
Can You Fake Sleep Apnea and Fool the Test ? Yes and No

Who’d want to fake sleep apnea and try to fool the sleep study test? A person wanting to scam an insurance company.
A young man wanted to know if he could fool a sleep study test into yielding a positive result for sleep apnea – to gain some kind of insurance benefit of which I don’t recall the details.
But I found his thread in a sleep apnea forum.
Ethics aside, CAN a person fake sleep apnea enough to fool any kind of test for it?
“To my knowledge, not really,” begins Joseph Krainin, MD, board certified in sleep medicine and neurology and founder of the online sleep apnea clinic Singular Sleep.
“You can hold your breath and fake central sleep apnea but, unless you have a serious cardiopulmonary problem such as COPD or congestive heart failure, you likely won’t be able to fake the typical oxygen desaturations that follow these breathing events — so a good sleep doctor will pick up on this,” continues Dr. Krainin.
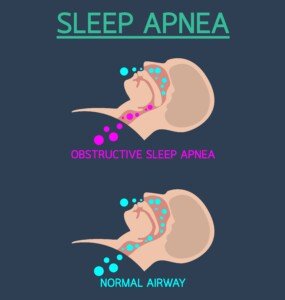
What would you need to do to fake obstructive or central sleep apnea?
Shutterstock/iLoveCoffeeDesign
In order to fake sleep apnea, you’d have to be able to be in bed throughout the night while remaining wide awake enough to repeatedly “fake” the condition.
If you let yourself fall asleep, you just botched your scam.
So first of all, you’d have to succeed at fighting the urge to fall asleep – which can be done if you prepare days ahead of time by switching your schedule to that of a night shift worker.
Years ago I got a third shift job and was asked to come in the night of the day I was hired. I said, “I don’t think so, but I can come in the next night.”
And come next night, I had no problem being alert from 11 pm to 7:30 am.
But lying in bed in a dark room can certainly encourage falling asleep even if you’ve trained your body for several days to function alertly on a third shift schedule.
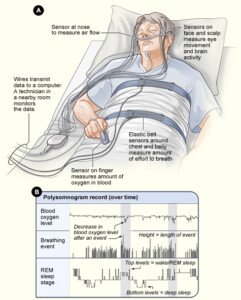
Sleep study
Next, assuming that you CAN just lie there for six, let alone eight hours straight, eyes closed but awake, without going batty, you’d have to frequently stop breathing long enough to become very uncomfortable.
That’s more uncomfortable than you ever were as a child when you’d time with a stop watch how long you could hold your breath or see if you could swim across an entire swimming pool underwater without coming up once for air.
So try doing that, while lying in bed, for at least six hours – let’s say, 10 times an hour.
But remember, you’d have to hold your breath past the point that you did when you were a child (or adult) playing breath-holding games with friends.
But there’s more to faking a sleep apnea test than lying still and awake for at least six hours and repeatedly holding your breath long enough to induce gasping.
Dr. Krainin says, “You can’t really fake valid-looking snoring on a sleep study, and attempting to fake obstructive apneas — if you could even figure out how to approach this — would probably be pretty obvious to an expert reviewer.”
 In 2013 Dr. Krainin was elected a Fellow of the American Academy of Sleep Medicine, an honor reserved for sleep doctors who’ve made significant contributions to the field in education, research and service.
In 2013 Dr. Krainin was elected a Fellow of the American Academy of Sleep Medicine, an honor reserved for sleep doctors who’ve made significant contributions to the field in education, research and service.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Maria Sbytova
How Does Inconsistent CPAP Use Affect Sleep Apnea?

People who find the CPAP device very uncomfortable may end up using it inconsistently and wonder how bad their sleep apnea can still be with this approach.
Some people can’t tolerate sleeping with a mask for a variety of reasons. (more…)

13 Things Never to Say to Someone Who Has Acne or Pimples

This isn’t about deliberately nasty comments to those with acne, but so-called well-meaning comments that are actually quite hurtful, rude and thoughtless. (more…)

Can Cancer Make Your Urine Smell Fishy?

