

Really Dry Skin Around Eyes: Causes & Solutions

Dry skin around the eyes is a common problem.
It is not always corrected by simply dabbing on skin lotion or moisturizers.
“Dry skin of the eyelids is frequently referred to as blepharitis (which just means inflammation of the eyelid),” says Dr. Dendy Engelman, a board certified dermatologic surgeon with Manhattan Dermatology & Cosmetic Surgery.
Causes of Dry Skin Around the Eyes
Dr. Engelman explains, “The potential causes of blepharitis are many: allergic contact dermatitis, seborrheic dermatitis, irritant dermatitis, so treatment needs to be catered according to the cause.”
Dermatitis (contact and irritant)
• Keep track of anything that can possibly come in contact with the skin under your eyes throughout the day.
• You’d be surprised at what can end up there that you’d never think of.
• This includes household cleaning agents that are on your fingers — that get transferred to the skin beneath your eyes.
• Other possible culprits are pet dander, cosmetics, hair care products, fragrances and chemicals from the workplace.
• Once you’ve figured out what comes in contact with that area, eliminate them as best you can and see what happens.
Seborrheic Dermatitis
- This common problem involves the sebaceous glands. Not only is dry skin a symptom, but often, the skin flakes, itches and appears as a pinkish patch (sometimes with a tinge of dull orange).
- Do not scratch or rub the affected area no matter how badly it itches.
- Your doctor can prescribe an ointment to rid the problem.
Dr. Engelman continues, “Eye irritation can also be a symptom of ocular rosacea, a subtype of the disorder [rosacea] that can potentially be very serious if allowed to become severe.
“Once a medical cause has been ruled out, a nice OTC option to try to mitigate dryness around the eyes are Ocusoft lid scrubs.
“I recommend patients use these twice daily to help cleanse the delicate eye area.”
 Versed in the latest techniques and technologies, Dr. Engelman provides a wide range of services including fat removal, mole excision, Mohs surgery and skin cancer treatment.
Versed in the latest techniques and technologies, Dr. Engelman provides a wide range of services including fat removal, mole excision, Mohs surgery and skin cancer treatment.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, bearfotos

Get Rid of Seborrheic Dermatitis with Selsun Blue

Getting rid of seborrheic dermatitis is easier than you think with Selsun Blue.
Selsun Blue’s active ingredient is one percent selenium sulfide. Selsun Blue is a popular dandruff shampoo, and any similar shampoo with this active ingredient should be just as effective at treating seborrheic dermatitis.
I was diagnosed with seborrheic dermatitis some years ago. My doctor told me to just put Selsun Blue on the patches, then rinse.
I wonder how many people, who struggle with seborrheic dermatitis, have tried Selsun Blue or another shampoo with the one percent selenium sulfide. Maybe I’m an exception, but the stuff works like a charm.
I put my index finger to the bottle’s opening and tip it, getting a good gob on my finger. I then smear the shampoo on my skin, giving it a thick coat.
This is primarily on the sides of my nose, including where the nose has a crease.
It’s also on the front lower part of my nose, and sometimes on my forehead, between but above my eyebrows.
There’ve been times when the seborrheic dermatitis appeared below my eyebrows, and I dabbed the shampoo there as well.
There’s no reason to wait any length of time before rinsing. After you apply the shampoo, just rinse with water.
Any residue can be wiped away with a few Q-tip swabs held together. There’s no need to rub. Be gentle.
A wet sponge will also work on flatter areas. I’ll dab with the sponge on the front of my nose and on my forehead.
I’ll then splash water on my face. Residue is removed with the Q-tips.
I’ve noticed an improvent within 24 hours, and a complete elimination in about three days or less.
However, what typically happens is that I get lazy and stop applying the Selsun Blue.
Invariably, the seborrheic dermatitis returns. Sometimes I’ll let it go several days, but it isn’t long before I’m forced to apply the shampoo again.
If I applied the Selsun Blue every day, or maybe even every other day, this would prevent flare-ups of the seborrheic dermatitis.
But let’s face it: It’s a drudgery to have to do this every single day or even every other day.
Sometimes I forget. Sometimes I remember and just decide to skip it, because I know that when the seborrheic dermatitis flares up again, I could make it disappear within three days by just putting the shampoo on it.
The reason the active ingredient in this shampoo is so effective is because the process that leads to seborrheic dermatitis is the same process that leads to scalp itchiness and dandruff — that’s what my doctor told me.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

