

Brain Tumor Headache vs. Normal Headaches
Is there a difference between brain tumor headaches and normal headaches?
Answers to brain tumor headache questions you could never find are now right here. I asked an expert questions about brain tumor headaches that you’ve wondered about.
Headaches are so common.
Is there a way to tell the difference between brain tumor headaches and regular headaches?
I asked Virginia Stark-Vance, MD, who specializes in the field of neuro-oncology (treatment of brain and spinal cord malignancies), about BT headaches vs. regular headaches.
She is coauthor of the book, “100 Questions and Answers about Brain Tumors.”
Do BT headaches necessarily feel like a “brain tumor headache”? Or can it feel normal?
Dr. Stark-Vance: “A tension headache, often felt as tightening in the back of the head or neck, is a common symptom in brain tumor patients who have a tumor in the back of the head, or causing pressure on the lateral ventricles, the spinal fluid spaces in the middle of the brain.
“The pressure from the tumor seems to transmit to the back of the head and downwards.
“It is not unusual for such patients to see a chiropractor, thinking they have a neck problem.”
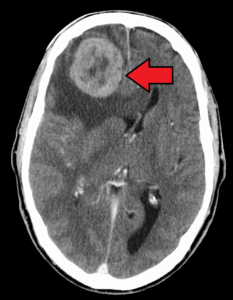
Credit: James Heilman, MD
What are unique characteristics of BT headaches that differ from regular (tension, dehydration) headaches?
“There are no truly unique characteristics, although some patients will have an increase in pain with changes in barometric pressure, during a flight, or with changes in altitude.
“Some have a headache when bending forward or coughing. However, absence of these signs isn’t unusual either. Some brain tumor patients never have a headache.”
How do BT headaches differ from migraines and cluster headaches?
“Patients who have a history of migraines who develop a tumor often say their ‘tumor headache’ is different from their ‘migraine’ headache. They are not relieved with the same medication.
“Often the migraine headache is accompanied by nausea and sensitivity to light. Most brain tumor headaches are not accompanied by nausea.”
Are BT headaches necessarily confined to one area (pinpointed), or can they be in the entire head?
“Some patients describe their headache as poorly localized, at the top of the head, or the whole head. Some never describe it as a headache, just as ‘pressure.’
“They usually do not throb, but can radiate to the top of the head, behind the eye, or the back of the head.”
Is it typical or possible for the first incidence of BT headaches to be unbearable pain?
Or is the first headache almost always a mild pain?
“Sometimes patients have ‘the worst headache of their life’ when they present with a brain tumor, almost like an intracranial hemorrhage.
“More commonly, a patient will describe a more subtle headache; it can come and go, sometimes worse in the morning.
“Many patients have not even taken Tylenol for a headache.”
What percentage of patients experience only headaches as a symptom?
“Some patients have headache as the only symptom, or as the first symptom. Obviously not every patient with a headache gets a CT or MRI.
“Often a physician will look for some other problem (weakness, visual problems, dizziness) before ordering a scan on a patient with a headache.
“Some physicians have been successfully sued because they didn’t order a scan after the patient complained repeatedly of headache, but the physician didn’t order the scan because no other signs or symptoms were present.”
What about the tumor causes headaches?
“A ‘brain tumor headache’ in the classical sense, is a headache caused by the pressure of a tumor against the meninges, skull, or another structure that has pain receptors.
“The brain has no pain receptors, per se, but that doesn’t mean all patients are free of headache.”
How big does a BT need to be before it starts causing headaches?

“Some large brain tumors never cause headache; some small brain tumors can cause very severe headaches.
“The latter occurs with tumors in the ventricles that block the flow of spinal fluid.”
Can a person have a BT and NEVER have headaches?
“About 50% of brain tumor patients have headache at the time of diagnosis. It has been estimated that 10 million people in the U.S. have a headache on any given day.
“Therefore, the vast majority of people having a headache do not have a brain tumor, since even counting patients with metastatic brain tumors, less than 100,000 people are walking around with a brain tumor of some type.”
Do brain tumor headaches respond to aspirin or ibuprofen?
“Brain tumor headaches may respond to Tylenol, ibuprofen, Darvocet, Vicodin, Fioricet, and many other medications.
“Sometimes the swelling or edema around a brain tumor may be contributing to the headache, and reducing the edema with steroids, mannitol, or other drugs relieves the headache.
“Brain tumor headaches usually do not respond to Imitrex, Amerge, or other migraine drugs.”
What should a person ask himself if he’s afraid he might have a brain tumor?