There are numerous causes of fishy smelling urine, and you may be wondering if cancer is one of them if you’re suffering from this situation.
If your urine has a fishy odor, it’s exceedingly unlikely that cancer has anything to do with this.
You probably have one of the following causes of fishy smelling urine.
Antibiotics. These drugs may cause urine to have an unpleasant odor that one might describe as fishy.
Asparagus. Yes, eating this healthful vegetable can make urine stink.
Kidney stones. There may be pain in the lower back or groin, but there may also be a foul smell to your urine.
Phenylketonuria. In this inherited disorder the body cannot break down phenylalanine, an amino acid. Urine may have a putrid or somewhat fishy smell.
Prostatitis. Inflammation of the prostate can cause burning urination and a bad smell.
Trimethylaminuria. This genetic condition causes the whole body to smell fishy, and the urine may have a particularly strong stench of rotten fish.
Urinary tract infection. Along with classic symptoms of a frequent feeling that you have to relieve yourself, burning while urinating and cloudy urine, you may notice a fishy odor.

Shutterstock/mistaht
Vaginitis. Inflammation of the vagina often causes itching and discharge.
When bacteria is the cause, the condition is called bacterial vaginosis and can definitely result in fishy smelling urine – because the vaginal discharge itself is fishy in odor and can intermix with urine output.
PROSTATE CANCER
Can prostate cancer change the odor of urine?
“No; humans can’t detect a difference,” says Jonathan W. Simons, MD, President and Chief Executive Officer of the Prostate Cancer Foundation, David H. Koch Chair.
Dr. Simons continues, “So, while humans can’t smell prostate cancer, research continues as to what is in the urine that a dog can smell and whether a new kind of biosensor could be invented like an artificial dog’s nose superior to a PSA test.”
Bad Urine Odor but not Fishy
Dehydration can cause urine to have a “strong” odor, but it just smells more “uriny,” or almost like what a port-o-potty smells like that hasn’t been cleaned for a while.
Diabetes, too, can alter the natural odor of urine, but the change is that of an odd sweet smell because there’s more sugar in the excrement.
Don’t jump to the conclusion that you might have cancer just because your urine has a stinky fishy smell.
But certainly, you should see a doctor to find out what is causing the problem.
 Dr. Simons is an internationally recognized physician-scientist, oncologist and acclaimed investigator in translational prostate cancer research.
Dr. Simons is an internationally recognized physician-scientist, oncologist and acclaimed investigator in translational prostate cancer research.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/ARENA Creative
Sources
mayoclinic.org/diseases-conditions/vaginitis/home/ovc-20258665
mayoclinic.org/diseases-conditions/prostatitis/home/ovc-20271415
mayoclinic.org/diseases-conditions/urinary-tract-infection/symptoms-causes/dxc-20344304
mayoclinic.org/diseases-conditions/phenylketonuria/basics/definition/con-20026275#808080;”>link.springer.com/article/10.1007/s11306-012-0425-5
mayoclinic.org/diseases-conditions/vaginitis/symptoms-causes/dxc-20258675
Did Las Vegas Shooter Paddock Have a Brain Tumor?
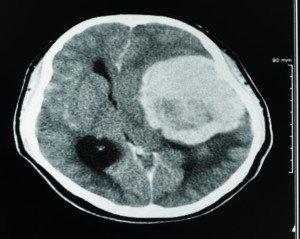
It may seem that the most plausible explanation for Stephen Paddock’s Vegas shooting rampage is a brain tumor.
The idea of a brain tumor causing Stephen Paddock’s premeditated savagery has not been broached by the media.
How does a man (albeit being raised by a violent criminal) who (apparently) lives extremely normally for decades suddenly decide to wipe out as many people as possible with a massive arsenal of automatic rifles?
Brain Tumor vs. Superficial Normality
Can a brain tumor cause a previously normal (or so it seems) person such as Stephen Paddock to premeditate a mass shooting and then carry out this act?
“Aggression and violence have rarely been presented in the neuro-oncology [brain cancer] literature, but have been well documented in stroke and dementia literature,” says a report in Journal of Neuro-Oncology (Sept. 2009, Villano et al).
The report focuses on the case of a man, 55, with a glioblastoma type of brain tumor, who committed an act of violence against his wife.
But that’s a far cry from assembling dozens of rifles and shooting at thousands of people from a quarter mile away.
In 1966 Charles Whitman (“Texas Tower Sniper”) killed 16 people, most from a tower at the University of Texas at Austin.
He was killed by police. A subsequent autopsy revealed a small brain tumor.
Intense analysis was done by various experts. No definitive conclusion was ever drawn regarding the effect the brain tumor may have had on the decision to go on a killing spree, especially since there were multiple factors in Whitman’s life and history that came across as far more contributing.
In short, though a very intriguing topic of conversation, it’s not likely a brain tumor made Stephen Paddock strategically plan a mass assault on 22,000 people from the 32nd floor of the Mandalay Bay hotel. Do not bet on it.
Instead, place the bet on a common phenomenon: People can be as disturbed as heck without those “around” them ever knowing.
Ever hear of that old saying, “The evidence is right under their nose but they don’t see it”?
What’s more likely, and a lot more likely, is that those who “knew” Paddock best did not know him as well as they believed.
For example, just because someone is your brother doesn’t mean you really know him.
Yes, you grew up with him. But the last few decades, or more, could have consisted of only occasional (e.g., holidays, weddings, graduations) in-person contact — that lasted only days.
You only see the superficial, the game face, the guest-in-the-house personna — which can easily be switched on and off by a sociopathic individual.
Emails, texts and even regular Skyping sessions are not enough to really know what’s going on in even your own sibling’s mind.
In other words…did anyone really know this deranged and evil man? Even his own mother might not have had much contact with him over the years.
Do YOU really know the people who live on your street even though you see them all the time?
As that saying goes, “There are psychopaths among us.” The most seemingly normal person you know may be a vicious person behind closed doors. And usually, the creepiest people you know are the last ones to commit murder.
No matter how shocking Stephen Paddock’s behavior was to those who knew him, it’s still a very unlikely possibility that a brain tumor was the driving force.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Richman Photo
Soueces
link.springer.com/article/10.1007/s11060-009-9850-3
garylavergne.com/LegacyTowerChronicle-Lavergne.pdf
Can Diabetes Cause Numbness on Only One Side?
Numbness on one side of a large portion of the body is not normally caused by diabetes. Other causes can be an emergency.
It also depends on how much of the body you’re referring to. (more…)
Can Anemia Cause Muscle Weakness?