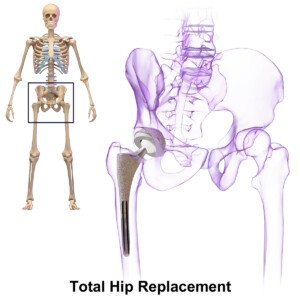
Regional vs. General Anesthesia for Hip Fracture Surgery

If you need hip fracture surgery (or replacement), you’re better off requesting regional anesthesia rather than general.
Many people don’t know that hip surgery can be performed with only regional anesthesia, and instead automatically assume that the patient must be “completely knocked out” in order to have this procedure. Not true at all.
My father had hip replacement surgery a few years ago and it seemed that anything less than general anesthesia was out of the question.
However, a study from the Perelman School of Medicine at the University of Pennsylvania concludes that regional presents a substantial reduction in mortality as well as pulmonary complications.
Twenty percent of hip fracture patients die within one year of injury, says Mark D. Neuman, MD, assistant professor of anesthesiology and critical care, and the study’s lead author.
The paper notes how common hip fractures are: 1.6 million a year worldwide, with most occurring in people over age 65. After age 80, mortality spikes.
Regional anesthesia may include epidural, spinal or a nerve block, while general has the patient unconscious; their nervous system is considerably depressed, such that they can’t even breathe on their own and must be intubated.
In this study, the patients who had hip fracture surgery with regional anesthesia had a 29 percent lower adjusted odds for mortality when compared to general anesthesia.
As for the decrease in adjusted odds for inpatient pulmonary complications, it was 24 percent with regional vs. general.
Being that hip fracture is such a global burden, these study results are not to be ignored.
These findings “highlight an important potential opportunity to improve outcomes among a growing population of vulnerable surgical patients,” says Lee A. Fleisher, MD, chair and Robert Dunning Dripps professor of anesthesiology and critical care.
BruceBlaus
If you’re concerned about breaking your hip bone when you’re “old,” there are things you can do to dramatically lower the chances of this happening.
If you don’t lift weights, then start.

Freepik.com
Strength training will strengthen bone by forcing muscles to pull against bone to generate joint action.
This stresses the bones and makes them adapt by becoming denser. Denser bones are less likely to break.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2012/06/120620100827.htm

Is Physical Rehab for a Herniated Disc Supposed to Hurt?

How can a patient do physical therapy for a herniated disc if it hurts too much to exercise?
What if you have a herniated disc and find that the physical therapy exercises are impossible to do because you can’t get into the position without a lot of pain? Should you just grin and bear it?
Or does the pain mean that the exercise is actually making things worse for the disc?
First off, you certainly do not want to hastily make the decision to undergo surgery just so that you can avoid physical therapy.
People who have surgery to repair a herniated disc will still be required to stick to a physical therapy program.
And surgery is never a picnic.
How to Deal with the Pain of Physical Therapy for a Herniated Disc
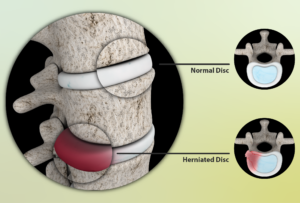
Source: myupchar. com
“Physical therapy is employed to diminish pain and suffering,” says Kenneth K. Hansraj, MD, who specializes in minimally invasive spine surgery, laminectomies and spinal fusions, and is author of the book, “Keys to an Amazing Life: Secrets of the Cervical Spine.”
“Unfortunately, especially in the phases of pain, just touching the involved spinal area may lead to further pain and tenderness.
“I encourage my clients to stay with the therapy at this point, since the therapy will lead to diminished inflammation and restoration of function along with further tolerance of therapy.”
In other words, before progress is to be felt, the patient may have to endure some inconvenience.
Pain does not always mean that something is getting injured or made worse.
In this case it would mean that the physical therapy is involving the compromised structures — and of course there will be some hurting. But stick it out; give it a chance.
In addition to the physical therapy for your disc herniation, you can implement the use of heat packs and stretching exercises to combat pain. Below are a few stretching exercises.