Shutterstock/B-D-S Piotr Marcinski
The patient should be careful to note any other characteristics of the headache that seem unusual:
- Is the patient prone to headaches, or is this something completely different?
- Is the headache present at certain times every day, such as early in the morning?
- Can the headache be explained by other problems, such as sinus infection or a herniated disk in the neck?
- Are there other symptoms, such as memory loss, dizziness, loss of balance, visual loss, or word-finding difficulty?
- Is there a family history of brain tumors? (only about 5% of BT patients have a family history of brain tumors)
- Is the pain unusual in its location?
- Has the headache persisted over days or weeks? Some brain tumors are so slow-growing that a patient could have a headache for years and still have a brain tumor.
What kind of test should a person insist upon that can rule out a BT?

Freepik.com
“The physician may tell the patient that insurance will not cover a CT or MRI, but if a patient is very concerned, he or she can ask for a referral to a neurologist or headache specialist.
“If the headache becomes very severe, one can always go to an emergency room.
“However, the majority of ER scans are CT scans done without contrast, and some tumors are not detected without contrast.
“A scan done to rule out a brain tumor should be an MRI, which is more sensitive, and should be done with contrast, which will ‘light up’ when there is breakdown of the blood-brain barrier caused by a tumor.”
 Dr. Stark-Vance is a medical oncologist in private practice in Dallas and Fort Worth, providing medical neuro-oncology services to patients of neurosurgical consultants. She received her training in medical oncology at the National Cancer Institute in Bethesda, Maryland. Following her Fellowship, Dr. Stark-Vance served as a clinical investigator at the Cancer Treatment Evaluation Program of NCI. Since her return to Texas in 1996, she has continued developing clinical trials for malignant glioma plus lecture widely on treatment options for primary and metastatic brain tumors. Her work has been published in Journal of Clinical Oncology and Neuro-Oncology.
Dr. Stark-Vance is a medical oncologist in private practice in Dallas and Fort Worth, providing medical neuro-oncology services to patients of neurosurgical consultants. She received her training in medical oncology at the National Cancer Institute in Bethesda, Maryland. Following her Fellowship, Dr. Stark-Vance served as a clinical investigator at the Cancer Treatment Evaluation Program of NCI. Since her return to Texas in 1996, she has continued developing clinical trials for malignant glioma plus lecture widely on treatment options for primary and metastatic brain tumors. Her work has been published in Journal of Clinical Oncology and Neuro-Oncology.
 Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Lump in Throat: Causes and Solutions

