
A brain tumor can mimic BPPV symptoms. In fact, patients with a brain tumor have been misdiagnosed as having benign paroxysmal positional vertigo.
The biggest symptom overlap between a brain tumor and BPPV:
• Vertigo (a type of “dizziness” in which the patient perceives that the room is moving, even revolving, especially in response to a change in body position). Vertigo from a brain tumor can actually be triggered by positional changes.
• Nausea
• Vomiting
More than one type of brain tumor can produce symptoms that can be mistaken for BPPV.
Of course, an MRI can immediately determine the presence of a brain mass.
The high incidence of benign paroxysmal positional vertigo means that automatic MRI’s for every single patient reporting the symptoms would be impractical to the public health system.
However, there are certain criteria that would justify ordering an MRI: criteria that would point towards a possible non-benign positional vertigo.
Brain Tumor vs. BPPV
There are several types of brain tumor whose symptoms can be mistaken for BPPV.
“Statistically, one is more likely to have BPPV vs. tumor (vestibular schwannoma) that would cause similar presentations,” says Lenny Cohen, MD, founder of Chicago Neurological Services; diplomate of the American Board of Psychiatry and Neurology.
“BPPV incidence are 100 cases/100,000 population, while vestibular schwannoma is only 1/100,000.”
A vestibular schwannoma, also known as an acoustic neuroma, is a benign brain tumor that’s located in the inner ear canal.
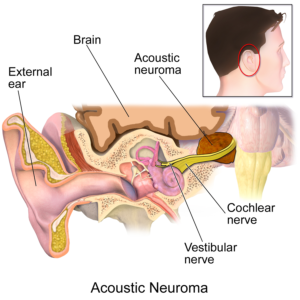
Blausen.com staff
This is one kind of brain tumor that can cause symptoms that the patient might believe is BPPV.
“Secondary symptoms like hearing loss can be associated with vestibular schwannoma,” says Dr. Cohen.
The hearing loss is usually sudden, and there may also be sudden-onset tinnitus (ongoing ringing or hissing sound) in the ear.
But these very slow growing tumors can cause what patients describe as dizziness and feeling off-balance.
Other brain tumors, though, can also mimic BPPV, to the extent that a misdiagnosis can occur – and according to medical literature, HAS occurred.
A review of patients who were seen in the Department of Otolaryngology at Ohio State University between July 1992 and August 1996 identified five cases of brain tumors that had been misdiagnosed as BPPV.
• Two meningiomas
• Glioma
• Lipoma
• Vestibular schwannoma (acoustic neuroma)
Another study revealed that the following types of brain tumors resulted in misdiagnosis:
• Hemangioblastoma
• Metastases from another part of the body
When to Get the MRI
Dr. Cohen explains, “Symptoms of BPPV are self-limiting and usually resolve within three to seven days [though they can go on for several weeks] — while tumors will have persistent symptoms.”
Even when BPPV symptoms persist for weeks – because the patient has not sought treatment and has not undergone any positional maneuver treatment – the symptoms do not progress over time.
The symptoms may be debilitating enough to incapacitate the patient – but this usually occurs suddenly, out of the blue, from the get-go.
For instance, the patient may awaken one morning and experience a spinning room upon rising from bed. The vertigo can be so bad that the patient is at risk for falling.
But even if severe BPPV isn’t resolved (either spontaneously or via a maneuver), the symptoms remain the same: basically the vertigo, and perhaps nausea and vomiting.
In BPPV, nothing else develops that would indicate a brain mass such as new-onset headaches (especially in the morning), changes in behavior or vision, one-sided weakness, clumsiness or seizures.
In short, symptoms that don’t respond to BPPV treatment, plus other symptoms or new symptoms, are suspicious for a non-benign cause – warranting an MRI.
Guidelines for when to Seek an MRI
• Presence of other neurological symptoms not associated with BPPV (unexplained sleepiness, memory problems, difficulty with fine motor skills, impaired judgement, speech difficulties, difficulty swallowing, facial weakness or numbness).
• If there’s more than one brain tumor (from metastases), the symptom array may be quite varied.
• Repetitive, uncontrolled eye movements (nystagmus) without vertigo in positional diagnostic tests.
• Nystagmus that goes in different directions in positional tests done at different times.
• Vertigo unresponsive to positional maneuvers.
Positional Maneuvers
The most common is the Epley maneuver. “Epley maneuver is a good technique to not only move crystals out of semicircular canals, but also to ‘re-educate’ how one perceives motion and therefore diminish perception of dizziness/vertigo,” says Dr. Cohen.
The crystals, or canaliths, are particles that float in the inner ear and help maintain our balance and sense of space.
When they spontaneously float out of their proper location, BPPV results.
The Epley maneuver can be self-applied.
 Merging traditional medicine with alternative therapy, Dr. Cohen uses advanced science and a devotion to personalized care to provide men and women a unique approach focused on their long-term health and well-being.
Merging traditional medicine with alternative therapy, Dr. Cohen uses advanced science and a devotion to personalized care to provide men and women a unique approach focused on their long-term health and well-being.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.

