Freepik.com
 Dr. Hansraj is an orthopedic surgeon in Poughkeepsie, NY, and is affiliated with St. Francis Hospital-Roslyn. He received his medical degree from Drexel University College of Medicine and has been in practice for 20+ years.
Dr. Hansraj is an orthopedic surgeon in Poughkeepsie, NY, and is affiliated with St. Francis Hospital-Roslyn. He received his medical degree from Drexel University College of Medicine and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/yanalya

Improve Your Blood Sugars by Tweaking Carb Intake

There are several ways to improve your blood sugar levels (glucose metabolism) by making changes to your carbohydrate intake.
You may have increased awareness of glucose metabolism in an effort to prevent type 2 diabetes or even prediabetes.
And not all type 2 diabetics are overweight, by the way — even though obesity is a major risk factor.
“People without diabetes will metabolize most any form of glucose without any problem,” begins Julie Cunningham, MPH, RD, LDN, registered dietitian and certified diabetes educator.
“As some people get older and heavier, they may develop prediabetes, which is essentially a condition in which the body has trouble metabolizing glucose quickly,” continues Cunningham.
“This can be improved by eating complex carbohydrates, such as whole grains, beans, fruits and vegetables, rather than simple carbohydrates, such as white bread, pastries, candy and sweetened beverages.
“Complex carbs are digested more slowly and create less of a spike in blood sugar levels.”
That’s your general way to help control blood sugar — whether you have diabetes or not.
But there are some more refined and clever tricks you can employ to manage and improve your blood sugar levels.
Changes You Can Make with Carbohydrate Intake to Help Improve Blood Sugar
- Limit carb servings to 60 mg or less per meal or snack.
- Eat protein with your highest carb servings, and ideally, with other carb servings such as fruit plates. E.g., deviled eggs with your dish of fruit or fig newtons.
- Don’t eat carbs close to bedtime — or at least, have only a small amount or under 20 g such as a medium apple.
- Be strategic with when you eat carbs. E.g., eat your daily apple or banana right before your step class, chest workout or treadmill run. Have another one of your daily fruit servings in the middle of a weight workout.
- At the conclusion of any workout, have another piece of fruit before your post-workout meal.
- Have your biggest carb serving of the day (pasta, rice, potatoes, etc.) within one hour of your strength training workouts.
- If you decide to indulge in a very quick-acting carb like a large glass of juice, or a helping of apple pie, a bowl of ice cream or fresh baked chocolate chip cookies, coordinate this so that it’s within one hour (ideally 30 minutes) of a strenuous workout, when glucose metabolism is most efficient.
- Space out your carb feedings. If you normally eat four servings of fruit at once, divide this into a separate four servings to be eaten once every 45-60 minutes.
- Limit juice; eat more whole fruit. Increase fiber intake.
- Replace white bread and white rice with whole grain and brown/wild/basmati, respectively.
- Limit processed foods (e.g., granola bars, some cereals, frozen dinners), which are full of quick-acting carbohydrates. Of course, for most people concerned about blood sugar, it’ll be impossible to eliminate altogether favorite processed foods. But DO make an honest effort to cut back.
How to Monitor Your Blood Sugar Levels

Shutterstock/Maya Kruchankova
To check if your glucose metabolism has improved – or at least if it’s normal — buy a home blood sugar test kit from the local drug store.
But don’t become obsessed with frequently checking your blood sugar, as this can become as obsessive as checking your body weight.
 Julie Cunningham specializes in helping men and women with diabetes and prediabetes learn how to eat to manage their blood sugars–so they can get back to the things they enjoy.
Julie Cunningham specializes in helping men and women with diabetes and prediabetes learn how to eat to manage their blood sugars–so they can get back to the things they enjoy.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lean Fit People Who Exercise Can Get Insulin Resistance

