat cracker, not even a crumb.
This is why people with CD, when going gluten-free, won’t even eat food that was prepped on the same cutting board or even counter, that gluten-containing foods were, unless the surface area is thoroughly cleansed.
They can’t even eat fruit from a plastic bag that had a gluten-containing sandwich in it; there’s bound to be a few crumbs in the plastic that will “contaminate” the fruit.
In celiac disease, the body’s immune system will be activated by one tiny crumb. It is this immune response that damages the body, whether the patient experiences symptoms or not.
Though genetic testing for celiac disease is not a standard part of the routine annual physical, nothing should stop you from requesting a blood test for this condition.
However, having the blood test is worthless if you don’t have the gene for CD.
So if you want annual testing for celiac disease, you should first find out if you even have the gene. This can be done via an independent lab.
Dr. Guandalini is an internationally recognized expert on celiac disease, Professor Emeritus, University of Chicago, and the founder of the University of Chicago Celiac Disease Center. His clinical and research efforts have greatly influenced how celiac disease is diagnosed and treated today.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/iodrakon

What to Expect the Day AFTER Knee Replacement Surgery

The day OF total knee replacement surgery — after the surgery, that is — is not always the same as the day AFTER total knee replacement surgery.
Are you worried about a loved-one who just had total knee replacement surgery, who seemed to be doing well and in high spirits several hours after the surgery, but then next day, seemingly has taken a turn for the worse?
Relax. This is normal. I know so because my father just had total knee replacement surgery.
The surgery for his knee replacement was in the late morning, and in the evening, I visited him.
He was in high spirits, feeling no pain (due to a “nerve pain block” that was still in effect), and his knee had what appeared to be several pounds of bandages wrapped around it, above it and below it.
Emotionally, he was doing great; total knee replacement surgery is very traumatic to the lower body, even though advertisements for total knee replacement surgery make the ordeal seem like smooth sailing.
The next day, I saw a completely different man. He complained of burning skin and a burning forehead, yet a chilled lower body; grueling pain in the knee despite having been medicated all day long with painkillers, and was depressed, downtrodden, dismal, and kept complaining that there had been no progress with the rehab.
His startling words were, “I have a gut feeling something is wrong.” He said he felt that the knee just wasn’t working at all during the rehab.
The morning after total knee replacement surgery, a patient is started on rehab.
In the surgery, the knee is literally replaced; the patella bone is removed and a titanium plate is put in, and in between the knee are metal parts that substitute for the cartilage that was originally there.
Despite such extensive surgery, the patient is given rehab the following morning.
He or she is held by rehab staff while trying to walk using a walker. Additionally, rehab involves various exercises.
My father kept saying how poor he had performed, and kept comparing this outcome to the morning and day following his first total knee replacement.
A nurse took his temperature to check for fever; his forehead was hot; he felt burning up; also felt chilled; but wanted the room cooler.
His temperature was normal. My father’s dampened spirits were spooky; I’d never seen him like this before.
This wasn’t just about knee pain.
There was the odd burning sensation in his skin and face; he appeared flushed; there were the chills in the lower body; and overall he just felt terrible, hopeless and was convinced that somewhere along the way, there was a mistake made.
He even entertained the idea that the nerve pain block damaged the nerve in his upper leg.
The nurse kept assuring him that the rehab went “perfect” and that he was ahead of schedule.
The nurse showed no worry and kept smiling, insisting that my father would feel “200 percent better” the next morning.
She was not able to say if any of the medications were causing side effects, and despite continually reassuring him and his family, he was convinced he was doomed, and just lie there, projecting hopelessness and having given up.
Next day, two days out from the total knee replacement surgery, there was a complete turnaround.
He’d been given a different painkiller which was working — no pain — and not only that, but the rehab went great; he was in very high spirits. A complete turnaround.