One of the classic signs of anemia is a feeling of overall weakness and fatigue that may seem to originate from the muscles.
Symptoms of anemia can be anything from mild to severe, and there’s quite a few potential symptoms. (more…)

How Well Can Amitzia Treat IBS-C ?

Have you tried Amitzia as a treatment for your IBS-C?
Many people who suffer from IBS-C notice that over time, laxatives that once worked begin to lose their steam.
They ultimately become ineffective and the patient is back to square one with their constipation.
Amitzia (generic name lubiprostone) has been FDA approved for treating chronic constipation of unknown origin.
Irritable bowel syndrome is a condition of exclusion — a diagnosis given when all other possible causes of the constipation (through extensive testing including colonoscopy) have been ruled out.
“Amitzia is a medication to improve bowel movements in constipated people,” says Lawrence Hoberman, MD, a board certified gastroenterologist and creator of EndoMune probiotic products.
“Side effects include nausea, bloating, cramps and diarrhea.”
Though for some people, diarrhea may be preferable to constipation, it’s also possible that Amitzia can result in stool formation that doesn’t quite qualify for diarrhea, and is a lot easier to void than the previous constipated bowel movements.
But then there are also the possible other side effects, as mentioned.
Dr. Hoberman says, “Because of the side effects, it is not the drug of choice for irritable bowel syndrome (IBS-D).”
Nevertheless, all the patient can do is try it and see what happens.
This should be discussed with the patient’s gastroenterologist.
A study in Alimentary Pharmacology and Therapeutics (Jan. 2008, Johanson et al) notes that though Amitzia can be effective even at low doses, it’s associated with more GI side effects at higher doses (especially 48 mg/day).
 With 40+ years’ experience, Dr. Hoberman is an expert in probiotics. He has extensive first-hand experience treating a variety of digestive health issues and has seen the dramatic results probiotics have had on his patients. endomune.com/meet-dr-hoberman
With 40+ years’ experience, Dr. Hoberman is an expert in probiotics. He has extensive first-hand experience treating a variety of digestive health issues and has seen the dramatic results probiotics have had on his patients. endomune.com/meet-dr-hoberman
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Aaron Amat
Sources
gastrojournal.org/article/S0016-5085(07)00793-7/abstract
springer.com/article/10.1007/s10620-011-1702-2
tandfonline.com/doi/abs/10.1517/14656560802631319
onlinelibrary.wiley.com/doi/10.1111/j.1365-2036.2008.03629.x/full
onlinelibrary.wiley.com/doi/10.1111/j.1365-2036.2011.04983.x/full
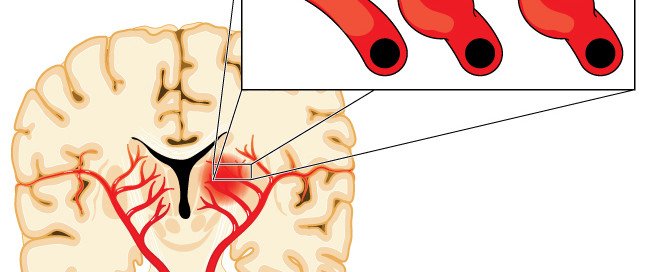
Can Aneurysm Cause One Pupil to Be More Dilated than the Other?
If one pupil is dilated this CAN be from an aneurysm.
One dilated pupil usually represents a recent change in the aneurysm or possible small sentinel (early warning) bleed. In the case of bleeding, usually there is associated sudden onset headache.
