
Penis Bumps, Spots and Dots Guide by a Doctor
Here is a DOCTOR’S explanation for the many causes of different bumps, dots and spots on your penis and what can be done about these.
Forget the forums with laypeople’s explanations for why you have tiny red bumps or white bumps or dots or spots on your penis.
You may think that this problem belongs to a urologist, but the penis is covered with skin, and anything that goes on with the skin falls under the specialty of dermatology.
The Many Different Kinds of Bumps, Dots and Spots on the Penis
“Some dots on your penis may be perfectly normal or harmless,” says Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
“Others on the other hand may be sexually transmitted diseases.
“Clear bumps around the penis head are normal for about 10% of men and are nothing to worry about.
“A single hard bump that seems to appear just under the skin could be a harmless cyst that should be excised or drained.
“A cluster of blistery spots, however, may be herpes. These red spots eventually burst and become red and scaly.
“Another infection, syphilis, looks more like a red, painless ulcer.
“Molluscum contagiosum is a viral infection that causes small pearly-colored bumps.
“Genital warts is another viral infection that causes small, rough bumps.”
Deadly Virus
“The HPV (human papilloma virus) causing the genital wart could be dangerous and lead to penile cancer, which can be quite serious,” says Dr. Prystowsky.
“The Gardasil vaccine is intended to help young men and women avoid infection with HPV.
“Also, oral contact with genital warts can lead to life threatening oral/throat cancer from certain bad strains of HPV.
“There are many reasons your penis may have a small bump.
It is important to make sure that if the bumps are infectious, they are treated before being spread to someone else.”

In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

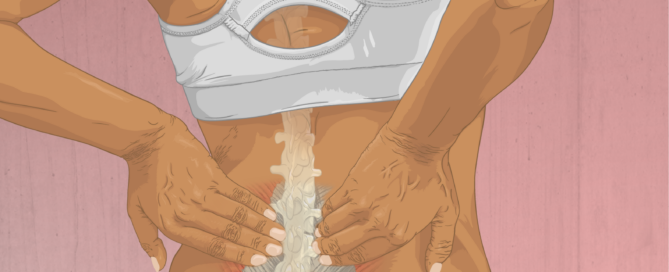
Can Dehydration Alone Cause a Bulging Disc?