It’s alarming but true that lean fit people who exercise can develop insulin resistance.
You’ve most likely heard of insulin resistance, and it seems that every article about insulin resistance contains the words overweight, obese, lack of exercise, inactive and poor diet (or something similar).
Read enough articles on insulin resistance and you’ll soon be convinced that only overweight (especially obese) people who never exercise get this prediabetic condition.
If you’re a lean, physically fit athlete, and especially if your diet restricts processed foods, trans fats, sat fats, white sugar and high fructose corn syrup, it will be very easy to believe that you can never, ever develop insulin resistance.
The body relies upon glucose for energy—not just the energy needed to play sports or pump iron, but the energy required on the cellular level: cellular metabolism.
When you eat carbohydrates (in the form of sugar or starch), they enter the bloodstream and raise blood sugar levels. In response, the pancreas secretes the hormone insulin.
There are insulin receptor sites on the surface of cells (e.g., muscle and liver cells).
The insulin binds to these receptors, causing uptake of the glucose by the cells from the bloodstream.
The glucose will be used as energy for cellular metabolism, or stored as glycogen in the liver for later use.
But what if these insulin receptors aren’t up to this task?
This is insulin resistance, according to Dr. David Edelson, MD, board certified in internal and bariatric medicine, one of the top obesity experts in the U.S., and founder and medical director for HealthBridge.
The receptors “seem to ignore the insulin, or require higher levels before they will respond,” he says. And what if there’s a short supply of these receptor sites? That, too, is insulin resistance.
Because the cells are not taking up the glucose the way they should, the pancreas may end up pumping out even more insulin, thus stressing this gland. In the early phases of insulin resistance, says Dr. Edelson, this will result in too much insulin in the blood (hyperinsulinemia).
Over time, this can cause “fatigue, fat gain around the midsection and eventually full-blown metabolic syndrome, but in the beginning there may be no noticeable symptoms,” says Dr. Edelson.“After a while, the pancreas can’t keep up.”
The result is that blood sugar levels remain elevated. Left untreated, there is a 30 percent chance that insulin resistance will morph into type 2 diabetes. IR also raises the risk of heart disease, stroke and kidney damage.
If you’re a mean, lean and buff iron-pumping machine, and have a plant-based, mostly whole-foods organic diet, “You can still develop insulin resistance at some time in your life,” says Dr. Edelson.
However, it’s crucial to remember that remaining lean and fit through a healthful diet and rigorous exercise will substantially lower the odds of developing insulin resistance.
To learn what a lean, fit athlete or gym enthusiast with a clean diet can do to absolutely minimize the chance of getting insulin resistance, go to Part II of this article for Dr. Edelson’s recommendations.

Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/vladee

What Can Lean, Fit People Do to Prevent Insulin Resistance?

David Edelson, MD, says that even lean, fit athletes can develop insulin resistance but there are ways to help prevent it.
First of all, examine your sleeping habits. Spiegel et al, found that “In laboratory studies of healthy young adults submitted to recurrent partial sleep restriction, marked alterations in glucose metabolism including decreased glucose tolerance and insulin sensitivity have been demonstrated.” (Journal of Applied Physiology)
If you find this shocking, the June 2010 Journal of Clinical Endocrinology and Metabolism published a report titled:
“A Single Night of Partial Sleep Deprivation Induces Insulin Resistance in Multiple Metabolic Pathways in Healthy Subjects.”
This title was the exact conclusion of the study’s authors, Donga et al.
If your fasting glucose reading is between 100 and 125 mg/dL (which in and of itself does not qualify for a diagnosis of insulin resistance, but it’s something to take notice of), or, you have been diagnosed with IR, perhaps it’s due to disrupted sleep. (A normal fasting glucose is 60-99 mg/dL.)
Insulin resistance in lean people who rigorously exercise can also result, in part, from a genetic predisposition, says Dr. Edelson.
He is board certified in internal and bariatric medicine, and one of the top obesity experts in the U.S., and founder and medical director for HealthBridge.
Dr. Edelson explains, “IR is a genetic trait that you either have or do not have.”
Insulin resistance is classically triggered by one or more lifestyle factors (e.g., a diet high in processed sugars, starches, high fructose corn syrup, trans fats, low in omega-3s, plus lack of exercise, poor sleep and excess belly fat).
But there’s more. A vitamin D3 deficiency can lead to insulin resistance.
The D3 deficiency can be caused by a number of factors, including inadequate dietary intake, lack of sunlight exposure, and inflammatory bowel disease.
Studies support the correlation between inadequate D3 and IR (e.g., Chiu et al, American Journal of Clinical Nutrition, 2004).
How a Lean, Fit Person Can Reverse and Help Prevent Insulin Resistance