Most medical sites will list “dilated pupils” as a possible symptom of an aneurysm.
However, when only one pupil is dilated in a person, this is far more concerning than when both are.
When only one pupil is dilated, or unilateral dilation, this is called anisocoria.
Pupils of uneven size may also be a benign finding, and in this case is called physiological anisocoria.

Physiological anisocoria. Russavia [CC BY 3.0
“Typically, the difference in pupil diameters is less than 1.0 mm and may vary from day to day,” says Dr. Siddiq.
“Aneurysms can also cause anisocoria, particularly in a location known as the posterior communicating artery or PCOM.”
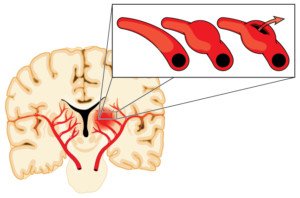
Aneurysms and Unequal Pupil Size
“Here, aneurysm grows close to the third cranial nerve and can sometimes cause sudden compression of the nerve and cause a third cranial nerve palsy, which will occasionally manifest as dilatation [dilation] of the pupil on the side of the aneurysm,” continues Dr. Siddiq.
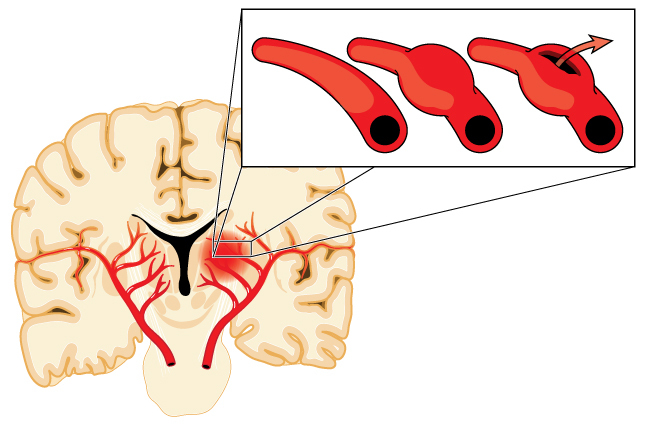
“Usually this dilatation is painless, but pain could be associated with it, indicating a possible recent rupture of the aneurysm.
“The pupillary dilatation is not a variable but may still be responsive to light. There may or may not be double vision associated.
“Any sudden change in the size of the pupil on a previously normal individual should raise suspicion.
“Interestingly, diabetes can also cause these symptoms, so urgent tests are required to rule out a ruptured PCOM aneurysm.”
As frightening as this may sound, there is no reason to obsess over the size of your pupils by frequently inspecting them in magnifying mirrors.
Nevertheless, it’s always a smart idea to be informed. People have suffered from ruptured aneurysms because they ignored the warning signs.
Other Dangerous Causes of Uneven Pupil Size
“Anisocoria, or unequal pupil size, may be an early sign of an impending neurologic emergency and often suggestive of a life threatening condition affecting cranial nerve function, such as tumour compression, intracranial hypertension with impending uncal herniation, expanding intracranial aneurysm, or haemorrhage,” says a paper in the Indian Journal of Anaesthesia (July/August 2010, Yalcin et al).
Symptoms that an Unruptured Aneurysm May Cause
• Pain above and behind an eye
• A dilated pupil
• Change in vision
• Numbness, weakness or paralysis of one side of the face
• Drooping eyelid (ptosis)
Note the word “A” before “dilated.” This means one pupil – which means pupils of unequal size.
The challenge of physicians is to determine if one pupil is actually dilated more than it should be, given the lighting conditions, or if one pupil is more constricted than it should be.
Other symptoms that are present, plus recent medical history, are crucial in the determination of how to proceed with a patient who presents with unequal pupil size.