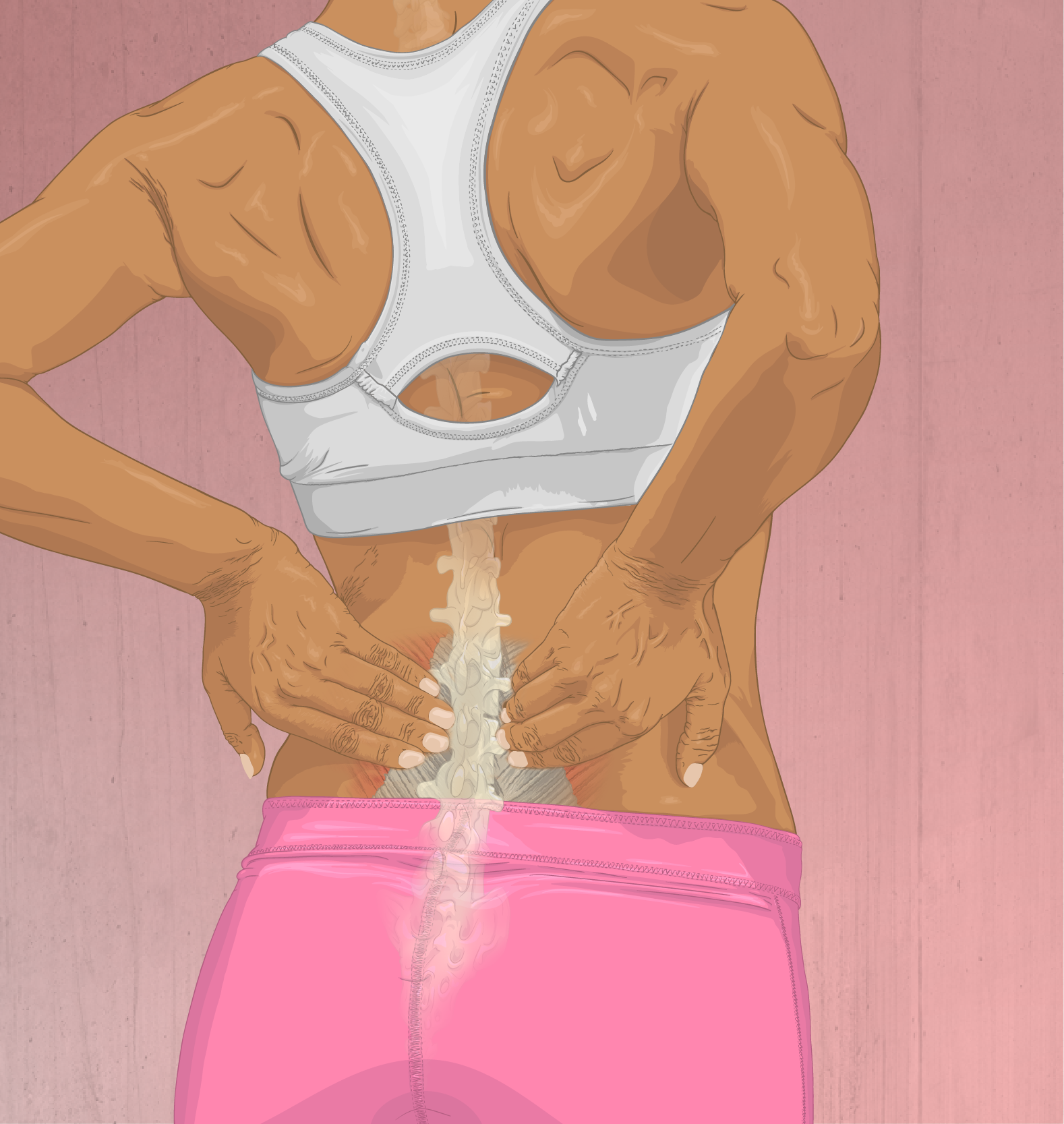
A bulging disc in the lower back can cause low back pain.
Many people drink much less water than they actually believe.
For optimal health and well-being, getting enough water is crucial.
When a disc bulges, this means that the spongy, shock-absorbing tissue that’s between the vertebral bones juts or oozes out of its place.
This can irritate nearby nerves, leading to pain or aching in the low back. The discomfort may radiate down a leg or include tingling.
Not Enough Water
To avoid dehydration, you should not wait until you’re very thirsty.
In fact, dark yellow, and especially orange, urine is an indicator that you’re not adequately hydrated — even if you do not feel thirsty.