Shutterstock/BLACKDAY
Dr. Edelson says that the lean, fit athlete who already has insulin resistance can take the following supplements to reverse the condition, to “more naturally turn back on the insulin receptor site so it will respond better to insulin in the bloodstream,” he says.
• Fish oil. This is a potent tool for reversing, and preventing, insulin resistance.
Suggested daily dose for mild to moderate IR: 1,500-2,500 mg. Adding wild Alaskan salmon to the diet will also help.
• Cinnamon. Though studies on humans are limited, studies on animals suggest that this spice may be a heavyweight in the reversal of insulin resistance.
Sprinkle it on fish, chicken, grass fed beef, wild game, apples, and add a touch to your protein shakes.
• Chromium picolinate (“chrome-pic”). This mineral was reported in Diabetes Education (2004) to be highly effective against IR.
The report states: “Chromium picolinate, specifically, has been shown to reduce insulin resistance and to help reduce the risk of cardiovascular disease and type 2 diabetes.
Supplements containing 200-1,000 mcg chromium as chromium picolinate a day have been found to improve blood glucose control.”
The report adds that chrome-pic supplements are safe.
What about claims that supplementation with niacin (vitamin B3) can improve glucose metabolism?
Dr. Edelson explains, “There has been some concern that niacin may actually worsen IR. It has long been known that niacin can raise fasting glucose levels.
“Recent articles seem to indicate that this effect is due to niacin provoking IR.
“As such it is even possible that niacin supplementation in food items such as breakfast cereals may actually be worsening the obesity crisis.
“A recent article in the World Journal of Gastroenterology points to this effect.”
Additionally, there are other measures that the trim athletic individual with insulin resistance can take.
According to Kristine Gedroic, MD, who specializes in integrative medicine in Morristown, NJ, diet should be re-evaluated, even though the patient may think he or she has a very healthful regimen.
“Many complex carbohydrates are less than ideal,” says Dr. Gedroic.
“For those with true IR, I advise only carbohydrates that are cooked in a pan or from nature, i.e., steel cut oats, brown rice, quinoa, millet and potatoes.
“No flour products of any kind until the insulin resistance reverses.
“Sugar substitutes must also be removed from the diet (though Stevia, which is natural, is acceptable), along with chewing gum, which can activate digestive function artificially.
“After those basic interventions are made, this type of patient often needs a comprehensive endocrine assessment.
“Many times when the pancreas has been stressed producing insulin for whatever reason, the liver, adrenals and possibly thyroid gland may be suboptimal too.”
The key is prevention of insulin resistance, and lean, physically fit people who believe they have a clean diet are not exempt from being aware of this prediabetic condition.
Dr. Edelson is widely recognized as one of the nation’s top weight loss experts, and was listed in NY Magazine’s “Best Doctors of 2014” issue.
 Dr. Gedroic has spent 10+ years recovering thousands of patients with chronic illness. While most medical doctors prescribe a medication in response to symptoms, Dr. Gedroic strives to understand the root cause of an illness for a customized treatment plan.
Dr. Gedroic has spent 10+ years recovering thousands of patients with chronic illness. While most medical doctors prescribe a medication in response to symptoms, Dr. Gedroic strives to understand the root cause of an illness for a customized treatment plan.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/FXQuadro
Burn Fat with the Squat to Lunge Workout!
Here are easy instructions for the squat to lunge workout which will burn fat off your thighs, belly and all over your body. Video follows.
The squat to lunge workout is exactly what the name says: squat, then go into a lunge.
This can be done from end to end in an empty basketball court, or from end to end in an empty fitness class studio, or from one point to another on the gym floor.
Use a fixed weight barbell, as these are smaller than Olympic bars and less cumbersome.
This routine is not for beginners or people who are not proficient with the back squat form.
Stand with feet at least shoulder width apart or whatever your preferred stance is for the back squat. To start the exercise, perform a half squat.
After rising to the start position, step forward with one foot into a lunge stance, perform a lunge, rise, then bring the back foot up to flush with the forward foot.
Next, step forward with the other foot now, into a lunge, lower accordingly, rise, and then bring that foot flush — except instead of the feet being close together like they typically are after completing each lunge during walking lunges, after that second foot completes the sequence, it comes up to create the foot-to-foot distance that you’d use for the back squat. At this point, you squat.