Does a lump in your throat, or feeling that something is stuck in your throat, have you frightened it could be ALS or laryngeal cancer?
When a person develops an obsessive fear of ALS, sometimes they fixate on the bulbar-onset version of ALS.
If you clicked on this article, you probably know all about bulbar-onset ALS.
People with the bulbar-onset fear often detect a lump in their throat, or the sensation that something is stuck in their throat, and worry this may be bulbar-onset ALS. In fact, any throat or mouth peculiarity sets them into a panic.
Major Cause for the Throat Lump…
And for the sensation that something is stuck there, is ANXIETY — including anxiety over bulbar-onset ALS.
Anxiety begets the lumpy feeling in the throat.
This is why, in many novels, for example, a character who’s nervous is described as feeling “a lump in her throat.”
Ever notice that nervous people put their hand to their throat? It’s an automatic reaction to that lumpy feeling.
I asked an ear, nose and throat (ENT) doctor just exactly what creates the lump or stuck feeling, that can scare people into thinking they have bulbar-onset ALS or laryngeal cancer.
Other Benign Causes Besides Anxiety
There are others, according to Steven Y. Park, MD, author of the book, “Sleep, Interrupted: A Physician Reveals The #1 Reason Why So Many of Us Are Sick And Tired,” Dr. Park is Clinical Assistant Professor of Otolaryngology at the New York Medical College.
Some people fear laryngeal cancer due to throaty lump sensations or feeling something is stuck there.
But fear of bulbar-onset ALS may be more common, as evidenced by the hundreds of postings on various neurology help sites.
Many of the forum participants express fear of bulbar-onset ALS due to feeling the lump or something stuck in the throat.
Ironically, these forum participants don’t fear laryngeal cancer, even though these sensations are more likely to be laryngeal cancer than bulbar-onset ALS!
But the bigger picture is, these sensations almost always are neither laryngeal cancer nor bulbar-onset ALS, but rather, just plain anxiety and stress.
What causes the lump-in-the-throat feeling?
Dr. Park explains, “This a very common problem that I see almost every day.
“The most common reason for this is due to laryngopharyngeal reflux disease (LPRD), but there can be other reasons such as a foreign body, neurologic conditions and rarely, laryngeal cancer.
“The most common symptoms of LPRD include chronic throat clearing, hoarseness, post-nasal drip, a lump sensation, pain, cough, mucous, burning, tightening or phlegm. You can have one or all of the above.
“The ‘lump’ sensation is called a globus sensation, or a ball-like feeling.
“In our field, we treat LPRD with aggressive PPI therapy (such as Prilosec or Nexium) for 1-3 months, but it only works sometimes.
“One of the main reasons for this high rate of failure is that there’s something else that’s suctioning up your stomach contents into your throat.
“So the acid reflux medications don’t really prevent reflux. They only lower the acidity of the stomach juices.
“You also have bile, digestive enzymes and bacteria that come up and irritate the delicate voice box tissues.”
“A stressed person swallows differently than does a relaxed person.”
The altered swallowing mechanics somehow cause the lumpy feeling in the throat or the sensation that something is stuck in the throat.
How does this happen?
“If you change your swallowing mechanics due to any reason, whether from allergies, post-nasal drip, a scratch from a bone or acid reflux, you will feel pain, discomfort or a foreign body sensation,” says Dr. Park.
“Vigorous rubbing of opposing mucous membranes and cartilages can definitely irritate your throat temporarily.
“This can cause a raw surface on the mucous membranes that takes a few days to heal.
“The cricopharyngeus muscle (the upper esophageal sphincter) can go into spasm and cause a tightening sensation when under stress.
“It’s also been shown that under stress, due to dysfunction of the upper esophageal sphincter, stomach contents can leak up and cause irritation of the throat structure, aggravating the condition.
“If you have microscopic stomach contents in the throat, the mucous secreting glands in this area try to dilute and clear out this area, so you’ll feel mucous, hoarseness and post-nasal drip.
“There will be generalized inflammation in the throat, which can also go up into the nose.”
And there you have it: Why, when you worry about bulbar-onset ALS or laryngeal cancer, you suddenly start feeling scary things going on with your throat!
So relax … and realize that the mind is a very powerful force.
Finally, a very uncommon cause of a lump feeling in the throat is Eagle’s syndrome.
In this condition, a small bone below the skull becomes too long or its ligament hardens.
The resulting nerve irritation can cause a variety of symptoms.
Eagle’s syndrome usually starts later in adulthood due to aging.
SYMPTOMS
- Bad breath despite home treatment
- Breathing difficulty or noise with breathing
- Persistent cough
- Coughing up blood
- Ear fullness or pain despite no infection
- Hoarse voice that persists longer than two weeks
- Loose teeth or dentures suddenly poorly fitting
- Palpable lump in the neck
- Nosebleeds for no reason
- Swallowing pain or difficulty
- Throat pain or soreness
- Throat burning or irritation
- Throat lump sensation like something is stuck
- Changes in voice pitch or volume
- This list is not complete.
 Dr. Park practices integrative medicine and surgery, and has helped thousands of people breathe better and sleep better.
Dr. Park practices integrative medicine and surgery, and has helped thousands of people breathe better and sleep better.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.


































{kind=link}
{kind=link}