Shutterstock/gritsalak karalak
Is there a connection between dehydration and a bulging disc?
“Yes, dehydration can cause a bulging disc,” says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
It’s hard to believe, but true: Not drinking enough water can lead to a bulging disc.
“As most people know, the body is made up of 67 percent water, and some of that water is stored in the spine,” explains Dr. Perry.
He continues: “Our spinal discs are composed of two parts: annulus fibrosus —tough circular exterior composed of collagen fibers, and nucleus pulposus — inter core with a loose network of fibers suspended in a mucoprotein gel.”
The discs are shock absorbers. Dr. Perry explains that “about 75 percent of the pressure applied to the disc is on the nucleus pulposus.
“When the discs become dehydrated, the pressure is no longer on the nucleus pulposus but spreads throughout the entire disc.
“When pressure spreads to the annulus fibrosus, you can get cracks or bulges.
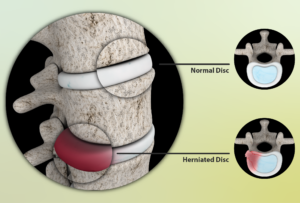
Source: myupchar. com
“This can also create pressure on the nerves and lead to other issues such as leg pain caused by sciatica.”
Dr. Perry adds, “Another interesting thing to note is that when we’re up standing or walking all day, we put enough pressure on our discs that can cause some people to even lose one-forth inch of height between when they wake up and go to bed.
“This is due to pressure and compression causing dehydration of the discs.
“When you lie down at night, the discs have time to extend and intake water. The discs are more likely to expand and the cushion effect becomes more apparent during rest and sleep.”
To make drinking eight to 10, eight-ounce glasses of water every day more feasible, make homemade lemonade, drink tea or add some water to your morning orange juice.
Soda never counts as water. Snack on cucumbers, watermelon and tomatoes, which have a high water content. Drink water with your meals instead of juice, soda or milk.
 Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Miss Ty
Drinking Water for a Bulging Disc for Recovery
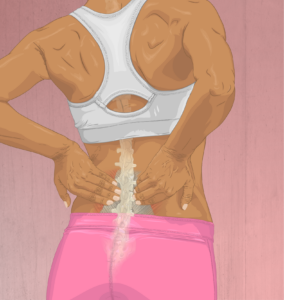
Dr. Michael Perry, MD, says that drinking water is very crucial for recovering from a bulging disc.
A bulging disc also goes by the terms “herniated disc,” “lumbar herniation” and “lumbar pinched nerve.”
“It is important to drink between eight to 10, 10-ounce glasses of water per day to maintain hydration,” says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
“If you’re outside or working in a hot and humid environment, it is important to increase this volume before you start to work.
“It makes a significant difference when you consume more water before you become thirsty; that way your body never becomes dehydrated in the first place.
Why Water Is Important for Treating a Bulging Disc
“Maintaining hydration combined with decreased force on the spine when lying down can help the discs reabsorb some of this additional water,” says Dr. Perry.
“This isn’t proven, but it may help prevent further bulging or even make the existing bulging less significant.”
Consider plentiful daily water intake as part of your conservative treatment for your herniated disc.
How to Fit in Eight Glasses of Water a Day
• Every morning, fill a pitcher with at least 80 ounces of water. Hopefully you already know there are eight ounces in one cup.
• The pitcher will be your supply for the ensuing day and evening.
• Drink only from the pitcher for a very easy way to track your intake.
• Replace soda and sugary juices with the water.
• Make it a point to have a glass first thing in the morning before you do anything else.
• Tea, coffee, soda and alcohol do not count towards your water intake.
• If you can’t drink water unless it’s chilled, and you’re struggling to drink 80 ounces throughout the day, you should try room-temperature water, as the lack of chill should make it go down faster.
• Give this plan some time to work towards improving your bulging disc.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: myupchar. com
Time It Takes for Lifting Weights to Bulge a Disc
“It could take seconds, or it could take years,” for weightlifting to cause a bulging disc, says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
I was inspired to write this article after the fitness director of the health club, where I used to be a personal trainer, walked in one day with a slow, tentative gait. I asked him what was wrong and he said, “I blew out a disc leg pressing.”
Dr. Perry explains, “Typically, anyone who uses their back in any type of physical activity will have generalized wear and tear. With that, the disc and spine will become degenerative over time and that, in itself, can cause a bulging disc.”
In the fitness director’s case, it took seconds: a single, acute event.
Though the floor leg press machine is supposed to stabilize the back (and it does, relative to the instability of the back squat and deadlift), the lower spine can also be subjected to high levels of stress if you’re straining from a very low position to push up a very heavy sled.
If your butt is off the seat at this point, this makes those lumbar discs even more vulnerable.
This is why I recommend that if you’re going to press from a very low position (knees by armpits), to use no more than a moderate amount of weights, e.g., that which you can press for at least eight reps.
Dr. Perry continues, “Chronic condition: A former acute injury to the spine can accelerate the degenerative process. If you have an acute back injury, 10 years down the road you may develop additional pain.
“This isn’t related to new trauma, but related to the injury from 10 years ago. That injury accelerated the degenerative process.
“Acute condition: If you’re a weightlifter, any time you apply pressure to your spine (whether you’re doing deadlifts, squats, bench pressing, etc.), you can herniate [bulge] a disc or cause nerve compression.
“In rare cases, this disc herniation in the lower back can cause cauda equina syndrome – when the nerve roots at the end of the spinal cord are compressed [causing paralysis, numbness, incontinence]. Cauda equina syndrome develops rapidly and is a surgical emergency.”
Does this mean avoid squats, deadlifts and leg presses because lifting weights might cause a bulging disc? Of course not.
Lack of weight-bearing exercise is far more dangerous, because the individual who never strength trains and then one day is helping a friend rearrange some furniture, shoveling snow or just leaning forward to pick up a potted plant…can “throw his back out” and require immediate medical attention.
Or, an extra-long session of housework or yardwork could render a non-strength-trained person in bed all day the next day due to back pain.
When lifting weights, you must use picture-perfect form, and to build strong or big muscles, you do NOT have to gun for the one-rep max.
But even if you do eight reps, you must pay strict attention to textbook form.
I see so many people performing deadlifts and back squats with lousy form; they risk getting a bulging disc.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