Summary: Then the cycle begins all over. So it’s as follows:
· Squat
· Return to start position
· Lunge with right foot
· Bring left foot to flush with right foot
· Lunge with left foot
· Bring right foot flush but at least shoulder width from left foot
· Squat
Ideally, a person should be able to execute smooth movement so that motion is fluid rather than robotic with the lunge portion.
Once you can execute the sequence with confidence, it’s time to get a barbell across the upper back.
How much the barbell should weigh is not something you’ll likely be able to figure out on the first try.
Let’s suppose someone starts with a 50 pound barbell. This may seem light to an individual who squats reps with 185. But the walking lunge really changes things.
Furthermore, one must get used to walking lunges with a barbell across their back; many who do walking lunges with weights use only dumbbells held with straight arms at the sides.
With the barbell, execute the aforementioned sequence. Don’t be surprised if you become fatigued very quickly. Intense fatigue is important for burning fat.
Squats should be at least parallel (half squat), and lunges should be deep. The more it “hurts,” the more fat you’ll burn.
Make sure you don’t “good morning” the squatting portions; keep good form and an upright back.
Burn More Fat by Increasing Intensity
Use a heavier barbell as you get better at this exercise. You should be able to sustain this movement for at least one minute before having to stop.
Longer than two minutes means that the emphasis is shifted towards endurance.
Another way to increase intensity is to perform the squat after every single stride.
And yet a third intensity technique is to perform this fat burning routine backwards.
It’s best to do the backwards version in a fitness studio so you can watch in a mirror.
Do this routine twice a week to increase your body’s ability to burn fat.
Remember, staying in your comfort zone will not burn fat. This exercise will promote fat burning through the entire body.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Acid Reflux – Increases Cancer Risk, Can Affect Throat
Acid reflux is a very common problem and can cause a number of symptoms, but the most common is “heartburn.”
“Acid reflux is a common condition which produces heartburn and chest pains,” says Natasha Fuksina, MD, an internal medicine and obesity specialist who combines traditional, integrative and functional medicine to restore health and function.
“It affects more men than woman and is associated with advancing age, smoking and obesity.”
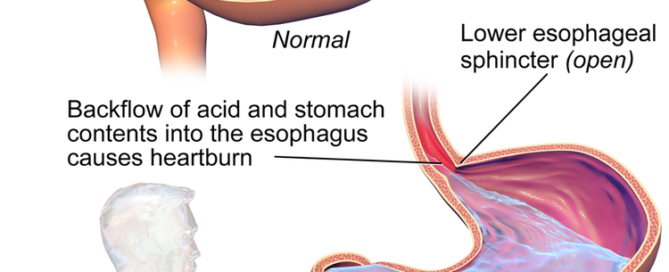
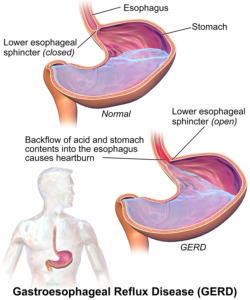
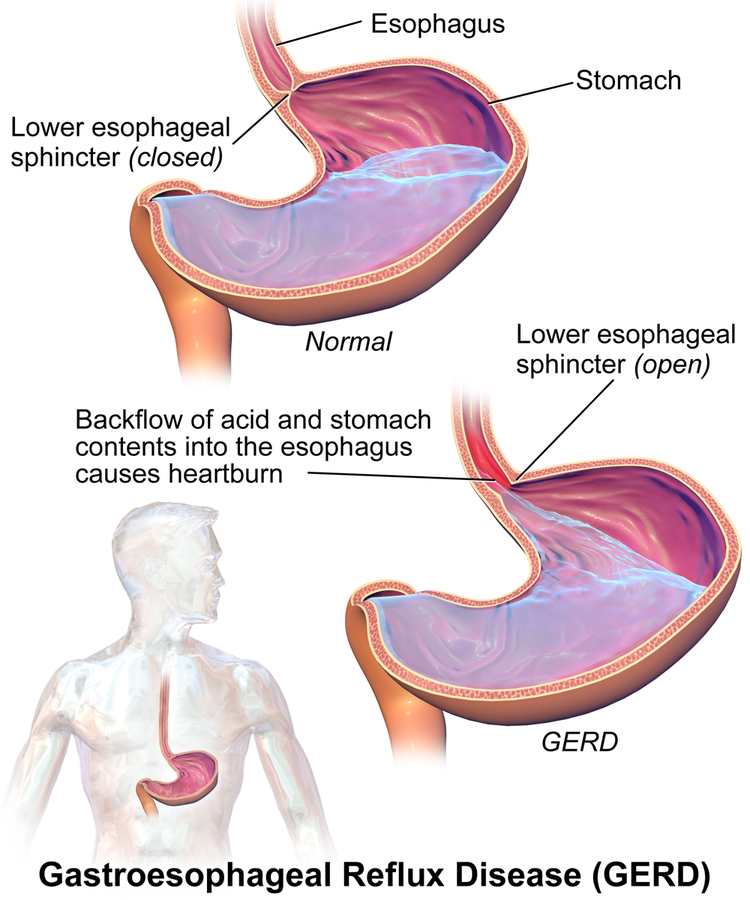
Reflux can ocur due to increased acid production and/or a weak esophageal sphincter muscle that doesn’t close properly, allowing acid to go up the esophagus.
“Rare but feared complication of acid reflux is esophageal cancer (adenocarcinoma) and its precursor, Barrett’s esophagus,” says Dr. Fuksina.
Barrett’s esophagus may result from untreated chronic acid reflux.
This is why you should never blow off the situation with “Oh, it’s just acid reflux.”
Dr. Fuksina explains, “With longstanding damage from acid reflux, the lining of the esophagus — normally consisting of flat squamous cells — can transform into columnar cells — leading to a precancerous condition (Barrett’s esophagus) and possibly esophageal cancer.”
TV commercials for heartburn are typically of a comical nature. This creates the illusion that cancer is nowhere downstream from this common condition.
But once a person develops Barrett’s esophagus, they must receive lifelong surveillance of the interior of their esophagus to catch any abnormal changes in time before they transform into a malignancy.
About one to two percent of cases of Barrett’s turn into esophageal cancer — which has a poor prognosis.
Chronic acid reflux that affects the throat is a risk factor for laryngeal cancer, though that risk is small as well.
Acid reflux that affects the throat on a chronic basis is called LPR: laryngopharyngeal reflux disease.
Symptoms include cough, a hoarse voice, a sore or burning throat, a sensation of a lump in the throat and an unpleasant taste in the mouth.
Not Always a Burning Sensation
However, the discomfort of chronic acid reflux, also known as gastroesophageal reflux disease (GERD), isn’t always a burning sensation.
It can also be described as “pain” by some sufferers — and very bad pain in the chest that can make a person think they’re having a heart attack.
When the throat is affected, this doesn’t mean that there are chest symptoms; sometimes the only symptoms are throat related.
Despite the absence of chest symptoms, however, there may still be acidic contents in the esophagus.
“Treatment includes dietary modifications, weight loss strategies and medications aiming to suppress acid production,” says Dr. Fuksina.
Here are numerous articles about acid reflux — you’ll probably find exactly what you are looking for.
 Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus

