

Should Obese Kids Do Pushups? Parents’ Guidelines

So here’s the answer to whether or not obese kids should do pushups:
This should be based on a case-by-case standard. There are interesting variables.
In general, as a fitness expert and former personal trainer, I’m not a proponent of obese people (children or adults) doing pushups. (more…)
Workout Myths that Sabotage Your Weight Loss

Don’t count on weight loss if you’re making mistakes with your APPROACH to working out, what you believe.
Here are 7 skewered beliefs that will kill any chance at losing weight. (more…)

Rotator Cuff Pain Heat Treatment Most Effective Application

Heat treatment for rotator cuff pain can be applied in different ways.
When my mother had pain from rotator cuff tendonitis as well as a few torn tendons, I noticed that there were two ways she often applied heat. (more…)

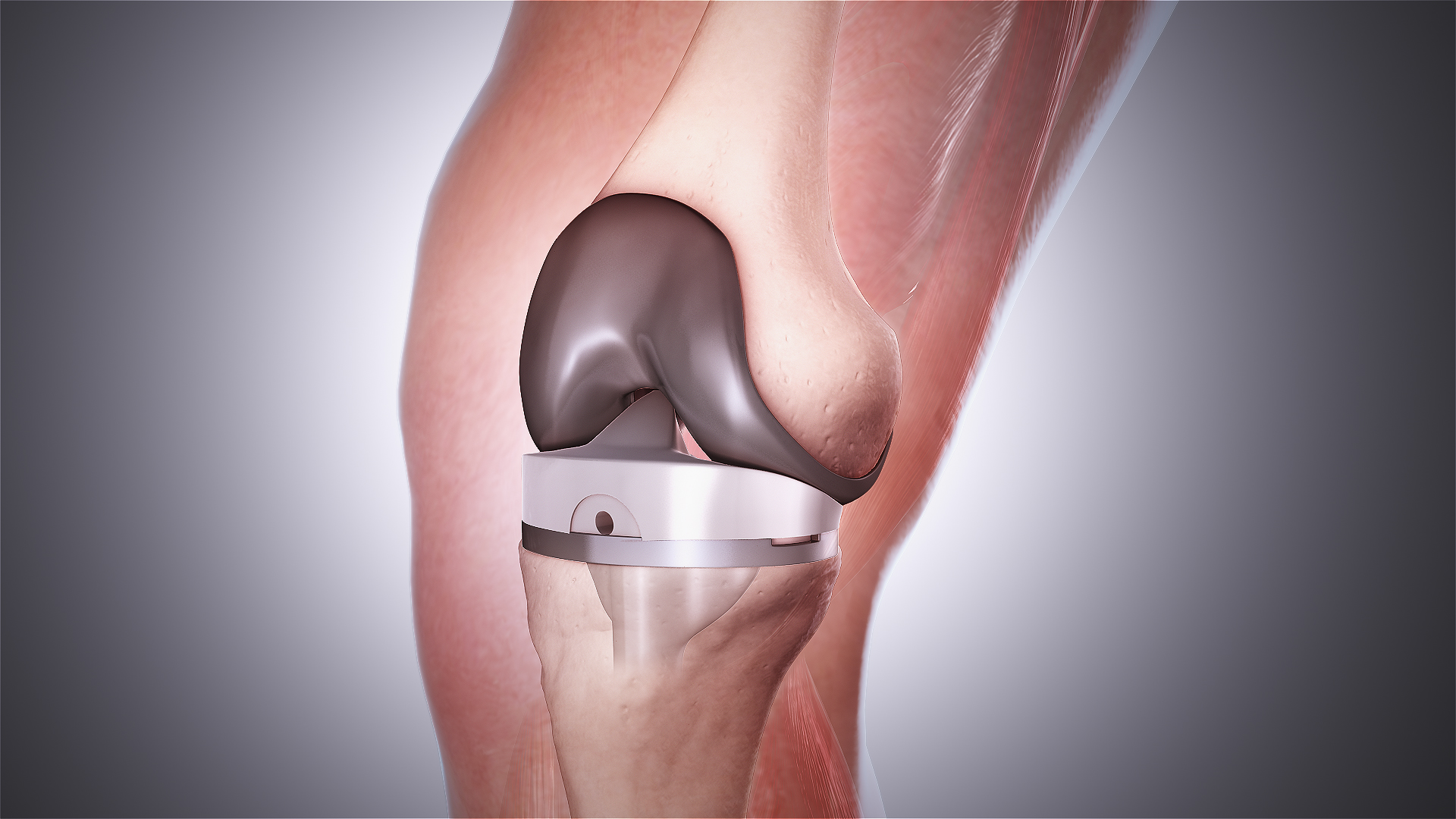
Upper Body Exercises for Total Knee Replacement Recovery