MRI vs. CT Scan for Low Back Pain: a Comparison

Low back pain is America’s No. 1 nonfatal health problem. An MRI, but also a CT scan, can tell a doctor a lot about what’s going on in one’s lower back.
The question though, is, which is better for diagnosing low back pain: an MRI or a CT scan?
For sure, from the patient’s point of view, the MRI sounds a lot better because it doesn’t emit the radiation that a CT scan does.
On the other hand, those with claustrophobia would rather undergo the CT scan than be “inside a tube.”
Patients who don’t want to feel trapped inside a tube can also inquire about the possibility of an “open” MRI.
An open MRI has wide sides and open space around the body, not a tight tunnel, allowing more visibility and airflow.
Low Back Pain: MRI vs. CT Scan
“The best test to obtain when looking at the spine is an MRI” rather than the CT scan, says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
“These scans are the best for soft tissues, such as your spinal nerves, disc, cord and ligaments,” continues Dr. Perry. “An MRI will allow your doctor to see cord and nerve compression.”
That’s not the greatest news to those who fear enclosed spaces and don’t care about radiation.
But it’s really good news because you should be concerned about radiation, and the MRI is truly superior at imaging the causes of low back pain.
So if you’re scared of being inside a tube, remind yourself that the MRI equipment does not emit radiation, and the CT scanner does.
“When you may have a bone issue, such as a hairline fracture, spurring or arthritis, a CT scan is the best test to obtain,” says Dr. Perry.
“A CT scan is preferable if you have a pacemaker, defibrillator or morphine pump. When you have one of these implanted devices, an MRI scan is contraindicated because of the MRI’s ability to interfere with the functions of these devices.”
If you’re scheduled for an MRI due so low back pain, bring good earplugs with you, as this machine produces loud knocking noises throughout the procedure.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Can Prolonged Sitting on the Toilet Cause Sciatica?