Dr. Siddiq is fellowship-trained in endovascular surgical neuroradiology and vascular neurology from the University of Minnesota Medical Center. His areas of special focus also include brain aneurysms and carotid disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Blamb
Sources
ncbi.nlm.nih.gov/pmc/articles/PMC2943725/
mayoclinic.org/diseases-conditions/brain-aneurysm/basics/symptoms/con-20028457
Can a CT Scan Show Crohn’s Disease?

“A CT scan can show signs of Crohn’s disease,” says Alan Gingold, DO, a board certified gastroenterologist with Central Jersey Ambulatory Surgical Center.
A CT scan can easily show the thickened bowel wall that comes with Crohn’s disease.
And that’s just the beginning of what computerized axial tomography can show with this inflammatory bowel disease.
However, this doesn’t mean that a CT scan, all by itself, diagnose Crohn’s disease. It’s one of many routes to the correct diagnosis.
An abdominal CT scan takes five to 20 minutes and may involve contrast dye to improve viewing.
The value in a CT scan is that it rules out complications from Crohn’s disease such as infections, obstructions, strictures and bowel perforation.
“Inflammation, enlarged lymph nodes, fistulas, abscesses, strictures can all be seen in Crohn’s disease and can be seen on CT scan,” says Dr. Gingold.
There is a type of CT scan called enterography which translates to mapping out the intestines.
It requires a contrast dye for enhanced quality of the image of the small bowel relative to other organs. Areas of inflammation or more subtle blockages can be seen.
According to a 2014 report in the American Journal of Roentgenology (Gore et al), the CT scan is the “premier imaging procedure for evaluating mural and extraintestinal manifestations of IBD.”
CT plays a crucial role in the detection of abscesses (infections), complications beyond the intestinal tract and other issues associated with Crohn’s.
“Pathology from biopsy taken during an endoscopic examination in the proper clinical setting is the gold standard for diagnosis of Crohn’s disease,” says Dr. Gingold.
“CT scanning is usually used to help aid in the initial diagnosis or to follow progression of disease or response to treatment.”
Why CT Scan Is not the Gold Standard for Diagnosis
Dr. Gingold explains, “Other things that can look similar to Crohn’s disease on CT scan would include cancer, appendicitis and certain infections such as Yersinia, campylobacter, salmonella Entamoeba and rarely tuberculosis.”
 Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}