Here are great upper body exercises to do while recovering from a total knee replacement.
Total knee replacement doesn’t mean that two days after surgery, you’re bouncing around on your new titanium knee.
It takes weeks of therapy to get the body used to total knee replacement.
But a person with new total knee replacement must not neglect upper body exercise routines.
Total knee replacement surgery means that the patient not only is confined to a walker for days, but can only be up and about for very limited periods of time.

Ravedave, CC BY-SA
Following surgery, the patient will be spending a lot of time in a seated position, but from here, he or she can conduct exercise routines for upper body muscles.
The patient’s upper body muscles will benefit tremendously from weightlifting workouts.
Just because a person is confined pretty much to a chair doesn’t mean they shouldn’t perform exercise routines for the shoulders, back and arm muscles.
Upper Body Exercises You Can Do Following Knee Replacement Surgery
Dumbbells are a must. Several pairs of dumbbells should already be waiting for the patient’s arrival home.
The patient must sit in a stable seat that has no arm rests. Such seats can be found at many different stores.
The rule of thumb is to work whatever you CAN, and in the case of total knee replacement, it’s the upper body.
Biceps Curl
There are many ways to engage the biceps. One way is called concentration curls, and only one dumbbell is needed, as shown below. Plant your elbow in a comfortable spot on your upper leg, and begin curling.
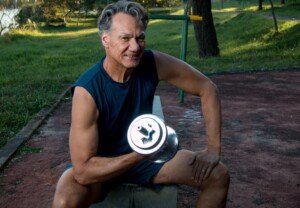
Shutterstock/Marcos Casiano
Side Raise
Hang arms straight at sides, then simply raise them on either side of you so that arms are parallel or a little past parallel with floor. Go no higher, then lower the dumbbells.
Though it’s usually done standing, it can also be done while seated.

Freepik/pressfoto
Shoulder Flexion (Front Raise)
Hold dumbbells with any palm angle, and, keeping arms straight and shoulders relaxed, lift them up in front of you so that your arms are parallel with floor. Go no higher, then lower. Can be done seated.

Shutterstock/ruigsantos
Shoulder Press
Hold dumbbells (or soup cans) at shoulder level, elbows pointing to floor, palms facing away from you. Now, simply push them above your head, straightening your arms.

Freepik.com, katemangostar
Triceps Press
Hold a dumbbell above your head, arms straight.
Keeping upper arms fixed in place, bend only lower arms so that the weight is behind your head, elbows pointing to ceiling. Then straighten arms.

Overhead Band Pull
Hold either end of an elastic exercise band and pull in opposite directions. Of course, do NOT copy the model’s lower body. Do this exercise while seated in a chair.

Shutterstock/Alexander Raths
Row
Loop a band around a secure object, then begin pulling the handles towards your chest. For a knee replacement patient, this exercise is best done while seated.

Shutterstock/Aaron Amat
How many sets?
I recommend four sets per exercise with 1-2 minutes’ rest in between. You have all the time in the world, remember.
Also realize that total knee replacement means severe restriction in calorie-burning. It’s unlikely that you can overdo upper body exercises.
How many reps?
Eight to 20. If you can do more than 20, use heavier weights.
How often?
Never do the same exercise two days in a row.
Three times a week will work if you apply moderate effort; and twice a week will work if you apply intense effort.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Scientific Animations, Creative Commons/BY-SA/Attribution-ShareAlike 4.0 International

Exercises that Replace Pushups for Obese Women & Men

Pushups are very difficult for obese people, but if you’re plus size and want to strengthen your chest, shoulders and arms, there are substitutes you can do instead of pushups. (more…)

Should Obese People Do Pushups?