Yes, sitting a long on the toilet and reading can cause sciatica, says a spine doctor.
It may seem benign — sitting on the toilet for extended periods and reading, talking on the phone, texting, what-have-you — but this can lead to sciatica, says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
In sciatica, the sciatic nerve is irritated. One cause of irritation is pressure against the nerve.
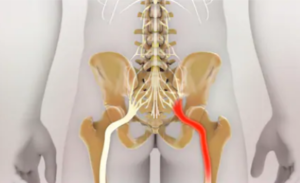
Sciatic nerve. Shutterstock/Nathan Devery
This can easily be caused by extended time sitting on a toilet, especially if the seat is hard — which it typically is.
The leaned-forward position that most people assume adds even more pressure on this major nerve.
Have you ever developed a numbness and tingling along your hamstring group after sitting on a toilet for a while? That’s the sciatic nerve being imposed upon.
“When you are sitting down, whether it is on a toilet or in a chair, you are applying more pressure to your discs than when in any other position,” says Dr. Perry.
“Some people tend to pull out a newspaper or a magazine while leaning forward on the hard toilet seat for an extended period of time.
“If that person also has an underlying disc abnormality, this significant and extended pressure can cause further deterioration.
“You may begin to experience shooting pain, electrical shocking pain or numbness because of this increased pressure while sitting in this position.
“If someone has a disc abnormality and they do feel this pressure and increased sciatica symptoms, it should be treated.
They should remain cautious and alert of sitting on the toilet for an extended period of time.”
If you cannot help but spend a lengthy amount of time on the toilet due to a major bowel movement or constipation, then try your best to periodically lift the affected leg off the seat to help relieve some of the pressure on the sciatic nerve.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Viacheslav Nikolaenko

Can Excessive Walking Cause Knee Bursitis?

If you already have bursitis in your knee, then it stands to reason that excessive walking will make you aware of it.
But this doesn’t mean that a lot of walking actually causes bursitis in the knee.
We live in a society that’s so sedentary that a lot of walking is viewed as something potentially harmful, when in fact, lots of walking is exactly how the human species survived and flourished. The problem is all the sitting that we do.
But let’s get back to bursitis of the knee. Something causes this when people have it.
Bursitis doesn’t just happen. A bursa is a fluid-filled sac (it’s supposed to be filled with fluid).
“The knee joint contains several bursae, which can be grouped by location into the medial, lateral and frontal bursae,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
Medial means inner; lateral means outer; and frontal means front.
“There are five medial bursae, four lateral and five frontal bursae,” continues Dr. Peck.
Causes of Bursitis in the Knee
“The most commonly-affected by inflammation leading to bursitis are the suprapatellar and pes anserine bursae. Pes anserine bursitis results from overuse and is common in runners.”
Now you might be thinking, if bursitis is common in runners, why wouldn’t a lot of walking be a cause?
This is because when we do a lot of walking, it tends to be for the sake of either transportation (such as a lot of walking on the job) or non-hard-impact exercise (fitness walking).

When bursitis is caused by running, it’s because the patient has been running way beyond that required for transportation or general fitness.
In other words, the patient has likely been training for long-distance running events or breaking personal record sprint times over short distances, which may include hurdling.
The patient may also have been running only in the name of fitness, but logging five miles at a grueling pace on hard concrete every single day. That’s still a lot of running.
This kind of running is not what ancient hunter-gatherers did for survival.
Sure, they jogged, but it was for transportation over natural terrain, not marathon training on an asphalt street.
Sure, they sprinted, but only to catch their dinner or escape from danger, rather than over and over and over on an asphalt surface every day to break personal record times.
Bursitis in the knee isn’t always caused by running, but if you’ve been diagnosed with it, it’s extremely unlikely it was caused by walking.
Dr. Peck also says, “It may lead to pain and a discrete area of tenderness over the medial tibial condyle, the bony protuberance on the inner aspect of the lower knee.”
 Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: depositphotos.com
Why Does Hip Replacement Cause Sore Thigh Muscles?