So if your loved-one seems out of character with abnormal dejection and feelings of hopelessness the day after total knee replacement surgery, you must realize that the next day, he or she will likely feel just fine and ready to take on the world.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, peoplecreations
Can Two Supplements Reverse Plaque in Coronary Arteries?
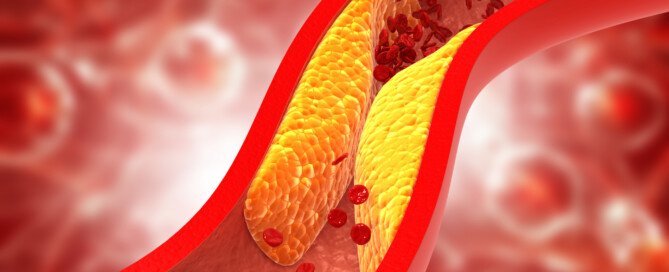
Can these two supplements actually reverse buildup of plaque in coronary arteries (heart disease)?
Yes — according to a very interesting study. But there are things you need to consider about the study.
“This study was performed in 2012 by researchers associated with Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center,” says Carlos González Quesada, MD, FACC, attending cardiologist with Cedars-Sinai Medical Center and a cardiologist with Cardiovascular Medical Group of Southern California.
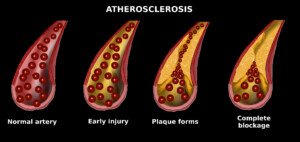
There is controversy over whether or not natural supplements can reverse coronary plaque buildup (a disease called atherosclerosis), which is strongly correlated to heart attack risk.
So the researchers studied a group of people (65 total at the start) who, when compared to the general population, have a two- to four-fold greater risk of heart attack.
This group was firefighters, and for the study, they took daily supplements of coenzyme Q10 (coQ10) and aged garlic extract (AGE).
Another group of firefighters did not take these supplements, so that a comparison could be made.
Nobody in the study was on statins. At the beginning of the study, all subjects had their calcium score taken (a numerical value of measurable plaque buildup).
The supplement group took 120 mg and 1,200 mg a day of coQ10 and AGE, respectively.
The control group took a sugar pill, but nobody knew which group they were in, and neither did the researchers.
The calcium scores of both groups, at the beginning, did not differ that much.
At the end of one year (during which the supplement group took their daily doses), another calcium score test was given.
The supplement group had about half the rate of coronary arterial plaque progression as did the placebo group, and this includes an adjustment for typical risk factors for plaque buildup.
What is the takeaway?
“Over the course of 12 months, 15 patients dropped the study due to loss to follow-up, withdrawal of the consent, or meeting exclusion criteria,” says Dr. Quesada.
“This is a significant number of patients who were not followed-up and may have impacted the result of the study.
“Although there was a small difference in the coronary calcium score and other markers of inflammation, this does not mean that there is a clinical difference.
“In other words, this does not prove that patients on the experimental group are less likely to develop heart attacks, strokes or develop premature death.
“Furthermore, the patients were only followed for 12 months, which is a short period of time.
“Results may have been different if the patient had been followed by several years.
“In my opinion, this clinical trial does not demonstrate a clinically relevant benefit of treating patients with a combination of coenzyme Q and aged garlic extract.
“To demonstrate any benefit, a larger clinical trial with longer follow-up is needed.”
In the meantime, here are very proven ways to prevent dangerous plaque buildup and possibly reduce soft plaque buildup on coronary arteries.
Shutterstock/Cessna152
Exercise. This means sustained aerobic activity at least three times a week for at least 20 minutes — something that gets your heart rate and respiration elevated: brisk walking, hiking, jogging, pedaling, stepping or a fitness class.
Avoid trans fats. This ingredient in processed foods also goes by the names shortening and partially hydrogenated vegetable oil.
Limit processed foods. Eat five to seven servings a day of any combination of fruits and raw vegetables.
If you’re overweight, lose weight. Practice portion control and stick to an exercise regimen.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}