If you consider yourself “fat,” could you benefit from doing pushups?
When I was a personal trainer I had many overweight clients. You may want to hold off on pushups for a while. (more…)

Which Is Better for Losing Butt Fat: Squat & Leg Press or Cardio?

This article explains which works better for losing butt fat, cardio exercise or squats and leg presses, and why.
Do you think you have a lot of fat in your butt and are wondering if you should do cardio exercise or try strength training like squats and leg presses?
If you had to choose between cardio exercise and squats plus leg presses for taking off fat in your butt, go with the strength training.
Fact is, cardio will do very little to slash excess fat in your butt.
Cardio is commonly done steady-state style. This means a constant pace is maintained, though there may be fluctuations here and there.
Nevertheless, it’s a continuous pace that enables you to maintain it, and some people maintain pacing for up to an hour on cardio machines.
Another form of cardio is an aerobics class, or walking or jogging outdoors. These too, fall under the style of steady state.
The reason these are not very effective at busting butt fat is because they recruit slow twitch muscle fiber.
Intense strength training recruits fast twitch fiber, which requires more fat for fuel than slow twitch.

Shutterstock/Aleksey Boyko
Furthermore, steady state cardio does not trigger the hormonal response that intense strength training does.
The superiority of squats and leg presses for losing butt fat:
Performing sets with heavy weights that make 8 to 12 repetitions extremely challenging can trigger a significant hormonal response.
When you lift weights that push you to your limit within this rep range, your body undergoes intense physical stress.
This stress signals the release of various hormones, such as testosterone, growth hormone, and cortisol, which are involved in muscle repair, growth and fat metabolism.
The hormonal response is particularly pronounced when you engage large muscle groups or multiple muscle groups simultaneously.
For example, compound exercises like squats and leg presses involve multiple large muscles, leading to a greater overall hormonal release.
This heightened hormonal response facilitates muscle recovery and growth while enhancing fat metabolism.
The fat-burning effect is substantial, as these hormones continue to circulate in elevated levels for several hours after your workout.
This phenomenon, known as excess post-exercise oxygen consumption (EPOC), means that your body remains in a heightened state of calorie burning even after the exercise session is complete.

Shutterstock/Reshetnikov_art
Yes: In the hours following an intense squatting and leg press session, your body will be burning fat at an accelerated rate. This includes the fat in your buttocks.
Leg presses can be done after barbell squats or before; it’s personal preference.
A 45 minute session of the leg press, the squat and the deadlift will burn far more fat than 45 minutes jogging on a treadmill or taking a Zumba class, and this fat burn will occur all over the body, including your butt.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Kokhanchikov

How to Get Strong Enough to Do Pushups for Repetitions

Here are four routines that will get you strong enough to do pushups.
With the right training, women and “weakling” men can get strong enough to do many solid pushups. (more…)

Should You Hold Onto a Treadmill at High Incline?

If you’re part of the hold-on-for-dear-life high treadmill incline camp, find out why you’re wasting your time, big-time.
Holding on at a high incline is so very wrong, on so many levels, I don’t even know where to begin.
Let’s begin this way: Next time you’re at the gym, look at people from the side as they walk a high incline and hold onto their treadmill. Do you notice anything peculiar?
If not, close your eyes and imagine viewing someone from the side, walking up a hill.

Source: Freepik.com, tirachard
Now compare that person’s profile to the treadmill user’s profile. Do you notice anything strange?
The outdoor hill walker’s body is vertical, forming a much less-than 90-degree angle with the hill in front of her.
Look again at the very top image of the woman holding onto an inclined treadmill.
The walker’s body is 15 degrees tilted back — 15 degrees because she’s using a 15 percent incline and leaning all the way back with it.
Her body is tilted back at the same angle as the incline because her hands are gripping the bar, arms straight.
She’s essentially walking on a flat surface because she’s reproducing the same angular relationship to the walking surface as someone who’s walking on a flat tread. This is a pseudo-incline walk.
To simulate an uphill walk, remove your hands, which will force your body to be vertical, reducing the angle between your body and the tread before you.