Have you noticed that the muscles in your thigh are persistently sore only since your hip replacement surgery?
There is a gait abnormality that can cause this problem, says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
It is called Trendelenburg gait, and it is characterized by weakness in the patient’s hip abductor muscles.
The hip abductor muscles enable you to move your upper legs away from the midline of your body (“abduct” means to move away from).
Think of the “hip abduction” equipment at the gym. You sit in it and abduct your hips to move your thighs away from each other.
So these muscles, then, are weak in someone with osteoarthritis of the hip joint.
“After hip replacement, retraining of the muscles of the thigh is necessary, but may result in soreness,” says Dr. Peck.
“In addition, soreness can be a result of simple post-operative pain, as the muscles of the lateral thigh are generally retracted for access to the joint for surgery.”
If the soreness in your thigh muscles persists, however, you’ll want to strengthen the hip abductors—which actually are located mostly in your butt, but may seem like they are “upper leg muscles.”
However, one of them, the vastus lateralis, is located along the side of the thigh.
Lying on the floor, on your side, and lifting a straightened leg up and down, with the inner part of your foot parallel to the floor, will engage the hip abductor muscles.
So will the equipment at the gym mentioned previously.
When using this equipment, it’s more effective to use a moderate amount of weight that allows you to abduct as much as you can, rather than a ton of weight that limits your range of motion.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Shaynepplstockphoto

Stabbing Sharp Knee Pain ONLY when You Walk?

“A meniscal tear, either medial or lateral, can result in sharp [knee] pain with walking,” among other possible causes, explains Devin B. Peck, MD, of owner of Austin Interventional Pain in Austin, TX.
The meniscus is cartilage (a shock absorber).
Dr. Peck continues, “While there can be pain at rest, it is less common, and if present would typically worsen with walking.
“There may also be a sensation of ‘catching’ in the knee with extension, especially if a small piece of the meniscus has separated from the main portion (a ‘free fragment’).”
Knee extension is when you straighten out your lower leg from a bent position.
“There may be difficulty straightening the knee all the way, and it may feel unstable with walking,” says Dr. Peck.
“Degenerative joint disease – or osteoarthritis – of the knee can also present with pain only with walking,” though it won’t necessarily be what you’d describe as stabbing or sharp.
However, bone-on-bone contact from severe osteoarthritis is certainly no picnic, either.
“Weight-bearing leads to more axial stress on the knee joint, and repetitive motion leads to wear-and-tear stress on the joint.
“There can be swelling, decreased range-of-motion or even joint deformity.
“These deformities are often either valgus deformities, in which the joint deviates inward (knock-knee), or varus, in which the joint deviates outward (bow-legged).”
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Sharp, Shooting Knee Pain only when Sleeping

Can sharp knee pain only when sleeping be caused by cancer?
“Pes anserine bursitis is inflammation of the bursa or sac of lubricating fluid located on the inner aspect of the lower knee,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
What can cause really bad pain in the knee only when sleeping?
Dr. Peck explains, “When sleeping on your side, you can experience pain from this source if the knees lay atop each other, putting pressure on this bursa.
“In fact, this type of bursitis can present as pain only with sleeping or lying down.”
Place a pillow between the knees and legs when you’re sleeping on your side and see if that helps.
“Knee pain that awakens you from sleep can indicate degenerative arthritis,” says Dr. Peck.
What about cancer?
“Joint pain is very rarely the presenting symptom of cancer,” says Dr. Peck.
“With bone tumors, there will commonly be associated symptoms such as weight loss, fatigue or other symptoms, and pain will typically be progressively worse over time.”
If you have pain in your knee that seems to occur only overnight, awakening you from sleep, chances are very unlikely that this is cancer.
“Most osteosarcomas occur in children and young adults,” says the American Cancer Society’s website.
“Teens are the most commonly affected age group, but osteosarcoma can occur at any age.”
Also, if this tumor is causing someone pain in the knee at night or awakening them from sleep, it’s also causing pain during the day.
This article is really about pain in the knee only when sleeping.
Another possible cause is chondromalacia patella or femoral patellar syndrome, a problem that involves the kneecap.
Risk factors for this are running, jogging and jumping.
This is probably also causing you some discomfort during the day but is not quite on the radar, but once the knee becomes still while you’ve been sleeping for a while, things just stiffen up.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}