Chest Pain: Heart Problem, Indigestion or Pulled Muscle?

Chest pain is the No. 1 reason people head to the emergency room.
But does this mean that most of the diagnoses for these patients relate to a heart problem?
Believe it or not, most are not related to heart disease. Chest pain has common causes that are not related to the heart.
But to play safe, people with unexplained and persisting chest pain, or chest pain upon exertion, should get a prompt evaluation.
Unfortunately, many people who experience this unnerving symptom don’t bother visiting the ER, figuring that it’s a little indigestion and that “it will pass.”
And often, a heart related problem that causes chest pain will, indeed, pass, tricking the person into thinking it was nothing serious.
Chest pain, aching and soreness have quite a few causes; in fact, even cancer can cause chest pain!
This is why this troubling symptom should always be investigated to rule out serious causes.
“Various risk factors must also be considered when evaluating chest pain,” says Waqar Khan, MD, who’s been providing state-of-the-art cardiology services to the Houston area for over 20 years, and is author of “Be Heart Smart: Understand, Treat, and Prevent Coronary Heart Disease.”
“Risk factors that are associated with coronary heart disease include diabetes, high cholesterol, family history of heart disease, history of smoking and high blood pressure,” continues Dr. Khan.
“A patient with two or more than two of these risk factors would certainly need an EKG and further workup to diagnose coronary heart disease or heart attack.”
Additional Risk Factors for Coronary Artery Disease
- Untreated sleep apnea
- Obesity and even moderate overweight, especially an apple shaped body
- Diet high in processed food, especially trans fats
- Excess dietary sodium
- Poor stress management
- Sleeping more than nine hours/night
- Sleeping fewer than six hours/night
- Insomnia
- Lack of exercise
- Sitting too much

Waqar Khan, MD, has a private practice and serves as an affiliate faculty member at Baylor College of Medicine in Houston, TX. Amazon.com/Be-Heart-Smart-Understand-Coronary/dp/1732268606
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}