This will require increased hip, knee and ankle flexion, which is why uphill walking is more taxing than flat movement.
Can’t sustain this? Solution: REDUCE THE SPEED.
If you keep yourself pulled forward with bent arms, this is still cheating because your hands, arms and shoulders are keeping your body vertical, rather than any power from your lower body.
This absolutely is NOT the same as walking hands free. It does NOT “all even out.”
Now if you hold onto the side of the treadmill at a high incline, your body won’t lean back so much. However, the rails are still supporting you.
When I was a personal trainer I’d periodically get a client who was used to walking a high incline at 3.5, even 4 mph, and of course, clinging onto the front or side of the machine.
The metrics — high incline and fast waking speed — made them think they were in great shape.
However, I’d get them on a treadmill and set the speed at only 2 mph, then raise the incline to 15 percent.
Initially they’d think that 2 mph was way too slow, even though I’d instruct them to keep their hands off the treadmill. They’d look at me like, “What? This is way too easy, TWO miles an hour!”
And at first, 2 mph even hands free at the highest incline will seem like very easy work.
But quite predictably, these clients began visibly struggling and breathing heavily within several minutes.
Pretending that it was as easy as they’d first thought became increasingly difficult.
Within several minutes they’d grab the machine, panting, unable to walk any more at 2 mph without holding on.
I’d point out that 2 mph OR SLOWER is about the same speed they’d walk on an actual outdoor hill; it’s not slow at all when it’s done on a high incline!
If you’ve been holding onto a treadmill at high inclines and setting the speed at 4 mph, try this experiment: Set it at 2 mph at 15 percent.
Without any holding on whatsoever, see how long you can sustain this. Don’t be surprised if very soon, your calves begin burning and/or your lower back begins aching.
That’s because when you hold on, the calves and core do VERY LITTLE work. Because they’re not used to the workload of hands-free incline walking, they quickly burn and ache when you finally do let go.
Holding onto the treadmill also promotes an unnatural gait and burns far fewer calories than what the console displays.
Solution: Use the incline, hands OFF, at 1 to 2 mph, for short periods, alternating with hands-free walking on a flat setting.
Over the next several weeks (depending on how often you follow these instructions) those dormant muscles will become more efficient and no longer ache or burn. You’ll also notice an improvement in aerobic ability.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Top image: ©Lorra Garrick

Why Women Love the Hip Abductor Machine

So why do women love the hip abductor machine, and men don’t care for it so much?
The hip abduction machine targets two buttocks muscles: the gluteus medius and the gluteus minimus.
However, if you’ve ever used the hip abduction machine, it feels as though the outer thighs are being worked more than the butt.
The diagram on the hip abduction machine shows the area of the lower body that gets worked, and the outer sides of the thighs are highlighted.
Women see this and believe that hip abduction exercise will shave inches off their outer thighs.
Women, so much more than men, are concerned about excess fat in the thighs, particularly the outer thighs.

This is a hot button for throngs of women, and that’s why they gravitate towards the hip abduction machine.
However, another group of women uses the hip abduction machine to tone the buttocks.
Remember, this equipment targets the gluteus medius and gluteus minimus, which are buttocks muscles.
These muscles, though, are responsible for the joint action of hip abduction.
This joint action, against resistance, either with equipment, tension tubing, calisthenics or inline skating (especially up hill), will tone and strengthen these buttocks muscles.
But working these muscles will not – absolutely will not – take inches off the outer thighs!
These are small, relatively weak muscles. They do very little to power the legs during running, strenuous walking, hiking, and exercises like squats, deadlifts and leg presses.
To shave inches off the outer thighs, a woman must increase her body’s energy demands.
There is no better way to do this than to do exercises that target large muscle groups:
- the quadriceps (front thigh muscles
- hamstrings (back thigh muscles)
- gluteus maximus (main buttocks muscle; it’s bigger than you think)
- and large upper body muscles (back and chest).
Targeting these muscles with very challenging resistance loads — as shown in the following images — will force the body to use stored fat – including fat stored in the outer thighs — for recuperative energy!

Deadlift. Shutterstock/Tyler Olson

Sled push

Dumbbell deadlift. Shutterstock/Robert Taylor

Lat pull-down, wide grip

Dumbbell shoulder/chest press
Combine this with high intensity type of cardio and sensible eating habits, and voila, a woman will experience inches lost in her outer thighs.
As for that hip abduction machine, it’s a good piece of equipment to tone and strengthen the smaller butt muscles.
It’s also great to keep these muscles in shape for inline skating if you haven’t been inline skating for a while due to injury, lack of time or cold weather.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}